
Abstract
The preoperative diagnosis of a paranasal epidermoid cysts (EC) is challenging and is frequently mistaken. We present the case of a patient who developed a swelling on the left side of the face. The clinical examination showed a fixed and poorly defined swelling in the left maxillary region, with a slightly painful bulge in the upper vestibular peri-gingival area. A computed tomography (CT) scan showed a well-encapsulated expansive hypodensity that filled the left maxillary sinus. Magnetic resonance imaging (MRI) revealed a mass hypo-intense on T1-weighted images, high intense on T2-weighted images, hyperintense on diffusion-weighted images, and had a low apparent diffusion coefficient with no contrast uptake observed after the injection of Gadolinium. Surgical excision under general anesthesia was considered. A combined approach using an endoscopic sinus and Caldwell-Luc approach was performed and the histopathological examination confirmed the diagnosis of an EC. In conclusion, the preoperative imaging, including CT scans and MRI, aids in diagnosing ECs and differentiating them from other sinus tumors. Postoperative follow-up involving endoscopic surveillance and CT scans is crucial to monitor for potential recurrence.
Introduction
Epidermoid cysts (ECs) in the paranasal sinuses are rare benign lesions. The frontal sinus is the most commonly affected, followed by the maxillary sinus and the ethmoid sinuses. 1 In the English literature, only a few dozen cases have been reported, with only 15 cases originating from the maxillary sinus. 1 The preoperative diagnosis of a paranasal EC is challenging and is frequently mistaken.1 -5 In this case report, we present the case of a 29-year-old female patient who presented with an EC originating in the maxillary sinus.
Case Report
A 29-year-old female patient visited our Ear, Nose, and Throat department due to the appearance of a swelling on the left side of her face a few months ago. The swelling has been gradually increasing in size and is not accompanied by any pain. There were no reported signs of neurological, ophthalmological, or rhinological issues. The patient had no history of sinus surgery, systemic illness, noninfectious diseases, or tobacco intoxication.
During the clinical examination, a tender, fixed, poorly defined, non-inflamed swelling measuring 3 cm was observed in the left maxillary region. The endoscopic nasal examination did not reveal any nasal masses or polyps. The intraoral examination identified a hard and slightly painful bulge measuring 2 cm in the upper vestibular peri-gingival area.
A computed tomography (CT) scan of the paranasal sinuses showed a well-encapsulated, non-enhanced, ex-pansive hypodensity that completely filled the left maxillary sinus. It was noted that the anterior wall of the maxillary sinus exhibited scalloping with erosion of the posterior and lateral walls, but there was no infiltration of the infratemporal fossa (Figure 1).
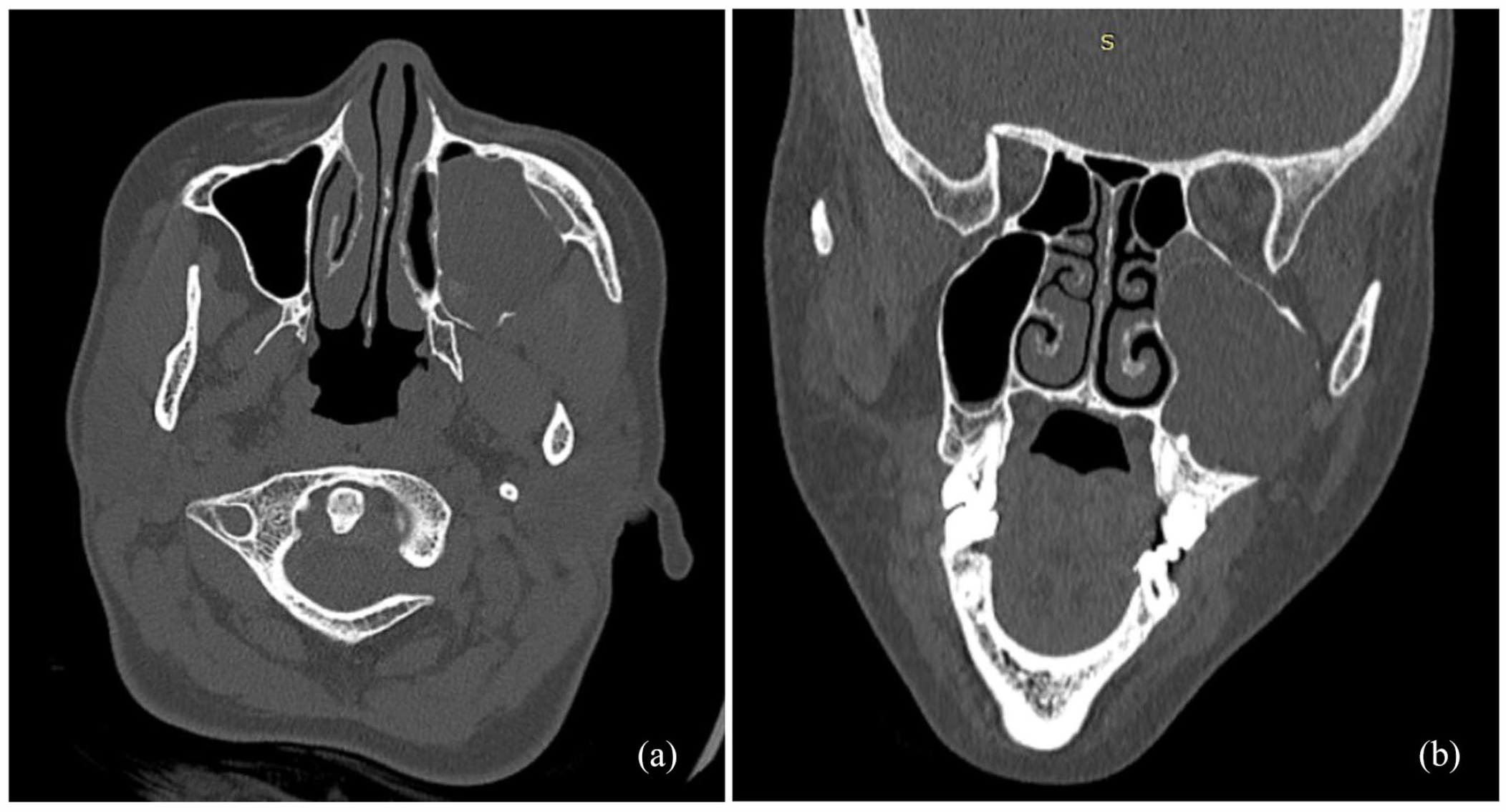
A computed tomography (CT) scan of the paranasal sinuses. (a) and (b) a well-encapsulated, expansive hypodensity completely filled the left maxillary sinus. The anterior wall of the maxillary sinus exhibited scalloping with erosion of the posterior and lateral walls.
Magnetic resonance imaging (MRI) of the paranasal sinuses revealed a cyst-like mass with distinct lobulated contours occupying the left maxillary sinus, causing scalloping on the anterior, lateral, and posterior walls. The mass measured 43 mm×34 mm in the axial plane and 48 mm in height. On imaging, the mass appeared hypo-intense on T1-weighted images, high intense on T2-weighted images, hyperintense on diffusion-weighted images (DWI), and had a low apparent diffusion coefficient (ADC; Figure 2). There was no contrast uptake observed after the injection of Gadolinium. A provisional diagnosis of an EC was considered, with mucocele and dermoid cyst of the maxillary sinus being proposed as differential diagnoses.
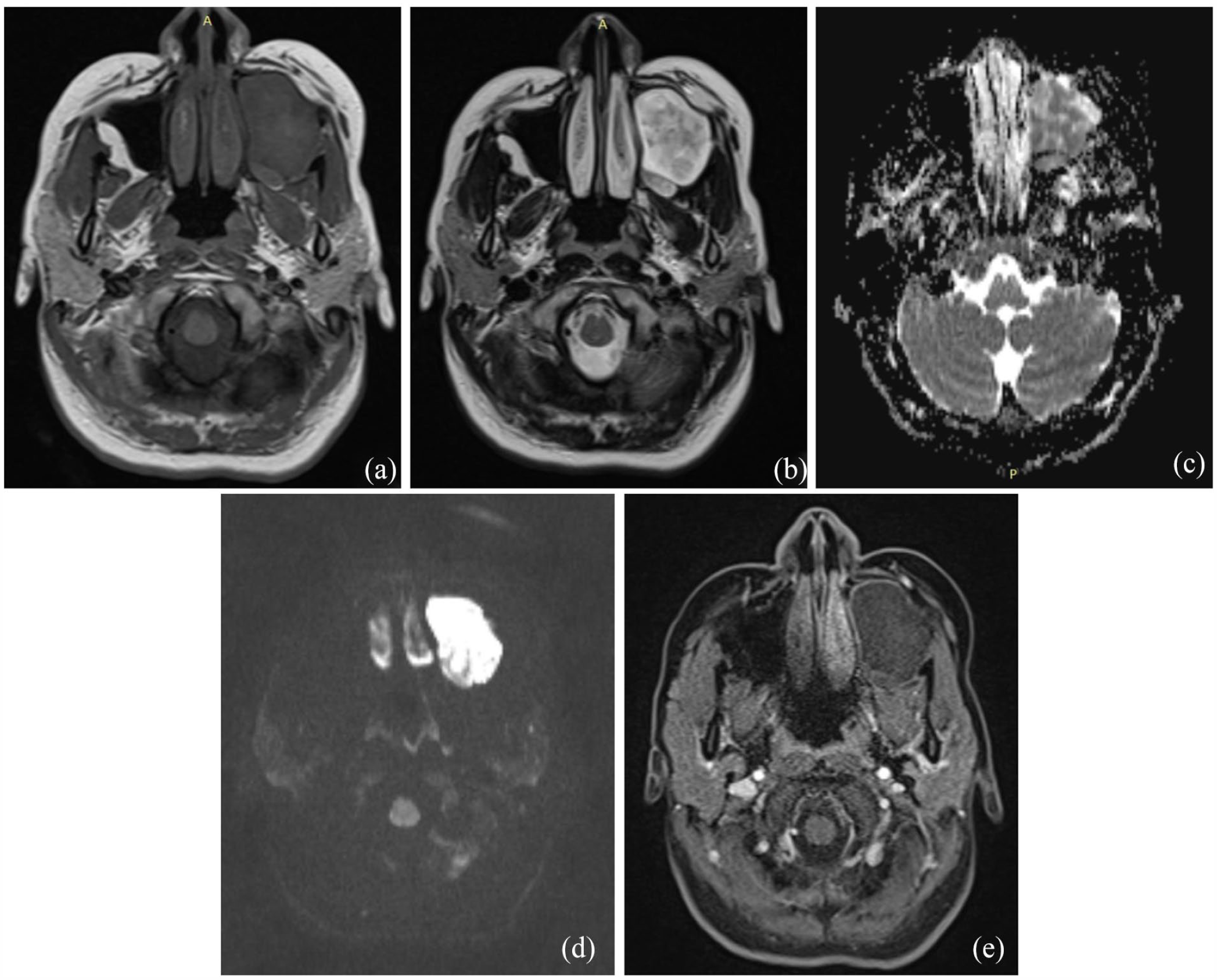
Magnetic resonance imaging (MRI) of the paranasal sinuses. (a) The mass appeared hypo-intense on T1-weighted images. (b) The mass appeared high intense on T2-weighted images. (c) The mass had a low apparent diffusion coefficient (ADC). (d) The mass appeared hyperintense on diffusion-weighted images. (e) The mass had no contrast uptake observed after the injection of Gadolinium.
Surgical excision under general anesthesia was recommended. A combined approach using an endoscopic sinus approach (large middle meatotomy) and Caldwell-Luc approach was performed due to the surgeons’ concerns about effectively controlling the inferior wall of the maxillary sinus endoscopically. During the operation, after marsupialization of the cyst, a cheesy content was found, confirming the diagnosis of an EC as the most likely. Consequently, the cyst’s dura was dissected from the surrounding bone tissue, and a radical excision was performed.
The histopathological examination revealed a cystic cavity lined by a regular squamous epithelium with a granular layer, resting on fibrosis that was continuous with a respiratory-type mucosa containing bone fragments (Figure 3). Some areas showed an inflammatory granuloma primarily composed of foreign body giant cells surrounding lamellae of keratin and cholesterol crystals. Based on these findings, the diagnosis of an EC was confirmed.
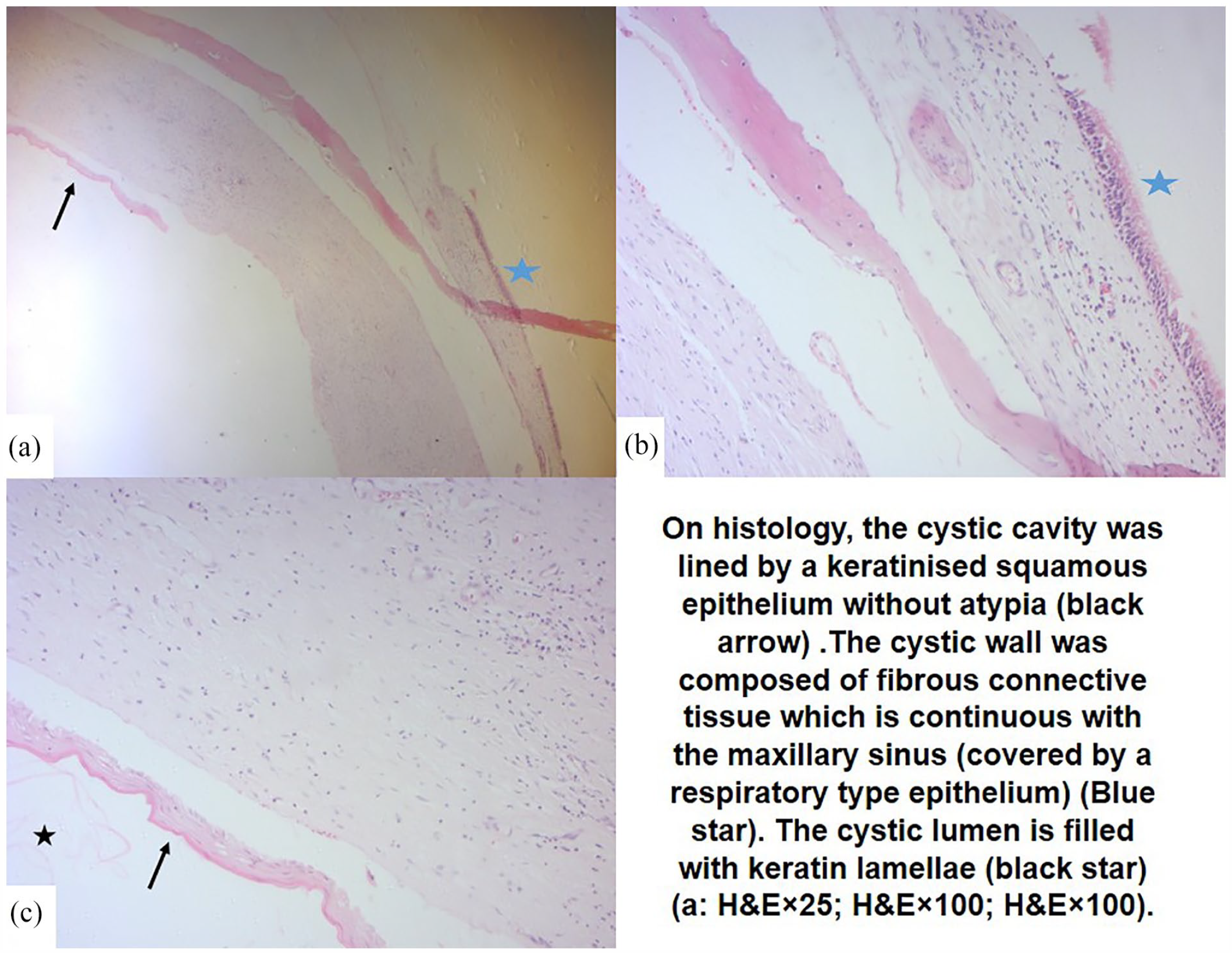
On histology, the cystic cavity was lined by a keratinized squamous epithelium without atypia (black arrow). The cystic wall was composed of fibrous connective tissue which is continuous with the maxillary sinus (covered by a respiratory-type epithelium) (blue star). The cystic lumen is filled with keratin lamellae (black star) ((a) HE × 25; (b) HE × 100; (c) HE × 100).
The postoperative healing process was uneventful, and the patient has been under follow-up for 12 months since the surgery without any clinical evidence of local recurrence.
Discussion
ECs in the maxillary sinus are benign lesions that can arise from abnormal epithelial components of ectodermal tissue during embryological development, or from implanted epithelium after trauma or surgery.1,5 Clinically, ECs are characterized by their smooth, expansive nature, which causes compression and destruction of surrounding tissues and bones. In the maxillary sinus, ECs may lead to nasal obstruction, recurrent sinusitis, infraorbital nerve dysfunction, disruption of normal sinus wall profiles, and facial deformities.1,5 However, these clinical signs are nonspecific for ECs and can also be observed in other benign and malignant sinus tumors.1,5
Preoperative imaging findings play a crucial role in diagnosing maxillary EC. CT scans typically show a well-encapsulated, unilocular, low-density mass in the maxillary sinus with erosion of surrounding bone but no soft tissue invasion. However, these signs are not pathognomonic1,6 and can also be observed in mucoceles, benign tumors (such as keratocystic odontogenic tumor, unicystic ameloblastoma), and malignant tumors (such as squamous cell carcinomas, salivary gland tumors).1,7 Despite the limitations in tissue characterization, CT scans are essential for determining bone invasion and selecting the most appropriate surgical approach.
MRI provides superior tissue characterization and can help exclude differential diagnoses. Uncomplicated ECs typically exhibit low or iso signal intensity on T1-weighted images and intermediate-high signal intensity on T2-weighted images.6,8,9 Additional study of DWI, ADC, and contrast enhancement with Gadolinium is crucial for tissue characterization. Maxillary sinus ECs, as similar to temporal bone ECs, often show high signal intensity on DWI, low ADC, and delayed peripheral contrast uptake after Gadolinium injection.6,8,9 These characteristic MRI findings play a key role in confirming the diagnosis of ECs, determining their soft tissue invasion, and excluding malignant and other benign tumors in the maxillary sinus. However, MRI has limited ability to assess bone changes.
The combination of preoperative CT scans and diffusion-weighted MRI of the paranasal sinuses is essential for diagnosing ECs in the paranasal sinuses and determining the most appropriate surgical approach.
Complete surgical removal is the gold standard treatment and should be considered for ECs.1,7,5 The cyst’s lining must be completely dissected to prevent recurrence. For ECs within the maxillary sinus, an endoscopic approach via medial meatotomy can successfully excise the cyst. However, this approach offers limited control over the inferior and anterior walls of the maxillary sinus. The combined transoral and transnasal endoscopic appr-oach, along with Caldwell-Luc procedure, is proposed as the treatment of choice to prevent recurrences, as demonstrated in our case. 10
No cases of recurrence in the maxillary sinus have been reported in the literature. However, strict postoperative follow-up is recommended to detect any potential recurrence. For this location, endoscopic surveillance combined with CT scans of the paranasal sinuses play a crucial role in follow-up, as they can help exclude re-currence.1,5
Footnotes
Author Contribution
All the authors have participated in the production of this article.
Data Availability Statement
The data are available with the corresponding author
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The patient gave their approval for reporting the case.
Informed Consent
The patient gave her approval for reporting the case.
Patient Perspective
The patient is satisfied with the treatment received.