
Abstract
Actinomycosis is common in the head and neck region but rarely occurs in the nasal septum. A 75-year-old male patient with an edentulous maxilla, hypertension, and diabetes developed actinomycosis confined to the nasal septum and showed mucosal necrosis and septal bony sequestration. The patient underwent surgery and medication therapy; this case was reported using endoscopic photographs and radiographs and a literature review was conducted to provide further context and understanding of the condition of the patient.
Introduction
Actinomycetes are anaerobic or microaerobic filamentous bacilli normally distributed in the oral cavity and gastrointestinal and urogenital tracts. They can cause a subacute or chronic suppurative granulomatous infection called actinomycosis when the mucosal integrity is disrupted and tissue oxygen concentration is low. Approximately 60% of all patients develop this infection in the cervicofacial region; actinomycosis is associated with trauma, diabetes, and dental procedures.1 -3
Actinomycosis rarely occurs in the paranasal sinuses and nasal cavity.4 -6 It can present characteristics similar to those of fungal balls inside the sinuses in a noninvasive form and progresses extensively by eroding the surrounding soft tissues or bones.
Actinomycosis confined to the nasal septum has rarely been reported in the English literature. Therefore, we report this rare case using endoscopic photographs and radiographs.
Case Report
A 75-year-old male patient visited our hospital, complaining of foul odor and bloody secretions while blowing his nose for the past 3 months. Other local symptoms, such as pain and nasal obstruction, or systemic symptoms, such as fever, myalgia, or weight loss, were not reported.
He was receiving medication for hypertension and was diagnosed with type 2 diabetes 1 year ago. In addition, he had been engaged in lifestyle modifications. The patient had no history of facial trauma or nasal surgery. The upper jaw had been edentulous for 2 years, and he had been using a complete denture.
Nasal endoscopy revealed defects in the anterior mucosa of the nasal septum on the right side, granulomatous changes, and lesions covered with yellow-green materials (Figure 1A). In the left nasal cavity, necrotic bone protrusion and granulomatous lesions were observed at the junction of the nasal septum and floor (Figure 2B). No abnormalities were observed in the oral mucosa.
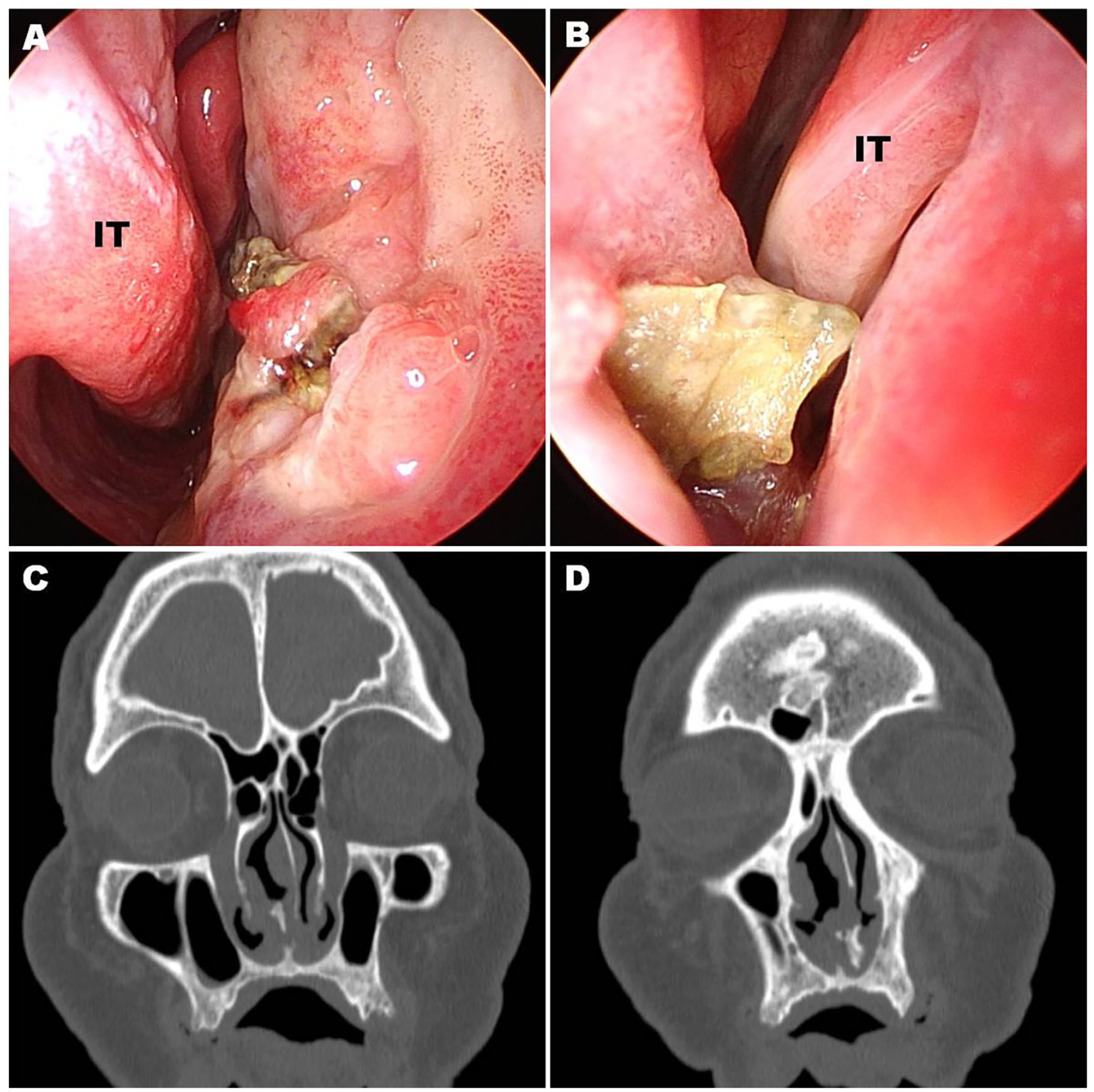
Endoscopic view and radiological imaging of actinomycosis of the nasal septum (IT = inferior turbinate). A yellow-green material covered the septal lesion on the right side of the nasal cavity through defects and granulomatous changes in the septal mucosa (A). Sequestration of the necrotic nasal bony septum protruding to the left nasal cavity (B). Coronal computed tomography shows a soft tissue density lesion in the anteroinferior region of the nasal septum and bony sequestration (C and D).
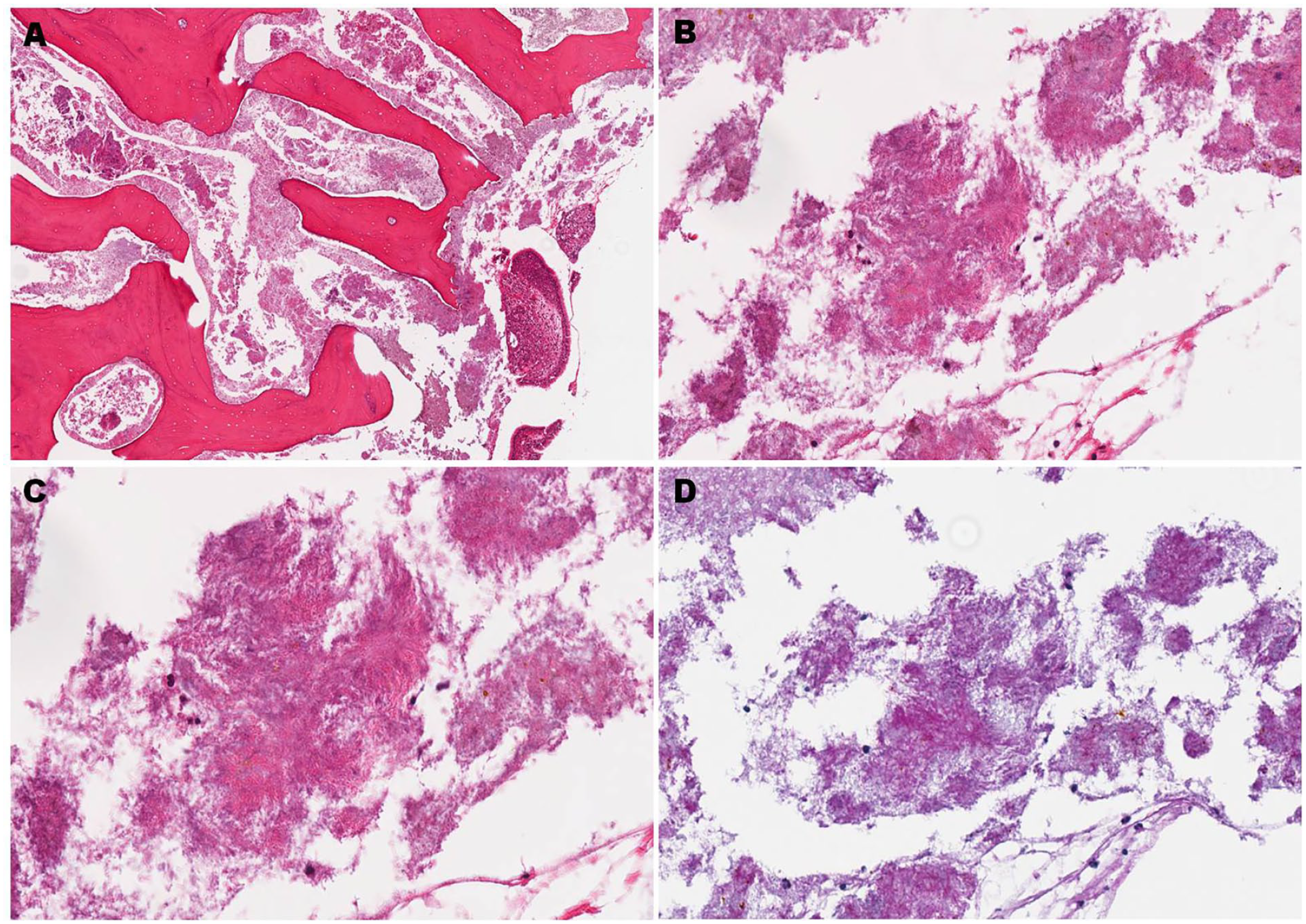
Pathological findings of actinomycosis of the nasal septum. Diffuse colonies of organisms with filamentous hyphae and sulfur granules within the bone (A, hematoxylin-eosin, magnification: ×4). Higher magnification illustrates actinomycotic granules with filamentous structures (B and C, magnification: ×200 and ×400). Positive Periodic acid-Schiff staining of the same area as that in B (D, magnification: ×200).
The paranasal sinus computed tomography (CT) re-vealed thickened soft tissue lesions in the anteroinferior part of the nasal septum, along with bony erosion and calcification, suggestive of sequestrated bone (Figure 1C and 1D). Magnetic resonance imaging (MRI) revealed an ill-defined lesion corresponding to the region shown on the CT scans, which had an intensity similar to that of the surrounding nasal mucosa on T1- and T2-weighted scans.
A biopsy of the greenish-yellow material and granulation tissue from the right nasal septum revealed colonies of organisms with filamentous hyphae and sulfur granules, leading to the diagnosis of actinomycosis (Figure 2). Endoscopic sinus surgery was performed under general anesthesia. Antibiotics for actinomycosis and oral hypoglycemic agents for diabetes were administered under strict control.
To preserve the normal septal mucosa, the sequestration of the bony septum protruding into the nasal cavity was carefully removed through the necrotic defects of the mucosa, and a part of the inflammatory granulation from the nasal floor was also removed. The lesions and surrounding areas were washed with saline. The symptoms completely resolved the day after the surgery.
Amoxicillin (1000 mg) and clavulanate (200 mg) were intravenously administered thrice daily for 5 days during hospitalization. After discharge, 750 mg of oral amoxicillin and 125 mg of clavulanate were administered thrice daily for 21 days. No gastrointestinal side effects such as diarrhea developed during the administration period, and the treatment was discontinued after confirming that the primary lesion at the surgical site had completely disappeared as shown on endoscopic and radiologic examinations. The patient had a 3-mm nasal septal perforation after surgery but remained asymptomatic. He did not develop any other problems and was followed up for 32 months, without recurrence.
Discussion
Actinomycetes are normally present in the oral cavity and oropharynx, with higher prevalence in tonsil crypts, gingival crevices, periodontal pockets, and dental plaques. Certain factors predispose individuals to actinomycosis, such as oral mucosal damage, maxillofacial surgery/trauma, infection by other bacteria, diabetes, radiation therapy, and immunosuppression. Granulomatous pyogenic inflammation, abscess pocket, oroantral fistula, and mandibular osteomyelitis can occur in the head and neck area.1 -3,7,8
Diagnoses can be made using bacteriological cultures or histological examinations. Bacterial culture has a high failure rate, as the results can be affected by previous antibiotic treatment and the inability to follow strict anaerobic culture techniques. Histopathological examination showing gram-positive filamentous bacilli, basophilic centers with club-shaped structures, and sulfur granules has a diagnostic value.1 -3
CT scans may reveal soft tissue density in the paranasal sinuses, calcification inside the lesion, and destruction of the surrounding bone. However, these findings are not specific to the disease.4,5 On MRI, cervicofacial lesions with abundant granulation may exhibit low or intermediate signal intensity on T1 and T2 images. Central signal voids, which are characteristic of fungal sinusitis, can also be observed in some conditions.9 -12
Treatment involves surgical resection of infected tissues and long-term antibiotic therapy. Surgery is performed to relieve the initial burden by removing the necrotic and granulomatous tissues appropriately and to improve the anaerobic environment, which is important for successfully treating the infection since bacteria thrive in such conditions.1 -5
Conventional treatment involves administering high-dose penicillin intravenously for 2-6 weeks, followed by oral penicillin for 6-12 months. Amoxicillin/clavulanic acid, cephalosporin, and clindamycin can also be used, and the duration of medication may be shorter or longer depending on the condition of the patient.7,8,13
Actinomycosis in the nasal septum has rarely been reported in the English literature.11,14,15 In 1995, actinomycosis presenting with purulent discharge and a septal mass was reported in a 51-year-old male patient with human immunodeficiency virus infection. In 2020, a 36-year-old healthy man complaining of hyposmia was diagnosed with actinomycosis through radiological examination, which showed a mucocele in the bony nasal septum. However, no specific findings were observed on endoscopy. Hence, the patient was treated with amoxicillin 1500 mg/day for 4 months after surgery. In addition, an 84-year-old female patient with a history of immunotherapy for breast cancer with bone metastasis, diabetes, and hypertension was diagnosed with actinomycosis, which appeared as a nasal septal mass covered with normal mucosa. The patient was administered 500 mg of amoxicillin twice daily for 3 months after surgery in 2021.
None of the patients with septal actinomycosis, including the present patient, had a history of recent facial trauma or surgery, and the occurrence of this condition was not related to dental problems. Patients were diagnosed through histological examination, and they underwent medical and surgical treatments. During endoscopy, it was observed that the sequestrum of the bony nasal septum was protruding into the nasal cavity on both sides of our patient. Bony sequestrum in cervicofacial actinomycosis is ob-served when the maxillofacial bones are extensively involved and may also occur when the mandible, maxilla, or frontal sinus is locally invaded.3,6,8,16,17 However, cases with similar conditions to this one have not been reported in the English literature.
We present the case of a 75-year-old male patient with diabetes, hypertension, and edentulous maxilla, who complained of foul odor caused by actinomycosis confined to the nasal septum. The infection resulted in mucosal necrosis, inflammatory granulation, and sequestration of the bony septum. The patient underwent surgery and received antibiotic therapy for 26 days. No recurrence occurred after 32 months of follow-up.
Footnotes
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a VHS Medical Center Research Grant, Republic of Korea (grant number: VHSMC 23040).
Ethical Approval
This study was approved by the institutional review board of Veterans Health Service Daejeon Hospital.
Statement of Informed Consent
The authors have obtained the patient’s informed consent.