
Abstract
Introduction
Acute mastoiditis (AM) is a suppurative infection of the m12OM), occurring in 1 case in 400 patients with AOM and dropping from 20% to 0.4% cases after the introduction of the routine use of antibiotics in AOM treatment.1,2 The incidence in the general population is 0.6 to 4.2 cases per 100,000 children per year. 2 The AOM complication rate decreased with antibiotic usage by half, but the persistence of these complications still occurs. 3 This may be connected to the increase of bacterial resistance, secondary to the routine use of antibiotics and pneumococcal vaccines, and to the “follow up” policy proposed by some national AOM guidelines. 4
AM is most common in childhood, due to anatomical, immunological, and infectious factors. The mastoid process in children is made of bony trabeculae, which are significantly thinner than those in adults, and the entrance to the mastoid air cells is much smaller than in adulthood, which leads to a longer retention of purulent content and increases the risk of spreading infection from the mucosa to bone walls. 5
Complications of mastoiditis can be life-threatening and require effective and prompt intervention. The dilemmas that the surgeon is facing when dealing with extracranial or intracranial complications would be the indications for surgical treatment, the best timing of surgery or the choice of the surgical procedure. Therefore, we performed a review of all pediatric patients with AM and its complications admitted to the university center over a 10-year period and tried to identify risk factors associated with complications. The analysis refers to the period before the obligatory pneumococcal vaccination.
Patients and Methods
A retrospective case review was conducted at the University Clinic for Otorhinolaryngology. The analysis included electronic databases of patients younger than 18 years old admitted with A diagnosis of AM in the period from January 2008 to March 2018. A total of 121 patients were identified using The International Classification of Diseases 10th edition codes for AM. Patients presenting with AM due to an underlying cholesteatoma and tuberculous otitis media were excluded. The patients’ data included demographic information, duration of symptoms and use of antibiotics before admission, and the type of complication related to AM. Patients were categorized into 4 age groups (0-1 group, 2-4 group, 5-10 group, and above 11 years group). Complications of AM were divided into extracranial (subperiosteal abscess, facial palsy, acute petrositis, labyrinthitis, and Bezold’s abscess) and intracranial (meningitis, venous thrombosis, cerebral abscess, and otitic hydrocephalus). The review included data from laboratory, imaging and culture results, surgical intervention(s), and antibiotic treatment.
All data were analyzed using SPSS 20.0 (IBM corp., Armonk, NY) statistical software. Statistical tests were used to perform the following analysis: chi-square χ2-test, Mann–Whitney U test, Student’s t test, Kruskal–Wallis H-test, and F-test. All P values less than .05 were considered significant.
Results
Of the 121 patients identified with AM, 70 were male (57.9%). The mean age was 3.7 ± 3.8 years (range 0-18 years) and 72% were from 0 to 4 years old, dominantly under 2 years (60%). The mean duration of symptoms was 5.4 ± 5.1 days and 59.5% of patients used antibiotic therapy (dominantly third-generation cephalosporins—37.5%) before hospitalization. A computed to-mography (CT) scan was done in 44.6% of patients with AM. Patients with suspected intracranial complications underwent CT and magnetic resonance (MR) imaging in 5% of cases. Figure 1 shows the CT scan of the temporal bone in a 13-year-old girl with Bezold’s abscesses as a complication of AM caused with group A streptococcus.
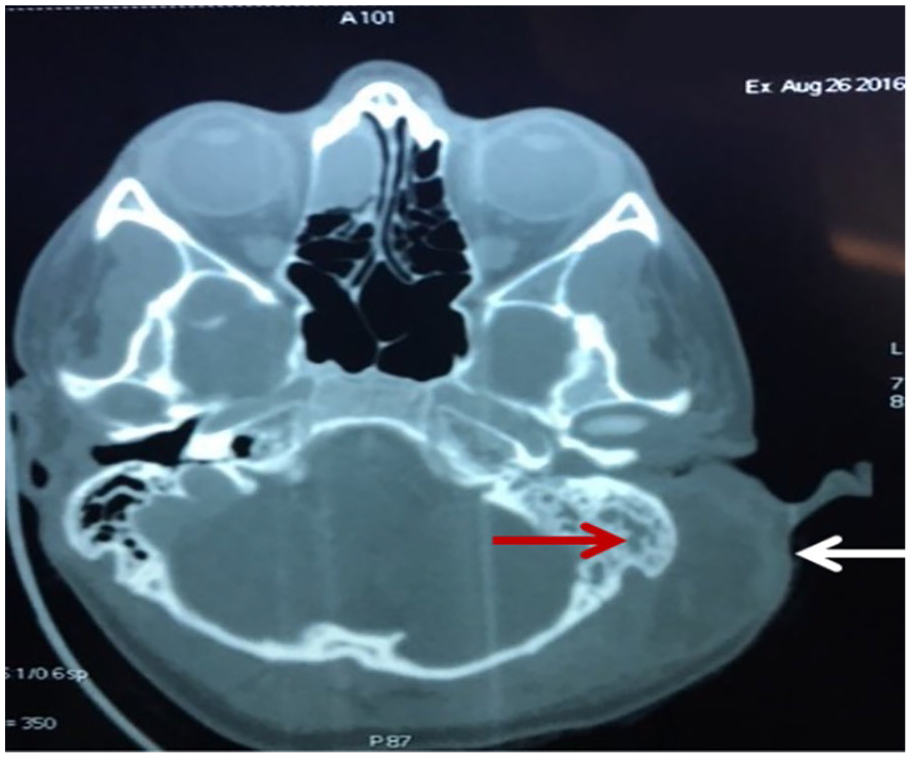
Axial CT scan shows left sided acute mastoiditis (red arrow) with apical erosion of mastoid and exteriorization of the infection into the neck (white arrow) with a forming Bezold’s abscess.
From the total of 121 children with AM, 115 (95%) patients underwent surgery, of them 16 patients had revision surgery, and 6 patients (5%) underwent conservative treatment. Most patients (95%) with AM were surgically treated within the first 48 hours after hospitalization. The most common treatment was insertion of ventilation tubes (N = 80, 69.6%), then insertion of ventilation tubes with mastoidectomy (N = 22, 19.1%) and the rarest treatment was insertion of ventilation tubes with mastoidectomy and incision and drainage of abscess (N = 13, 11.3%). Two patients underwent radical tympanomastoidectomy as a salvage treatment after no improvement after the first treatment—mastoidectomy and insertion of a ventilation tube—due to intracranial complication. Table 1 shows the type of surgery.
Surgical Treatment of Patients With Acute Mastoiditis With or Without Complication.
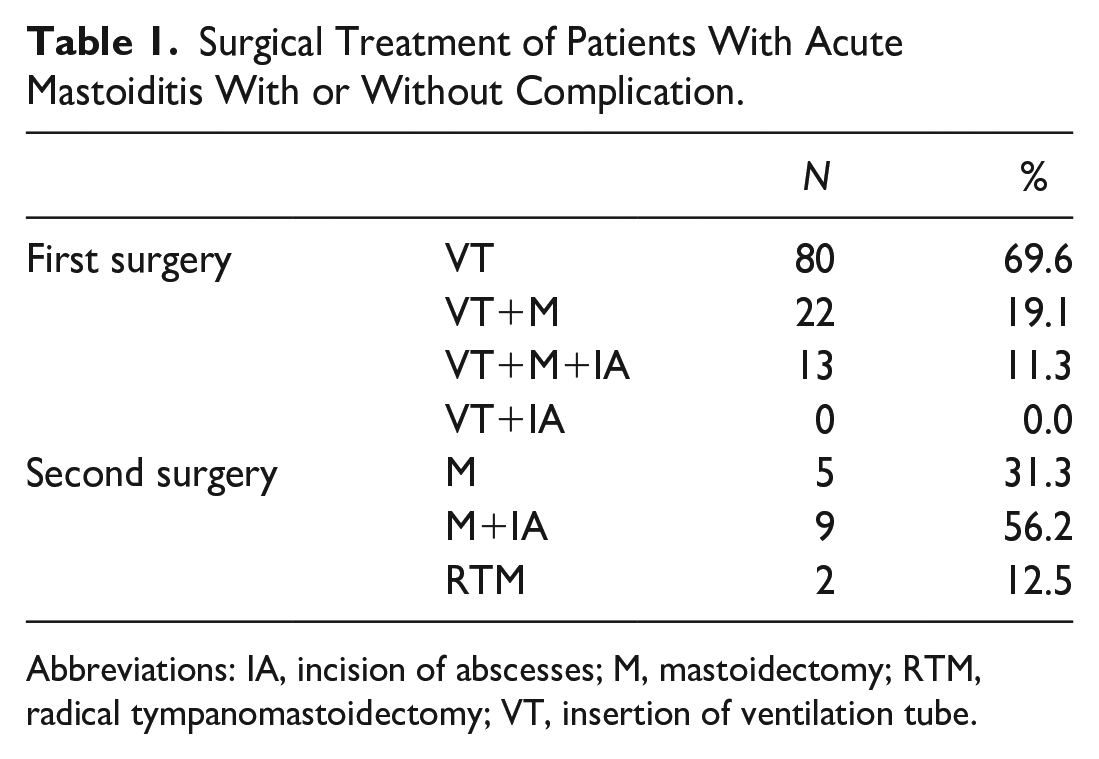
Abbreviations: IA, incision of abscesses; M, mastoidectomy; RTM, radical tympanomastoidectomy; VT, insertion of ventilation tube.
Streptococcus pneumoniae was the dominant isolated pathogen in patients with AM, as well in patients with AM with complications (Table 2). Both patients with severe meningoencephalitis had not been vaccinated and had a noninvasive serotype S. pneumoniae (serotype 3 and 11A) infection.
Microbiological Analysis Results of our Patient Samples.
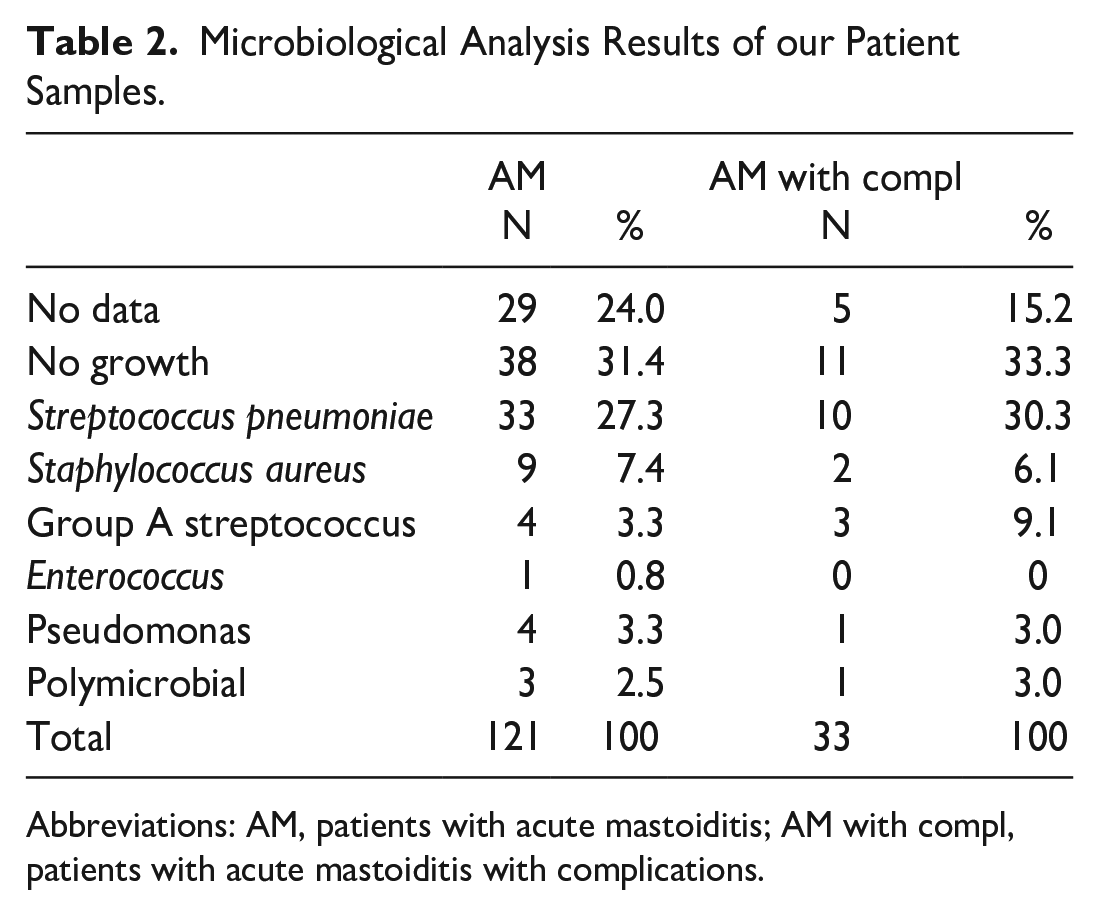
Abbreviations: AM, patients with acute mastoiditis; AM with compl, patients with acute mastoiditis with complications.
The most common initial intravenous antibiotic treatment in patients with AM was a monotherapy with ceftriaxone (76.5%) or a combination of ceftriaxone with metronidazole (17.4%) plus vancomycin in patients with intracranial complications.
From the total group of patients with AM, 33 (27.3%) of them had 1 (N = 30, 24.8%) or 2 complications (N = 3, 2.5%) of AM. Each complication was considered as a separate event and the analysis included 36 events. One patient had meningoencephalitis and otitic hydrocephalus, one had acute petrositis and meningitis and one had sigmoid sinus thrombosis and a subperiosteal abscess. Figure 2 shows the distribution of complications of AM according to types and ages. The most common complication was a subperiosteal abscess (N = 25, 69.4%), dominantly in patients under 4 years old. All cases of facial palsy and acute petrositis were in children above the age of 10. There was a significant difference between age group and occurrence of complications (P = .001; Table 3). We studied the immune status of all children with intracranial complications and all of them were immunocompetent.
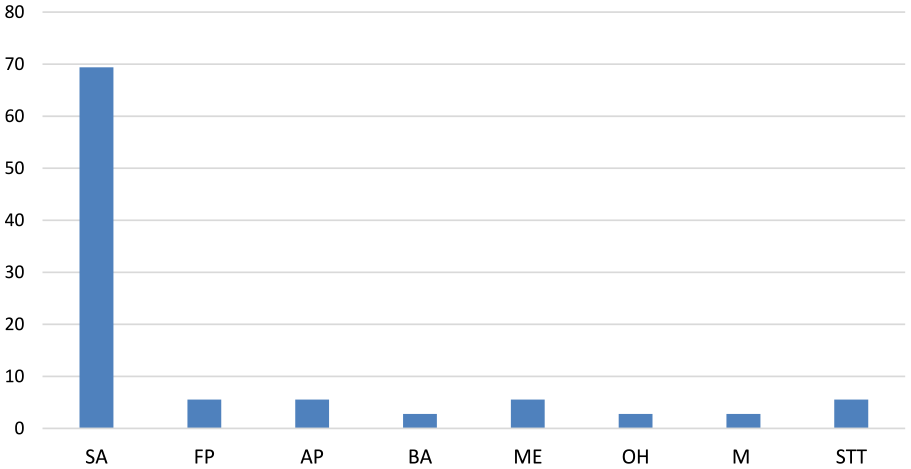
Distribution of complications of acute mastoiditis.
Age and complications (χ2 = 16,739; P = .001).
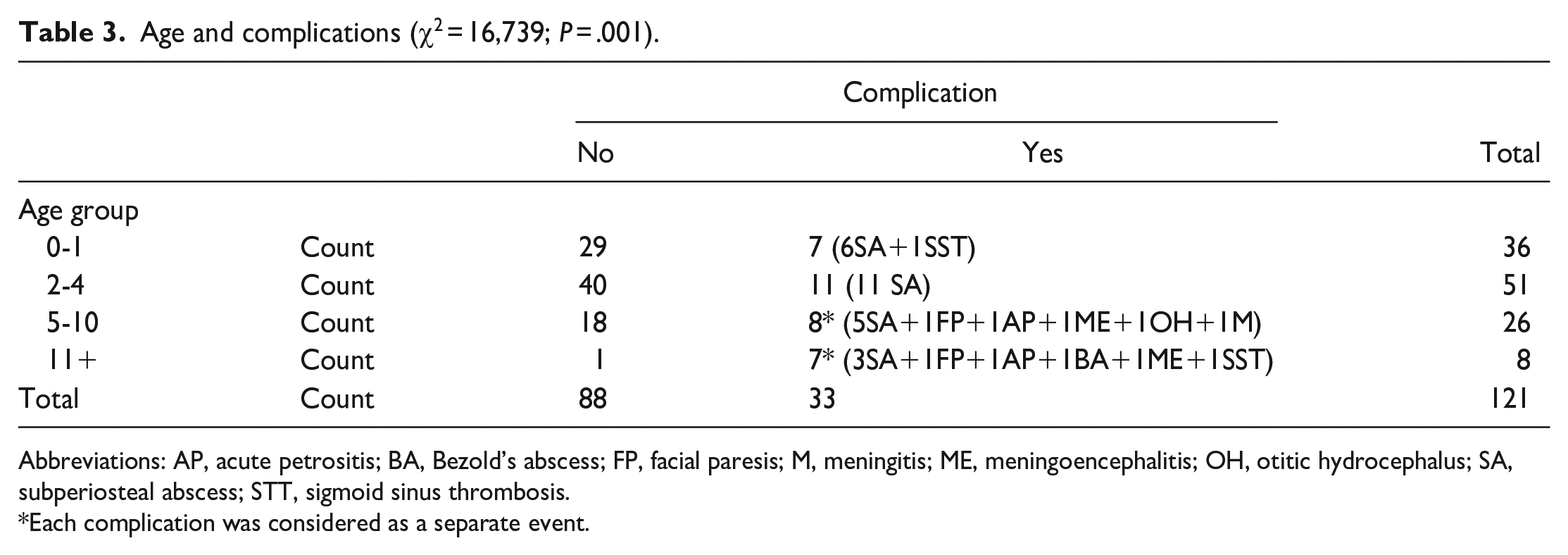
Abbreviations: AP, acute petrositis; BA, Bezold’s abscess; FP, facial paresis; M, meningitis; ME, meningoencephalitis; OH, otitic hydrocephalus; SA, subperiosteal abscess; STT, sigmoid sinus thrombosis.
Each complication was considered as a separate event.
Females had complications more frequently than males (P = .035). The mean duration of symptoms in patients with complication of AM was 6.3 ± 6.2 days and there was no significant difference between durations of symptoms in patients with or without complications of AM (P = .119). There were no significant differences in C-Reactive Protein (CRP; P = .373) and leukocyte count (P = .124) in patients with or without complications (Figure 3).
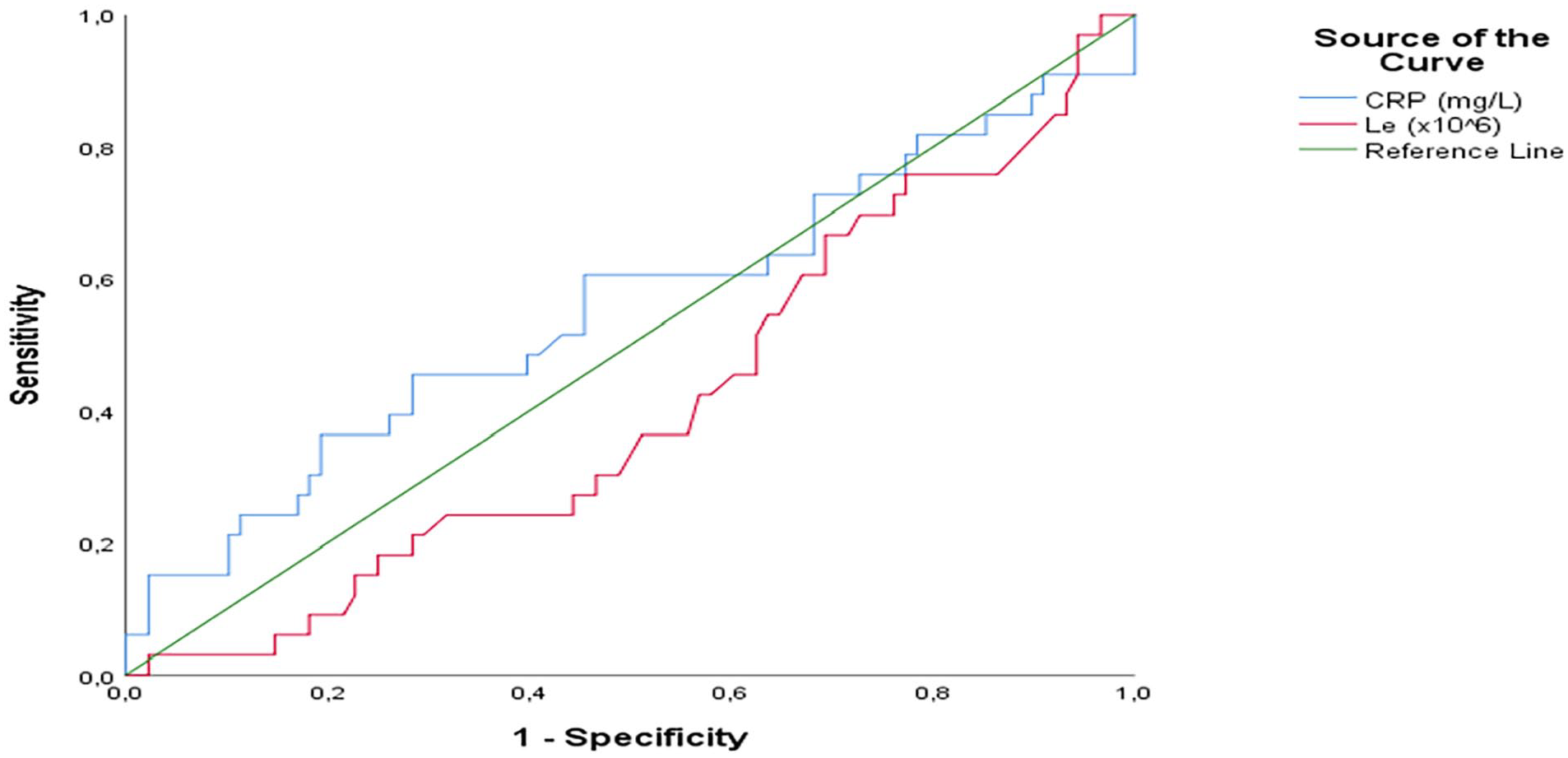
Curve for the sensitivity and specificity of CRP and leukocytes values.
Tube implantation was the first surgery in most cases (69.6%). The most common second surgical treatment was a mastoidectomy with (N = 8) or without (N = 4) the incision and drainage of abscesses. Intracranial complications were presented in 2 patients and a radical tympanomastoidectomy was performed as the second surgical treatment. One 13-year-old girl with acute petrositis was treated with long-term antibiotics because her parents refused surgical treatment for her, and she made a complete recovery. All patients with facial palsy underwent a mastoidectomy as well. Sigmoid sinus thrombosis (STT) was detected in 2 patients and both underwent a mastoidectomy with intensive antibiotic treatment without anticoagulants. A neurosurgical intervention (ventriculoperitoneal shunt) was performed in only 1 patient, due to otitic hydrocephalus.
A total of 22 (66.7%) patients with complications of AM were treated with antibiotics before hospitalization, but there was no significant difference in the number of patients who were treated with antibiotics and had or did not have complications of AM. In the group of patients who were treated with antibiotics before hospitalization, there was no significant difference in the type of antibiotics before hospitalization and occurrence of complications (P = .326).
There was a significant difference in the duration of hospitalization between patients with complications and those without (P < .001). In addition, there was a significant difference in the duration of antibiotic therapy in patients with and without complications (P < .001).
Discussion
In our study, we included 121 children. The average age of children with AM was 3.7 years (range 0-18 years), and 72% of children were younger than 4 years. Data from the literature show that AM in children is more common in boys. A retrospective study by Quesnel et al. showed that 57% of 188 children with AM were male, with a mean age of 15 months (range from 3 weeks to 15 years). 6 Favre et al. published similar percentages; out of a total of 2061 children with AM 1183 (57.4%) were male. 7
Almost two-thirds of our patients (59.5%) were on antibiotic therapy before hospitalization, mainly on third-generation cephalosporins (37.5%). Authors from Israel showed different data—36% of children with AM before hospitalization were on antibiotic therapy, primarily amoxicillin (78%), and almost the same data were published by authors from Portugal—every third child (33%) was on antibiotic therapy before hospitalization.8,9
In our research, CT scan was made in 44.6% of the children with AM, while CT and MR imagings were made in cases with suspicion of potential intracranial complications—5% of all children with AM. Indications of additional radiographic diagnostics in our study are slightly lower than those of the 39 studies where CT imaging was performed in an average of 68% of patients with AM (range 3%-100%). In the same review, an analysis of 9 studies found that MR imaging was performed in approximately 30% of children with AM (range 5%-100%). 10 There is no consensus when using CT or MR imaging in patients with AM. The diagnosis of uncomplicated AM is mainly made based on a clinical examination and, in most cases, there is no need for additional radiographic diagnostics. CT and MR imagings are necessary in cases where intratemporal, vascular, and intracranial complications are suspected. 11 Bone changes of the mastoid, intracranial, and extracranial abscesses are easily observed on contrast-enhanced CT imaging. In contrast, the use of MR imaging is necessary where there is a suspicion of intracranial complications, due to its higher sensitivity for the detection of extra-axial fluid collections and associated vascular lesions. 8 It should be noted that some authors believe that the use of a CT scan is necessary whenever there is a suspicion of AM in children to detect complications in time. In their opinion, the clinical examination is not sensitive enough for the early detection of AM complications, and since these are serious conditions that are often life-threatening, it is necessary to detect them as soon as possible to start adequate treatment in time.9,12,13 In our study, a CT scan was performed whenever we had children with high fever, disorder of consciousness, and high levels of inflammatory parameters or without improvement after the implantation of an aeration tube.
Immediately after hospitalization, we administered intravenous antibiotic therapy—ceftriaxone in 76.5% of cases, a combination of ceftriaxone and metronidazole in 17.5% of cases, and vancomycin in cases where intracranial complications were suspected. Only 6 (5%) patients were cured with conservative therapy and it is a significantly lower percentage compared to data from the literature, according to which in 3 out of 4 patients with AM, parenteral conservative therapy led to a complete cure.13,14 The remaining 115 (95%) patients in our study underwent surgery because the patient’s condition did not improve or worsened after conservative antibiotic therapy. Tube implantation was the first surgery in most cases (69.6%). In most cases, the second surgical treatment was a mastoidectomy with an abscess incision (56.3%). The treatment of children with AM is still the subject of academic discussion and differs from study to study depending on the clinical presentation, the presence of complications, and the experience of the surgeons. Due to the high frequency of S. pneumoniae in the etiology of AM and the susceptibility of this bacteria to third-generation cephalosporins, drugs of this group given parenterally are considered the drugs of choice in the initial treatment of uncomplicated cases. The susceptibility of pneumococci to penicillin is significantly lower, so oral penicillin therapy is often ineffective and may even predispose to complications. 11 There are significant differences in attitudes regarding the use of surgical treatment in patients with AM. 15 Thus, for example, the frequency of a mastoidectomy in the treatment of AM varies from 9% to as much as 88%. 10 However, in recent times, less invasive surgical treatment which includes a myringotomy with or without ventilation tube implantation, has been given increasing importance, especially in uncomplicated cases. Data from the literature show that the use of only conservative therapy (intravenous antibiotics) in the treatment of AM leads to a cure in almost 75% of cases, while the least invasive surgical treatment leads to the cure of almost 94% of patients with AM.13,14 The importance of a myringotomy with or without tube implantation is evidenced by the results of a recent study, which indicates that this procedure is effective in the treatment of complicated AM. The authors state that this surgical procedure together with the parenteral use of antibiotics and incision and drainage of abscesses is effective in treating AM with a subperiosteal abscess and that in most cases there is no need for a more extensive surgical procedure—a mastoidectomy. 16 A mastoidectomy is certainly indicated in cases of more serious complications of AM, in cases where CT imaging showed great destruction of the mastoid, and in cases where more conservative treatment did not lead to improvement. 11 The efficacy of a mastoidectomy in AM treatment is almost 100%, regardless of whether it is performed immediately after diagnosis or after unsuccessful conservative or less invasive surgical treatment. 14 In our study, we showed the necessity for a radical mastoidectomy in cases with intracranial complications of AM.
The most common complication in our study was a subperiosteal abscess, which occurred in every fifth child (20.5%) with AM. Loh et al. reported that the most common complication of AM is a subperiosteal abscess and occurs in 44.8% cases, which is twice as often as in our study. 15 Favre et al. also stated that the most common complication of AM is a subperiosteal abscess, but occurs in only 6.9% cases. 7 In our study we found that most cases of a subperiosteal abscess were in the age group between 2 and 4 years old. There is a statistically very significant correlation between age and occurrence of complications (P = .001) and they are significantly more common in younger children. There is also a statistically significant difference in the occurrence of complications in gender—complications develop much more often in girls (P = .035). Isaacson et al reported that the most common intracranial complication in children with AM is an intracranial abscess, while Favre et al. determined the most common intracranial complication to be intracranial thrombosis, which occurs somewhat more often than intracranial abscesses.7,17 However, none of our patients developed an intracranial abscess. Two patients developed serious meningoencephalitis, caused by pneumococcal middle ear infection and these cases were described in details.18,19 Otic hydrocephalus together with meningoencephalitis was recorded in 1 patient in the age group from 5 to 10. Sigmoid STT was found in 2 patients, 1 was in the age group from 0 to 1, and the other was in the age group 11 and older (Figure 2). In addition, we showed 1 child with a Bezold’s abscess as a complication of AM, a 13-year-old girl, who was treated for AOM in the primary health center for 1 month. It was caused by group A streptococcus and a radical mastoidectomy with abscess incision was performed. A Bezold’s abscess is a severe and very infrequent extracranial complication and rarely develops as a complication of acute coalescent mastoiditis. 20 Patients with a well-pneumatized mastoid are more likely to develop this complication, especially if they are immunodeficient. 21 Since the introduction of antibiotics, the incidence of this disease has significantly decreased, and from 1967 until today, less than hundred cases of a Bezold’s abscess have been published in English literature, of which only 4 were in children younger than 5 years of age. 22 Authors who, in their retrospective research, dealt with the topic of AM and its complications in children, with whose results we compared ours, did not report any case of a Bezold’s abscess, even though their studies included between 49 and 2061 children with AM.6,7,23
Microbiological analysis showed that the most common cause agent was S. pneumoniae (27.3%) in patients with AM, as well as in patients with AM with complications (30.3%). The results of 2 studies also show that the most common cause of AM in children is pneumococcus, which was isolated in 25.7% to 38% of cases.8,24 On the other hand, authors from the United Kingdom state that pneumococcus is a relatively rare cause of AM and was isolated in only 2% of patients, and they cite the high percentage of children vaccinated with pneumococcal vaccine as the most probable reason. 23 In our country, the pneumococcal vaccine has been obligatory since March 2018. Determining the effect of the vaccine on the possible reduction of incidence of AM and its complications will likely take a long time. We have already designed another study for postvaccinal period and have started to collect data. Some studies show that the pneumococcal vaccine has no influence on the incidence of AM. 4
The duration of symptoms of AOM, which would predict the appearance of complications, was analyzed and it was established that there was no statistically significant difference between duration of symptoms in patients with or without complication of AM (P = .119). In addition, complications of AM occurred regardless of the type of antibiotics that were used in the treatment of AOM.
The results of our study showed that there was no statistically significant difference in CRP and leukocytes values in patients with and without complications. Consequently, values of CRP and leukocytes might not be used as predicators of complications of AM. Other studies have, however, showed that there is a statistically significant difference in CRP and leukocytes values in patients with and without complications. Garcia et al. state in their article that a leukocyte count that was significantly higher in children with complications as well as a CRP value higher than 7.21 mg/dL at admission was associated with 1.9 times more risk of complications. 9
Our study was limited by a few factors. Firstly, it was a retrospective study and it was performed in a one department of tertiary clinical center. A significant number of children included in our research were initially treated in primary or secondary health care institutions, often with antibiotics that are not the first-choice drugs for AOM and AM—it is possible that the success of conservative therapy in these children would have been greater if initially prescribed antibiotic was adequate. Also, we did not analyze the otoscopic findings at the beginning of the treatment and compared it with the effectiveness of conservative or surgical treatment—we think that this correlation would be interesting and we will try to determine it in future studies. Future studies should include tertiary institutions in other regions and may yield more convincing data.
Conclusion
Almost all children with AM in our study underwent surgery because conservative antibiotic therapy was ineffective. The most common complication of AM in prevaccinal pneumococcal period was subperiostal abscess and the most common isolated pathogen was S. pneumoniae. Leukocyte count and CRP values cannot be used as predicators of complications of AM. Our future researches will determine whether the introduction of the mandatory pneumococcal vaccine in our country has led to a reduction in the incidence of AM and its complications.
Footnotes
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval for retrospective studies in our country is not required.
Consent Statement
We provided written consent of all patients/their legally authorized representative for including in this research.
Grant Number
Not applicable.