
Abstract
Gouty tophi is a disease characterized by the long-term deposition of monosodium urate crystals in joints or cartilages. The most commonly affected site is the first metatarsophalangeal joint, and gouty tophi in the head and neck region are relatively rare. This article reports a case involving an elderly male with asymptomatic gouty tophi in the thyroid cartilage. The patient had a history of gout for over 10 years and presented with a painless thyroid mass that had been present for at least 3 years. He had not received systemic treatment. Preoperative contrast-enhanced cervical CT results indicated a high likelihood of gouty tophi. Postoperative pathology confirmed the mass to be consistent with gouty nodules. Following the procedure, the patient was treated symptomatically with non-busulfan tablets and colchicine. No recurrence was observed at the 1-year follow-up. This report highlights the need to consider gouty tophi in cases of prolonged gout history and abnormal imaging findings in the head and neck region. Appropriate management, including urate-lowering therapy and surgery, if necessary, can lead to optimal outcomes and prevent recurrences. Further research is warranted to enhance understanding and clinical management of this uncommon regional manifestation of gout.
Introduction
Gout is a disorder caused by disturbances in purine metabolism or reduced excretion of uric acid, which leads to the formation of gouty tophi when serum monosodium urate (MSU) levels exceed the saturation point (>7.0 mg/dL). Gouty tophi manifests as chronic gout, typically occurring more than 10 years after the initial gout diagnosis. During the chronic stable phase, patients usually do not exhibit clinical manifestations such as redness, swelling, or pain, and gouty tophi is more common in males than in females. During the acute phase of gouty tophi the typical symptoms include redness, swelling, heat, and pain. However, when the disease enters the chronic phase, it may not exhibit clinical symptoms. Owing to the rarity of gouty tophi in the head and neck region, there is a tendency for misdiagnosis or missed diagnosis in clinical practice. When the swelling is mild, uric acid-lowering medications can be administered. However, if the swelling is significant and causes severe complications, surgical removal of the affected tissue is necessary. Herein, we report a rare case of painless thyroid cartilage gout tophus. There were no apparent clinical symptoms before surgery; however, the swelling was significant. To prevent further enlargement of the swelling and its intrusion into the airway, which may affect breathing, surgical treatment was performed along with uric acid-lowering therapy, which resulted in good outcomes. No recurrence was observed during the 1-year postoperative follow-up period.
Case Report
The patient, a 52-year-old male, presented at the Department of Otolaryngology—Head and Neck Surgery, Guangdong Medical University Affiliated Hospital, with the chief complaint of “painless neck mass for more than 3 years.” Three years prior, the patient had an incidentally discovered central anterior neck mass without significant tenderness, hoarseness, dysphagia, or breathing difficulties. Over time, the patient noticed a gradual increase in the mass size. Therefore, the patient sought medical attention at another hospital, where a neck CT scan revealed a “thyroid cartilage lesion.” No further treatments were administered. The patient underwent further medical evaluation and management at our institution. Past medical history revealed gout for over 10 years, with irregular use of colchicine and sustained-release lofentanil, but poor control of the gout condition.In recent years, multiple nodules had appeared progressively and enlarged throughout the body. The patient underwent excision of the nodules on both heels, both knee joints, and left wrist joint, both externally and in our hospital. The pathological examination of the excised nodules confirmed the presence of gouty tophi. Upon admission, physical examination revealed a palpable mass approximately 4.0 cm × 2.0 cm × 2.0 cm in size, located at the anterior midline of the neck, with hard texture, no tenderness, normal local skin temperature, smooth surface, and close adhesion to the thyroid cartilage. The mass moved slightly upward and downward during swallowing. Contrast-enhanced neck CT performed after admission (Figure 1) revealed scattered, nodular, and high-density shadows in the anterior neck region. The margins were relatively clear, and the internal density was slightly uneven, with CT values of approximately 150 to 196 HU. No obvious signs of enhancement were observed after the contrast scan. However, adjacent bone sclerosis and cystic changes were observed. Gout was considered the most likely diagnosis. A preliminary diagnosis of gouty tophi in the thyroid cartilage was established. Laboratory test results before surgery showed a white blood cell count of 5.89 × 109/L, uric acid level of 594.9 umol/L, creatinine level of 120 umol/L, and fasting blood glucose level of 4.35 mmol/L. After excluding absolute surgical contraindications, the patient underwent a thyroid cartilage mass excision under general anesthesia. A transverse incision, approximately 8 cm in length, was made along the skin creases adjacent to the neck mass. The skin and subcutaneous tissues were dissected and the mass was isolated. The mass was closely adhered to the surface of the thyroid cartilage, appearing as a circular structure with an intact surface and partially protruding into the deep side of the hyoid bone. The strap muscles in front of the neck were separated along the surface of the mass, exposing the boundaries on both sides. The mass could be separated from the surface of the thyroid cartilage. By pulling the hyoid bone and pushing the mass downward, the boundary of the mass remained visible and it gradually separated. The separation extended to the surface of the thyroid cartilage and the local mass was tightly attached to the thyroid cartilage plate. The mass and a portion of the cartilaginous tissue were completely excised (Figure 2A and B), and upon cutting the mass, a grayish-white paste-like substance was observed (Figure 2C). Negative pressure drainage was placed in the surgical cavity after the operation and removed 2 days later. Routine treatments such as fluid supplementation, nebulization, hemostasis, and antiemetics were administered postoperatively. The incision healed. A routine pathological report after surgery (Figure 3) showed that, under the microscope, the lesion had a blurry border with a large number of nodules of various sizes arranged centrally in a radiating pattern of needle-like crystals. Fibroblasts, lymphocytes, and multinucleated giant cells were observed around the nodules, and the diagnosis of gouty tophi was confirmed based on the clinical history and laboratory examination. After discharge, the patient received regular oral treatment with non-busulfan tablets and colchicine. A follow-up examination after 1 year showed no signs of recurrence.
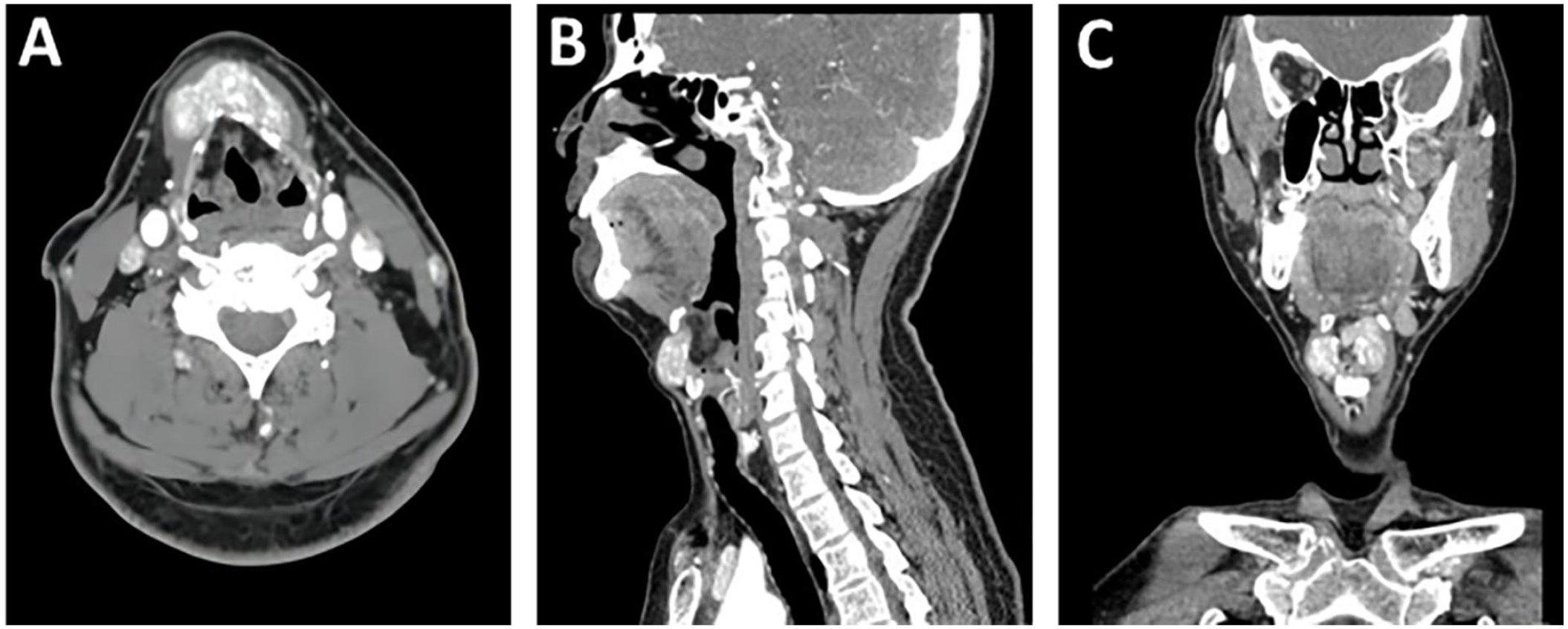
Imaging examination reveals irregular high-density shadows closely adhering to the periphery of the thyroid cartilage. (A) Horizontal view. (B) Sagittal view. (C) Coronal view.
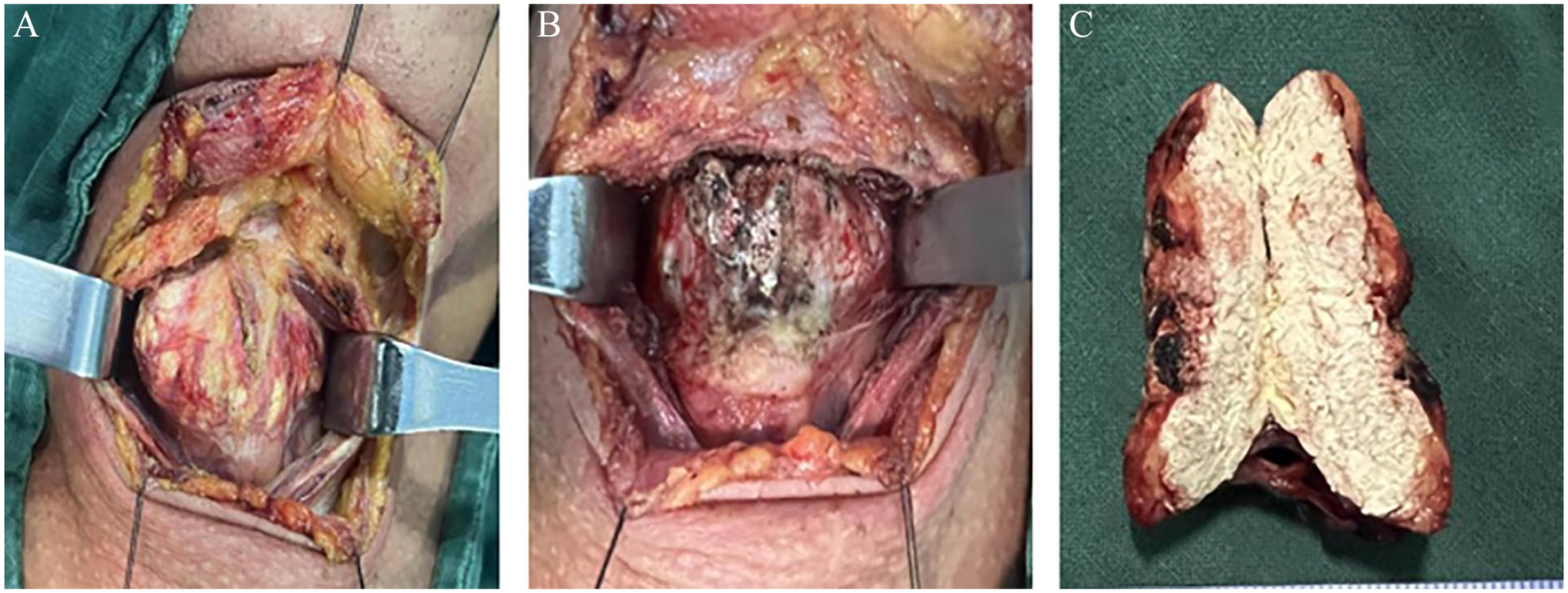
Intraoperative images. (A) Intraoperative observation, showing the mass closely adhering to the thyroid cartilage plate and complete excision of the mass along with a portion of the cartilage. (B) The mass and a portion of the cartilage are completely excised. (C) Observation after the mass is incised, revealing a grayish-white paste-like substance.
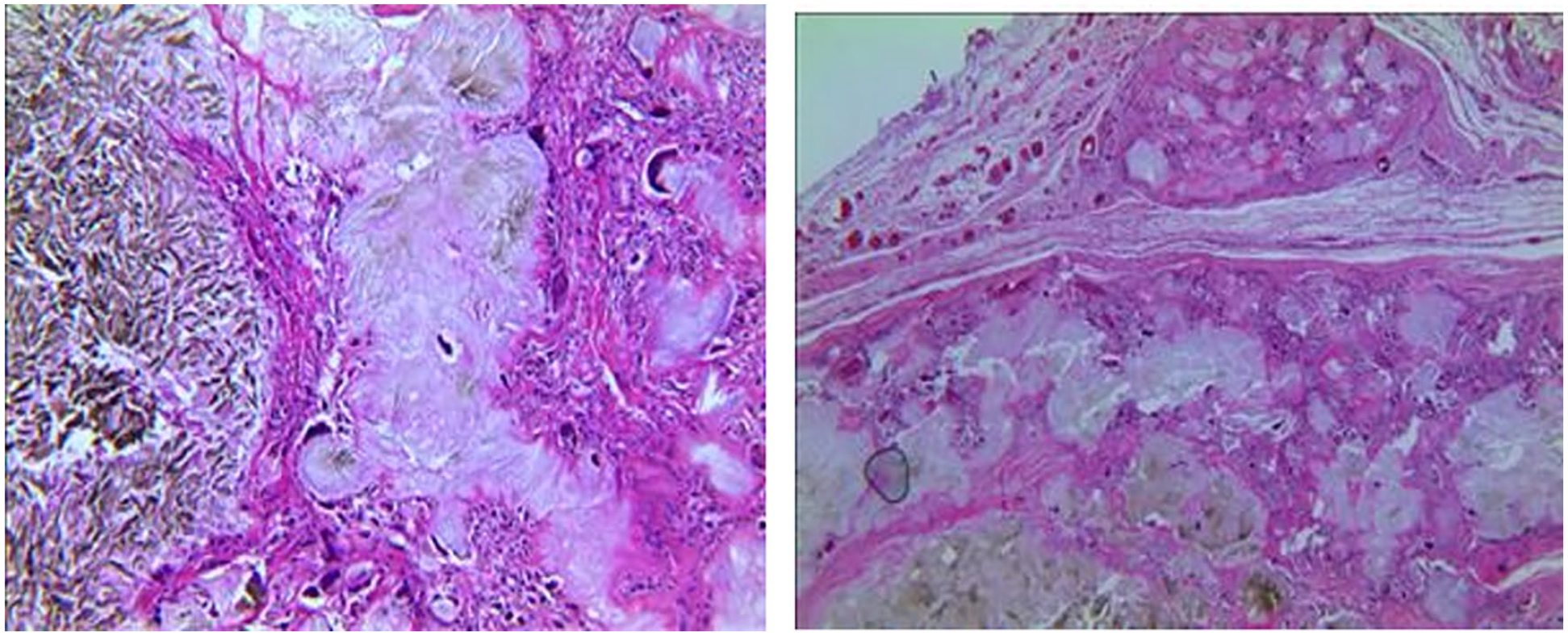
Postoperative pathological image. Microscopic examination displays a significant number of nodules in varying sizes in the central area. The nodules exhibit a radiating arrangement of needle-like crystals in their centers, surrounded by fibroblasts, lymphocytes, and multinucleated giant cells, which are characteristic features consistent with gouty tophi.
Discussion
Gouty tophi is a pathological condition in which urate crystals precipitate from elevated blood uric acid levels and are deposited in various tissues within or outside the joints. These tophi can be categorized as typical and atypical sites. 1 The most common location is the first metatarsophalangeal joint, followed by the wrist, ankle, and knee joints. 2 Gouty tophi occurring in the head and neck region are considered atypical and have been reported in the nose, 3 middle ear, 4 and vocal cords. 5 Among these, gouty tophi in the thyroid cartilage are relatively rare, with a limited number of documented cases, both domestically and internationally. A review of relevant literature revealed only 6 reported cases.
The thyroid cartilage is the largest cartilage in the larynx, located between the hyoid bone and the cricoid cartilage, and it covers the tracheal rings. When gouty tophi occur in the thyroid cartilage, they typically appear as irregular masses with higher density than soft tissue but lower density than calcifications on CT scans 6 Studies of laryngeal and thyroid cartilage gouty tophi have mostly been presented as case reports. The manifestations of gouty tophi in the larynx and thyroid cartilage are usually atypical and can cause symptoms such as hoarseness and throat pain. In severe cases, involvement of the trachea may lead to breathing difficulties or respiratory failure. In 1863, Garrod 7 first described the deposition of urate crystals in the cricoid cartilage. Tsikoudas et al. 8 suggested that during the acute phase of gouty tophi in the thyroid cartilage, patients may experience throat pain, ear pain, difficulty in swallowing, hoarseness, and breathing difficulties. Lee et al. 9 reported 1 case of gouty tophi on the thyroid cartilage plate and the longus colli muscle, causing severe throat pain and intermittent swallowing difficulties. Arlandis et al. 10 reported a case of laryngeal gouty tophi that resulted in respiratory failure. Therefore, once gouty tophi are detected in the larynx or thyroid cartilage, prompt surgical excision is recommended to prevent continuous enlargement of the mass and the occurrence of severe complications.
In the clinical differentiation of gouty tophi occurring in this area, the following diseases should be considered:
(1) Thyroglossal duct cyst (TGDC): A TGDC is a congenital cyst formed by the incomplete regression of the thyroglossal duct during early embryonic development, leaving a cyst in the neck. Cysts can occur at any location along the midline of the neck, from the tongue foramen to the sternal notch. Ultrasound is a common imaging examination for TGDC, showing a cystic mass between the base of the tongue and the suprasternal notch, closely related to the hyoid bone. The typical ultrasound presentation of a TGDC is a well-circumscribed, round, or oval anechoic lesion with no internal flow with Doppler imaging; however, if infection or hemorrhage occurs, TGDC will present as a typical hypoechoic lesion. 11
(2) Laryngeal chondroma: Laryngeal chondroma is a benign cartilaginous tumor, most commonly involving the cricoid cartilage, followed by the thyroid cartilage. CT is the most used imaging method for laryngeal chondroma, 12 which presents as a low-density, well-defined mass with scattered punctate or patchy coarse linear cartilaginous calcifications within the lesion. Histologically, the lesion is composed of mature hyaline cartilage cells and cartilaginous matrix without pathological mitotic figures. 13
Although imaging examinations can provide a basis for clinical diagnosis and differentiation, the gold standard for diagnosing gouty tophi remains pathological examination. The pathological features of gouty tophi include urate crystal deposits at the center surrounded by a significant number of macrophages and plasma cells. In our patient, numerous nodules of varying sizes were observed, showing a radiating arrangement of needle-like crystals at the center surrounded by fibroblasts, lymphocytes, and multinucleated giant cells, consistent with the pathological characteristics of gouty tophi. Currently, there is significant research interest in neutrophil extracellular traps and their crucial role in the formation of gouty tophi, which are involved along with MSU crystals in the formation.14,15
In this study, the patient was admitted to the hospital with a painless neck mass that had persisted for over 3 years. On physical examination, a hard mass was palpable at the midline of the anterior neck without tenderness. Our hospital’s enhanced CT scan revealed scattered, nodular, high-density shadows in the anterior neck with relatively clear margins. Considering the patient’s history of gout for more than 10 years, irregular oral administration of urate-lowering drugs, and poorly controlled uric acid levels, excess uric acid resulted in the deposition of urate crystals in the thyroid cartilage, leading to the formation of gouty tophi. At the time of this report, the tophi were in a chronic stable phase without acute symptoms such as redness, swelling, or pain. Further evaluation based on preoperative enhanced CT results confirmed the diagnosis of gouty tophi. Therefore, to prevent the enlargement of the mass and its intrusion into the airway, which would affect respiration, the treatment team decided to perform surgical excision of the tophi. However, to optimize the surgical outcome, the patient needed to take urate-lowering medication before the operation to normalize uric acid levels. To prevent recurrence postoperatively, the patient was advised to continue oral febuxostat and colchicine administration for uric acid-lowering treatment.
Conclusion
In conclusion, cases of gouty tophi occurring in the head and neck region, especially in the thyroid cartilage, are relatively rare, and clinical awareness among medical professionals is often lacking, which may lead to oversight or misdiagnosis. Therefore, in clinical practice, the possibility of gouty tophi should be considered when encountering patients with a long history of gout, a lack of systematic urate-lowering treatment, elevated blood uric acid levels, and imaging findings suggestive of a mass, regardless of whether the patient exhibits clinical symptoms. Additionally, active differentiation from related diseases should be pursued to avoid misdiagnosis and missed diagnoses, thereby enabling better diagnostic and treatment plans for patients. The recurrence of gouty tophi can be effectively reduced by controlling diet and implementing systematic urate-lowering treatment.
Footnotes
Author Contributions
Li and Chen: Writing and editing of the article and Dai and Zhou: Image analysis and article contributions. All the authors have read and agreed to the published version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent for Publication
Informed consent was obtained from the patient for the publication of this case report and the accompanying images.