
Abstract
Laryngeal mucosa-associated lymphoid tissue (MALT) is an extra-nodal margin zone B-cell lymphoma (MALT lymphoma) and a low-grade malignant lymphoma with a low incidence, the etiology of the condition remains obscure, and the process of differential diagnosis poses a significant challenge, so it is easy to miss diagnosis and misdiagnosis clinically. The present article presents a clinical case study of a patient who was diagnosed with subglottic MALT lymphoma, which was associated with laryngeal amyloidosis. The patient underwent a successful treatment regimen comprising carbon dioxide laser and radiotherapy. In addition, the article provides an overview of relevant literature that can aid in the diagnosis and management of this rare disease. The study is expected to contribute to the existing body of knowledge on the treatment of subglottic MALT lymphoma and laryngeal amyloidosis.
Introduction
Mucosa-associated lymphoid tissue (MALT) lymphoma is a subtype of non-Hodgkin lymphoma that primarily affects the stomach, although it has also been reported in other organs such as the thyroid, breast, salivary glands, and orbit. 1 However, the incidence of MALT lymphoma in the larynx is exceedingly rare. Notably, since its first report by Diebold et al. 2 in 1990, over a 100 cases have been reported in China due to its large population base, while no more than 50 cases have been reported abroad. 3 Laryngeal MALT lymphoma is classified into 3 distinct subtypes, namely supraglottic, glottis, and subglottic, based on their anatomical location. Among these, supraglottic lymphoma is the most prevalent form, while instances of subglottic and glottic lymphomas are relatively rare. 4 Despite the progress made in the diagnosis, investigation, and management of these malignancies, significant controversy still remains over the differential diagnosis, auxiliary examination, and therapy of these conditions. This report presents a case study of MALT lymphoma with amyloidosis that occurred in the subglottic region of the larynx. It provides an overview of the latest advancements in the diagnosis and treatment of MALT lymphoma, drawing upon relevant academic research studies.
Case Report
A 79-year-old woman was admitted to the hospital for inspiratory dyspnea and chest tightness while performing daily activities for 1 year. And she also complained of occasional cough, less sputum, dry throat, heavy breathing, and a persistent hoarseness. Following a course of treatments, which included inhalation drug therapy, the initial impact was discernible. Nevertheless, the ensuing effects were not commensurate with the desired outcome. During a video laryngoscopy, bilateral ventricular bulges and a “subglottic mass” were discovered. She was admitted to the hospital for thorough physical examination: general condition and double check of video laryngoscopy (Figure 1), and it showed that the left ventricular band and vocal cord were thickened, and a raised mass was seen in the laryngeal vestibule and subglottic area. Cervical computed tomography (Figure 1) showed that the left ventricular cord and vocal cords were thickened, the laryngeal vestibule and the left anterior wall of the subglottic area were unevenly thickened, which was moderately strengthened, and the airway compressed. Preoperative pathological biopsy showed (Figure 2): lymphoid hyperplasia, combined with immunohistochemistry suspected mucosa-associated extra-nodal margin area B-cell lymphoma; unstructured subepithelial red staining, with multifocal calcification amyloidosis. Special staining result: Congo red (+) and immunohistochemical results:CD20 (diffuse +), CD79× (diffuse +), Bcl-2 (+, 80%), CD5 (+, 30%), CD23 (a little +), CD10 (a little +), Bcl-6(−), CD43 (+30%), Lambda (scattered +), Kappa (a little +), CK (epithelial +), CD3 (partial +), CD38 (−), CD138 (a little +), CD21(+), CvclinD1 (−), and Ki-67 index (10%). Rearrangement of the B lymphocyte gene: monoclonal hyperplasia. Because of financial limitations, the patient was incapable of receiving a positron emission tomography-computed tomography scan. Consequently, a fraction of the heightened mass was extracted through the use of carbon dioxide laser cautery. The extracted tissue was then forwarded for pathological analysis, which included immunohistochemistry. The pathological results were in alignment with the preoperative outcomes, and the conclusive diagnosis was identified as MALT with laryngeal amyloidosis.
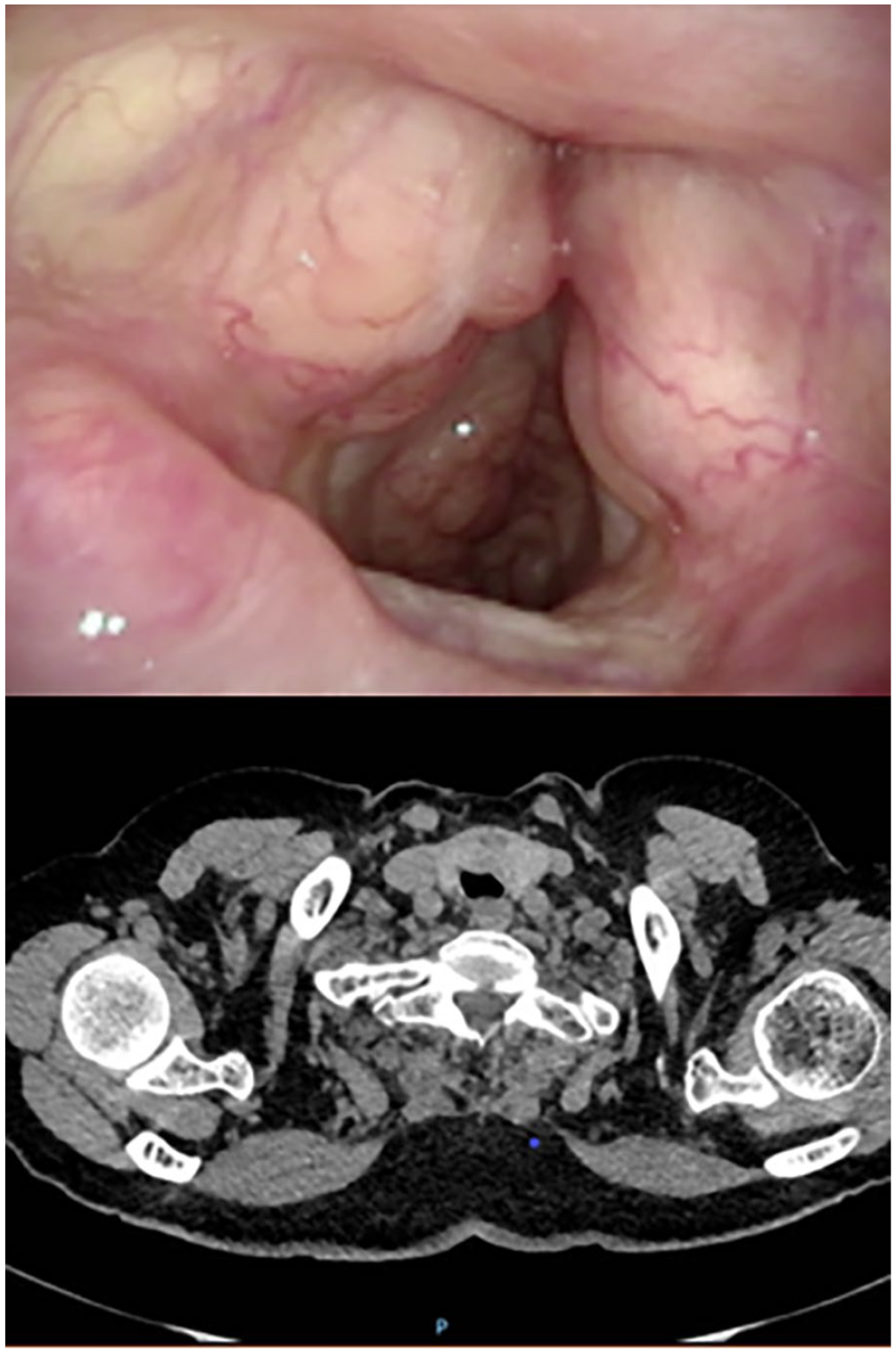
Evaluation of video laryngoscopy: Infiltration of subglottic regions with signs of chronic laryngitis.
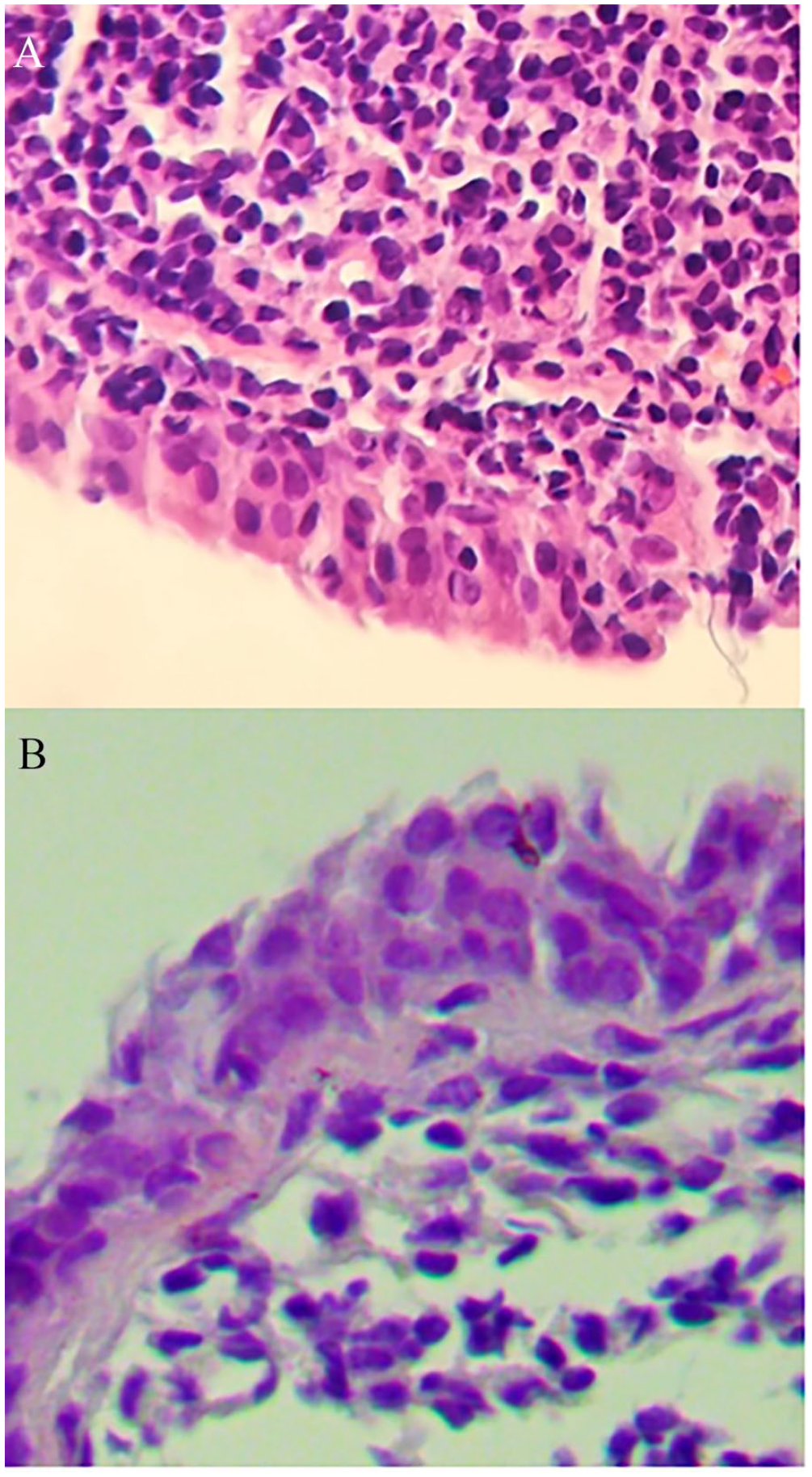
Laryngeal biopsy. (A) H&E. 40×: Extensive amyloid material deposition in the chorion. (B) Congo red.
After several multidisciplinary team discussions, the patient was planned to receive low-dose radiotherapy with a total dose of 24 to 30 Gy, 2 Gy every weekday for 3 weeks. The patient experienced a low dose of 30 Gy in a month. Following the course of treatment administered, the patient exhibited noteworthy amelioration in the symptoms of hoarseness and suffocation, with no instances of recurrence during a year and a half of posttreatment monitoring. Nonetheless, complete restoration of vocal clarity was not attained.
Discussion
Marginal B-cell lymphoma (MAL) is a type of lymphoma that has garnered significant clinical interest due to its increasing incidence worldwide. In a retrospective study of 200 patients diagnosed between 1973 and 2014, it was found that marginal zone lymphoma (MZL) accounted for 16.5% of laryngeal lymphomas.5,6 This percentage encompasses primary MALT lymphoma of the larynx, which is an exceedingly rare manifestation and accounts for less than 1% of laryngeal malignancies. 7 This study highlights the importance of considering the possibility of MZL in the diagnostic workup of laryngeal lymphomas, which may have implications for treatment and prognosis.
Studies indicate that laryngeal MALT lymphoma is more commonly diagnosed in males than females. Notably, a 2010 report by N.A. Siddiqui et al. 8 found that male patients were twice as prevalent as female patients. Likewise, a retrospective study conducted in England in 2015 9 demonstrated a male-to-female ratio of 1.6:1, while the ratio in China is even higher at 3.4:1. 10 The reasons for this phenomenon may be related to the trigger, one of which is smoking. Chronic Helicobacter pylori infection is a significant contributing factor to the development of gastric MALT lymphoma, 11 a subtype of non-Hodgkin lymphoma that affects the stomach in 80% of cases. 3 Some experts suggest that chronic inflammation caused by a lack of lymphoid tissue in the subglottic region may lead to the formation of lymphoid tissue. For laryngeal MALT lymphoma, the pathophysiology of association with Helicobacter pylori has not been accurately studied. In tracing the medical history of patients, there is often no prior gastric history, but smoking and family history may play a more significant role in the development of laryngeal MALT lymphoma.
The prognosis of laryngeal MALT lymphoma is impacted by its stage and classification, which is determined by the Ann Arbor criteria, based on the spread (I-IV) and systemic symptoms: (A) absent, (B) any of the following: fever for 1 to 2 weeks, weight loss, sweating, (E) local lesions that are not organs or tissues of the lymphatic system, (S) spleen damage. 12 Studies since 2000 have indicated that laryngeal lymphoma is primarily limited to the larynx, resulting in most cases being categorized as stage I or II. 13 In the present situation, the lymphoma was identified as being in the IE stage because there were no metastases detected in the cervical lymph node ultrasound. It is critical to distinguish between primary and secondary laryngeal Non Hodgkin Lymphoma (NHL) to develop precise treatment protocols. Primary involvement is best addressed with local radiation therapy, while systemic chemotherapy and immunotherapy are required for secondary involvement, which indicates a more advanced stage. 14
Clinicians may face a challenging task in diagnosing laryngeal MALT lymphoma due to its resemblance to squamous cell carcinoma, the most prevalent malignant tumor discovered in the larynx. Precise identification of squamous cell carcinoma remains a key priority for healthcare professionals as it is the most frequently occurring type of cancerous tumor in the larynx. In contrast, the symptoms of laryngeal lymphoma lack specificity, rendering its accurate diagnosis a formidable challenge. In a meta-analysis by P Zhao et al. 10 hoarseness (90.3%) was the most common symptom, followed by sore throat (33.3%), dyspnea (25.0%), and dysphagia (15.3%). Some patients have common symptoms of B-cell lymphoma (18.1%), such as fever and weight loss. The utilization of video laryngoscopy is highly beneficial in detecting polypoid masses in the glottis, which could potentially suggest the presence of laryngeal lymphoma. Nonetheless, these manifestations lack specificity and do not exhibit signs of ulceration. 15 As such, a precise diagnosis necessitates a comprehensive evaluation of pertinent imaging and a preoperative pathological biopsy.
For patients with MZL, imaging tests are crucial for a variety of reasons. Firstly, they help in making a preoperative diagnosis and distinguishing it from squamous cell carcinoma, NK/T-cell lymphoma, and other related diseases. They also help determine if any other body parts are affected. According to the research conducted by Zhao K et al., 16 17 F-fluorodeoxyglucose positron emission tomography/computed tomography (FFDG-PET/CT) can not only diagnose and stage the disease but also identify if there is any secondary involvement in other areas. However, some scholars believe that 17 FFDG-PET/CT may not be sensitive enough and, for diseases like lymphoma, and further bone marrow biopsy may still be necessary. 1
Obtaining a preoperative biopsy is essential in providing an accurate diagnosis for the disease’s distinct characteristics. An incorrect diagnosis may result in a delay in treatment or an improper operation. To ensure precision, multiple biopsies may be required for confirmation. MALT lymphoma is recognized through positive immunochemical markers CD19/20/22/79, while negative markers include CD5/10/23/BCL-6 and cyclin D1. 18 The patient’s positive CD20 and CD79 results led to a diagnosis of MAL. Additionally, pathology results confirmed a diagnosis of laryngeal amyloidosis, characterized by the extracellular deposition of protein-like substances. The presence of subepithelial extracellular deposits of amorphous and homogeneous eosinophilic material without structure confirmed the diagnosis. It’s important to note that laryngeal amyloidosis is a rare condition, with some cases potentially linked to lymphoproliferative diseases originating from lymphoid tissue associated with mucosa. 18
According to a study conducted by Velasco LC, 19 a patient who had MALT lymphoma along with laryngeal amyloidosis was treated with 18 radiotherapy sessions and experienced an improvement in their voice. In most cases, patients with non-Hodgkin larynx lymphoma have a positive prognosis. Early-stage disease can often be cured with chemotherapy or radiation therapy alone. However, for patients with advanced-stage disease, a combination of chemoradiotherapy is typically used, and it has been proven successful in controlling the disease. 9 In cases where there is laryngeal obstruction or heavy bleeding, surgical removal of the mass is becoming more common, while low-dose radiation therapy remains an option for curative cases. 15
Conclusion
Laryngeal MALT lymphoma with amyloidosis, although uncommon, is associated with a positive prognosis when treated early. As such, timely detection and accurate diagnosis are crucial factors in ensuring successful outcomes for patients. The present case exhibits promising outcomes with the use of laser and radiotherapy, thus providing valuable insights and methodologies for otolaryngologists to manage similar pathologies in the foreseeable future.
Footnotes
Data Availability
The data for the case were accessed through the electronic medical record. They are not available for readers to review as they contain confidential patient health information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Submission Statement
This article is original and has not been submitted elsewhere in part or in whole.
Ethical/Consent Statement
Written informed consent was obtained from the patient for the publication of this case report.