
Abstract
Middle ear meningiomas (MEMs) are rare tumors that can present with nonspecific symptoms, posing challenges in diagnosis and management. This case report focuses on a middle-aged female patient who was misdiagnosed with secretory otitis media for 5 years. However, further evaluation through computed tomography imaging and subsequent pathologic biopsy revealed the presence of a MEM. The patient underwent surgical and gamma knife resection of the tumor and follow-up examination after 1 year showed no signs of recurrence. This case report highlights the importance of considering meningiomas in the differential diagnosis of middle ear pathologies and the need for careful preoperative planning for optimal outcomes. Overall, this case demonstrates that correct diagnosis and appropriate treatment can lead to successful management of MEMs.
Introduction
Meningiomas are typically benign tumors that arise from the meninges, the membranous layers that cover the brain and spinal cord. 1 However, meningiomas can occur in a variety of locations throughout the central nervous system, including the middle ear. 2 Middle ear meningiomas (MEMs) are rare tumors that are difficult to diagnose, and often present with symptoms that are similar to those of other middle ear pathologies. 3
MEMs can be classified as primary or secondary.4,5 Primary meningiomas originate from the meninges that cover the middle ear structures, while secondary meningiomas arise from distant sites and metastasize to the middle ear. 6 The majority of MEMs are primary, and occur more commonly in women than men. 5 The clinical presentation of MEMs varies, but patients may experience symptoms such as hearing loss, tinnitus, ear fullness, otalgia, and facial weakness. 2 Diagnosis can be challenging, as the symptoms of MEMs are often nonspecific and may mimic those of other middle ear pathologies. Imaging studies, such as computed tomography (CT) and magnetic resonance imaging (MRI), are essential for diagnosing MEMs and assessing their extent.
Treatment of MEMs typically involves surgical resection, although the location and size of the tumor may influence the surgical approach. 7 Radiation therapy may be considered in cases where complete resection is not feasible or in patients with recurrent tumors. 8 However, it is easy to be misdiagnosed as inflammatory disease because of the low incidence rate or lack of specific symptoms. Here, we report a case of MEMs that was misdiagnosed with recurrent secretory otitis media via CT and discuss the clinic pathologic and radiological features that distinguish meningiomas from other temporal bone pathology.
Case Presentation
Clinical History
A 52-year-old female patient presented to the Oto-rhinolaryngology outpatient clinic with complaints of left ear hearing loss for 5 years. She also reported some specific ear symptoms such as aural fullness. There was no history of otalgia, otorrhea, or vertigo. She visited Union hospital, Tongji medical college, HuaZhong University of Science and Technology for evaluation and treatment. Her medical history revealed that the she had a ventilation tube application 4 years ago. Three months later the tube was removed because of the improvement of symptoms. These symptoms recured over a 1-year period. The patient presented to clinic again with the same complaints and audiological finding. Consequently, myringotomy and grommet tube insertion were performed once again, but the effect was limited. Then she came to our outpatients for further treatment. A new audiological assessment was performed and revealed a mix hearing loss (Figure 1A and B). Tympanogram demonstrated type B for the right ear and type A for the left ear (Figure 1C). Otoscopic examination revealed an intact tympanic membrane.
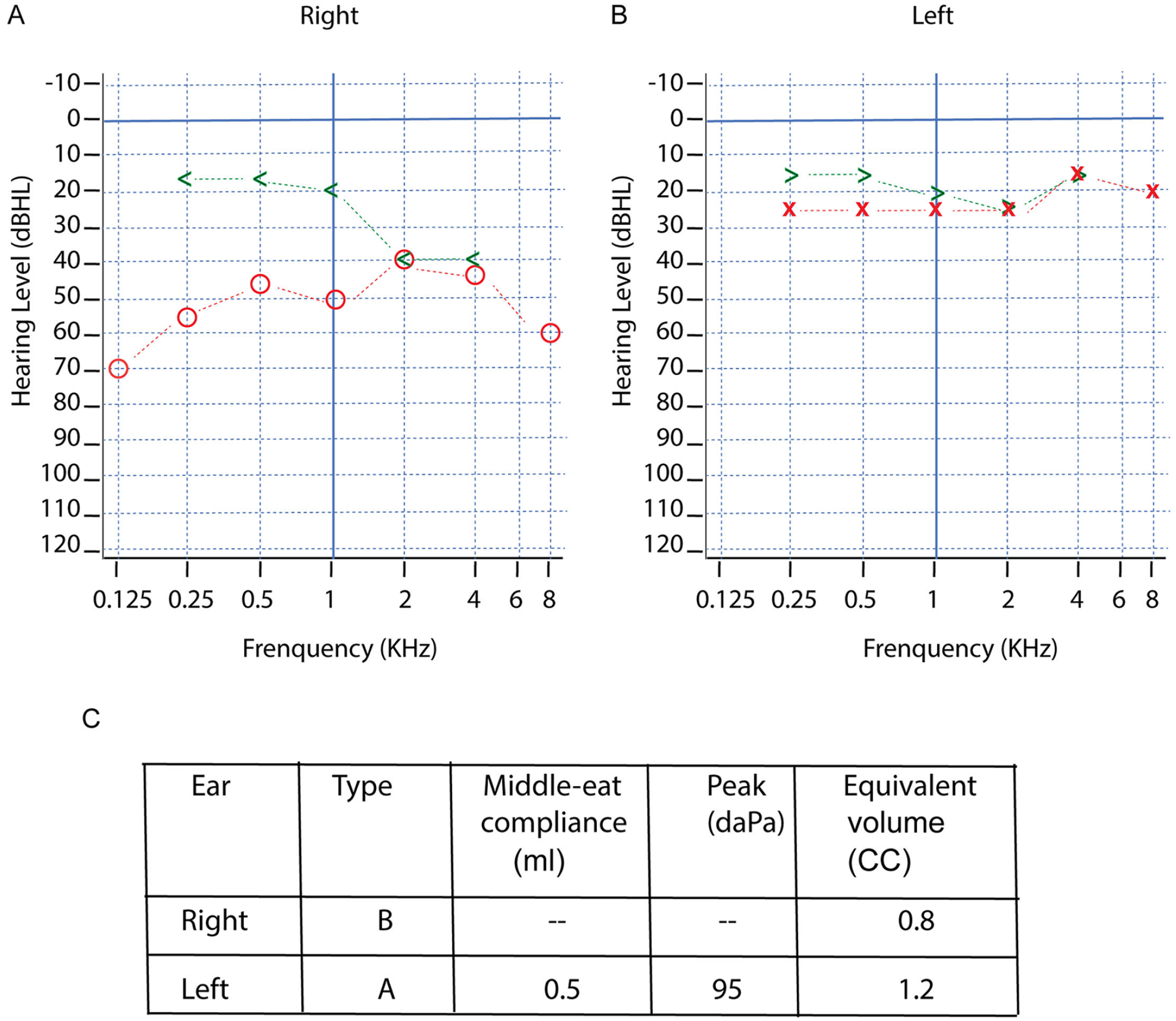
Audiogram show a mixed hearing loss for the right ear. (A) both air and bone conduction are in the abnormal range, with the air–bone gap generally greater than 20 dB. (B) Audiogram demonstrates both the air and bone conductions are normal for the left ear. (C) Tympanogram of the right ear showing a type B pattern with a compliance of 0.5 ml, peak pressure of 95 daPa, and volume of 1.2 ml.
Imaging
On CT imaging, a soft-density shadow is visible in the right tympanic cavity, surrounding the ossicles (Figure 2A). In addition, a slightly high-density strip-shaped shadow was observed in the right middle and posterior cranial fossa, which closely related to the right tentorium cerebelli and skull base dura mater. The lesion encircled the right cavernous sinus area and compressed the right margin of the brainstem and right temporal lobe in MRI (Figure 2B-D). The 3D reconstruction of the CT reviewed a tumor occupying the middle ear and mastoid cavity with intact ossocular chain and dural and sigmoid sinus plates. The maximum cross-sectional area was approximately 52 mm × 28.2 mm and protruded downward near the sphenoid sinus (Figure 2E-G).
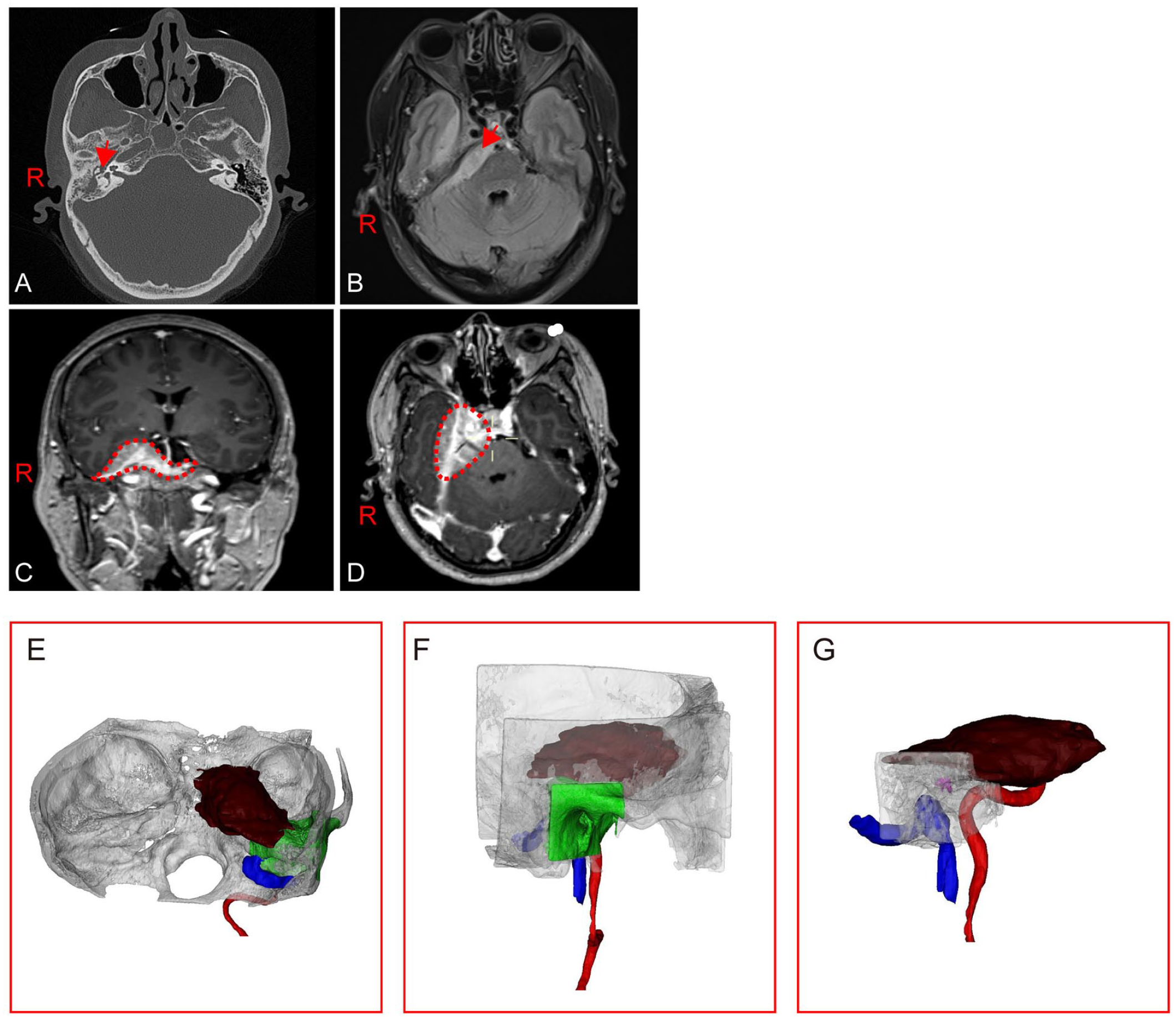
Imaging of the brain and temporal bone before surgery. (A) CT in the axial plane demonstrates a soft tissue mass in the right middle ear and mastoid cells (Red arrow show). (B) Axial T1-weighted MRI shows a slightly high-density strip-shaped shadow in the right middle and posterior cranial fossa. (C and D) Adjacent dural enhancement can be seen involving the middle fossa. Red dash line shows the tumor. (E, F, and G) show the 3D reconstruction of the CT.
The ossicles are clear and interruption of the continuity of the temporal bone is seen in the right temporal lobe (Figure 3A). Large patchy high signal intensity with unclear borders on flair imaging. No obvious abnormal enhancement is seen on the right temporal lobe on contrast-enhanced scanning. There is a slight accumulation of fluid in the right anterior pool of the pons and the infratemporal fossa. The right side of the pons is slightly compressed, and there is no obvious abnormal signal in the remaining brain tissue (Figure 3B-D).
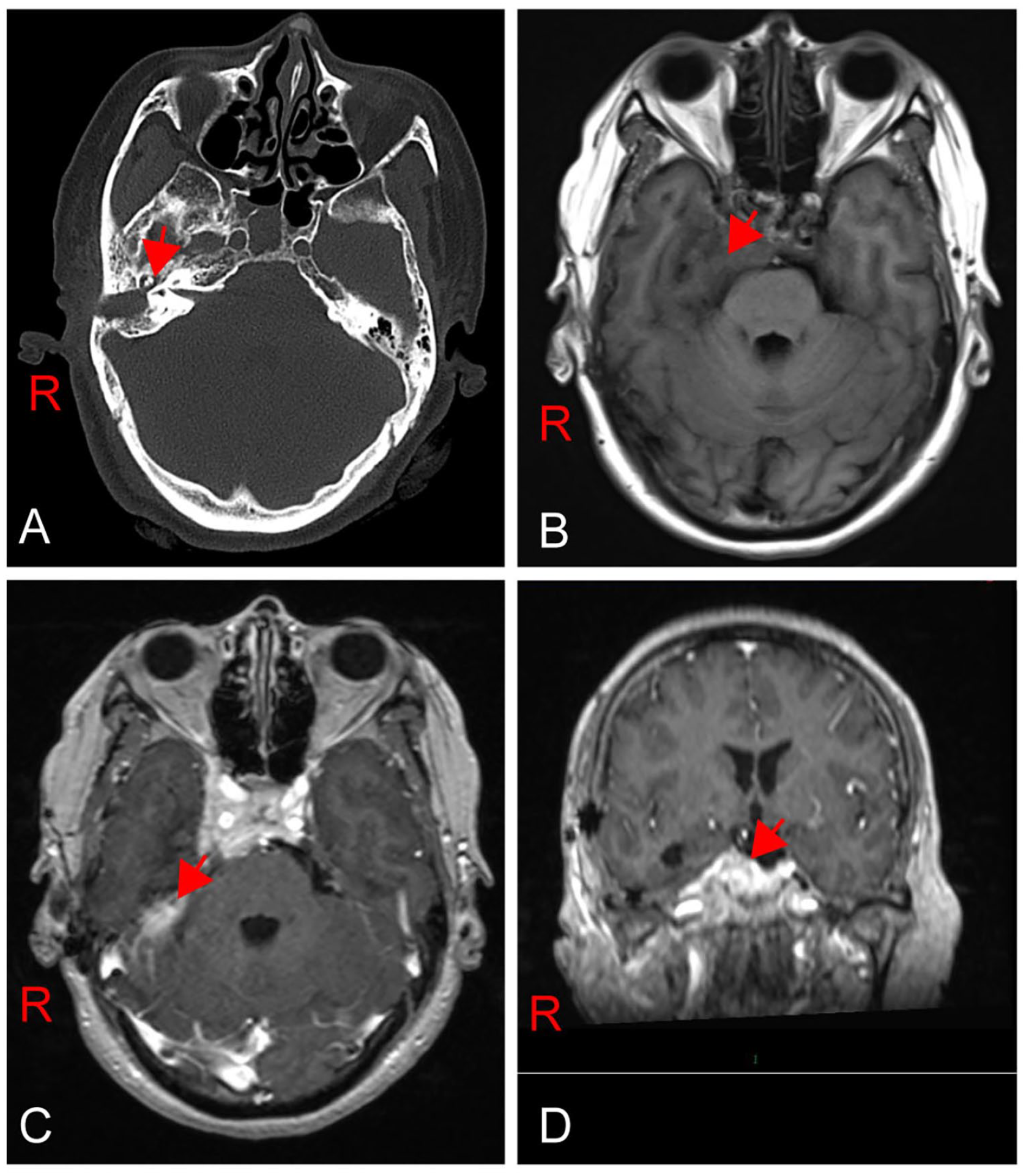
Imaging of the brain and temporal bone after surgery. (A) Ossicles are clearly shown in the CT (red arrow show). (B, C, and D) large, patchy, high signal intensity with unclear borders on flair imaging. No obvious abnormal enhancement is seen on the right temporal lobe on contrast-enhanced scanning.
Treatment
In February 2022, a decision was made to perform an exploratory tympanotomy to obtain a better specimen for biopsy. It was performed via a post auricular approach. The tumor was grossly and totally resected and subjected to histopathological analysis. The biopsy revealed a WHO grade 1 meningothelial meningioma. This was confirmed by immune histochemistry, namely epithelial membrane antigen (EMA), Somatostatin receptor type 2 (SSTR2), Progesterone receptor (PR), D2-40 (Figure 4A–H). Consequently, the patient was rescheduled for a removal via a transotic approach. Three months after the operation, the patient was treated with gamma knife due to some residual in the sponge sinus. At her most recent follow-up, approximately 1 year following surgery, she was found to have no evidence of radiologic growth or worsening symptomatology.
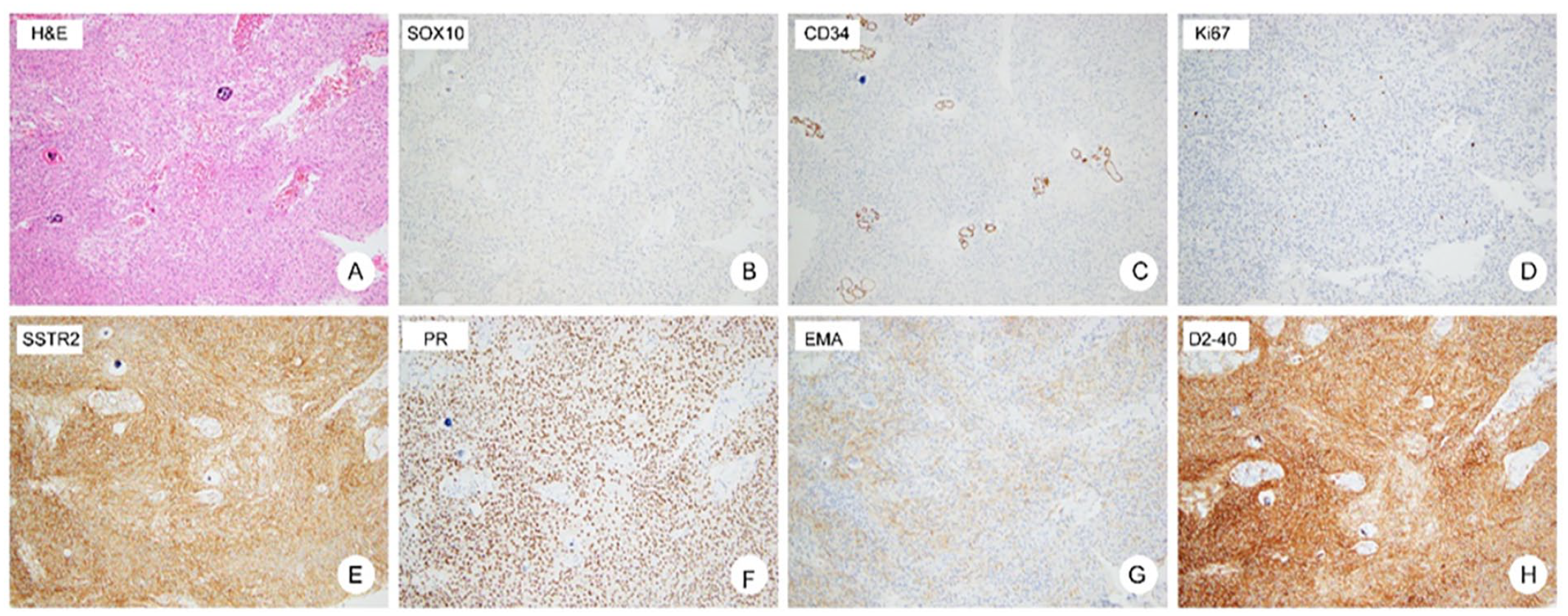
H&E staining of the tumor. (A) Tissue fragment from the middle ear and mastoid cavity shows a typical meningothelial whorl pattern with a polypoid growth pattern. (B–H) Tumor cells did not show the expression of SOX10, CD34, but demonstrated strong staining for EMA, SSTR2, PR, and D2-40. Ki-67 is less than 5%.
Discussion
In this case report, we describe a female patient with a MEM who presented with symptoms of ear fullness and hearing loss. The patient underwent successful surgical resection of the tumor, and there was no evidence of recurrence 1 year later. This case highlights the challenges associated with diagnosing and managing MEMs, as well as the importance of early intervention for optimal outcomes.
MEMs are rare tumors that can present with a variety of nonspecific symptoms, such as hearing loss, tinnitus, and ear fullness. 9 In this case, the patient presented with symptoms of ear fullness and hearing loss, which prompted further investigation and the eventual diagnosis of a MEM. It is important to consider meningiomas in the differential diagnosis of middle ear pathologies, as early intervention can improve outcomes and prevent complications. Surgical resection is the preferred treatment for MEMs, and complete resection is associated with favorable long-term outcomes.1,10,11 The location and size of the tumor can influence the surgical approach, and careful preoperative planning is essential for optimal outcomes. Radiation therapy may be considered in cases where complete resection is not feasible or in patients with recurrent tumors. However, radiation therapy is associated with potential complications, such as radiation-induced ototoxicity and cranial nerve injury, and should be reserved for select cases. In this case, the patient underwent successful surgical resection of the most part of the tumor and gamma knife was used to deal with the invasion that involved into the cavernous fossa. There was no evidence of recurrence 1 year later.
The prognosis for patients with MEMs is generally favorable, with a low risk of recurrence and a good long-term outcome. However, regular follow-up and surveillance are necessary to detect any potential recurrence or complications.
In conclusion, this case report highlights the challenges associated with diagnosing and managing MEMs, as well as the importance of early intervention and careful preoperative planning for optimal outcomes. Surgical resection is the preferred treatment, and complete resection is associated with favorable long-term outcomes. Radiation therapy may be considered in select cases, but potential complications should be weighed against the potential benefits. Regular follow-up and surveillance are necessary to detect any potential recurrence or complications.
Footnotes
Author Contribution
H.Y.S. and Q.L.H. contributed to data curation; Y.J.H. contributed to validation; H.Y.S and W.B.C. contributed to writing—original draft; Y.J.H. contributed to writing—review and editing and was also was responsible for supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Open Project of Key Laboratory of Molecular Imaging (2021fzyx017).
Ethical/Consent Statement
Not applicable.
Grant Number and Data Availability Statement
All data generated or analyzed during this study are included in this published article.