
Abstract
Introduction
Head and neck cancer is a globally increasing problem due to factors such as tobacco use and human papillomavirus infection. It is one of the most prevalent cancers worldwide, particularly in South Asia, Brazil, and Central Europe.1,2 Although the introduction of multimodal treatments has improved locoregional control and overall survival rates for advanced head and neck cancer patients, 3 coordination with patients remains a challenge, leading to potentially unsatisfactory outcomes. 4
Interruptions in radiotherapy are known to reduce survival,5,6 and a delay of 60 days in treatment initiation is associated with lower overall survival and higher recurrence rates. 7 Treatment outcomes are influenced by the timing of treatment initiation, postoperative radiotherapy, and treatment package time.8-10 Prompt countermeasures can be implemented once treatment has commenced, as patients are already under surveillance. However, identifying factors that cause patients to hesitate in starting treatment poses a greater challenge. There is limited research on these initial noncompliance factors. This study aims to retrospectively analyze the factors that contribute to noncompliance in initiating treatment for newly diagnosed head and neck cancers.
Patients and Methods
Study Population
Data from head and neck cancer patients (oral cavity, oropharynx, laryngopharynx, and nasopharynx) at Wan Fang Hospital between January 2018 and September 2020 were retrospectively analyzed. A total of 271 patients’ data were retrieved from the database. After excluding patients with multiple cancers, inconclusive diagnoses, rare primary cancer sites (nasal cavity, paranasal sinuses, and salivary glands), and unknown primary site, 193 patients remained. Their age ranged from 27 to 93 years, with an average age of 58.3 years, and the male/female ratio was 4.87:1. The patients were divided into 2 groups: delayed (76 patients) and on-time (117 cases) based on receiving standard treatment within a month of diagnosis.
Study Design
Patients in this study were divided into 2 groups. The on-time group included patients who received treatment according to their doctor’s schedule after diagnosis and staging at Wan Fang Hospital. The delayed group comprised patients who did not follow the treatment plan or recommendations either at Wan Fang Hospital or another hospital without referral for further consultation.
Factors influencing compliance were categorized as age, gender, primary cancer site (oral cavity, nasopharynx, oropharynx, and hypopharynx-larynx), T stage, N stage, M stage, overall stage (I–IV), patient’s residency inside or outside the territorial dominion of Wan Fang Hospital (Figure 1; Wenshan district of Taipei City, Shenkeng district, Pinglin district, and Shiding district of New Taipei City), and whether the patient visited before or after March 1, 2020, when the Taiwanese government imposed intensive border and social activity restrictions due to COVID-19.
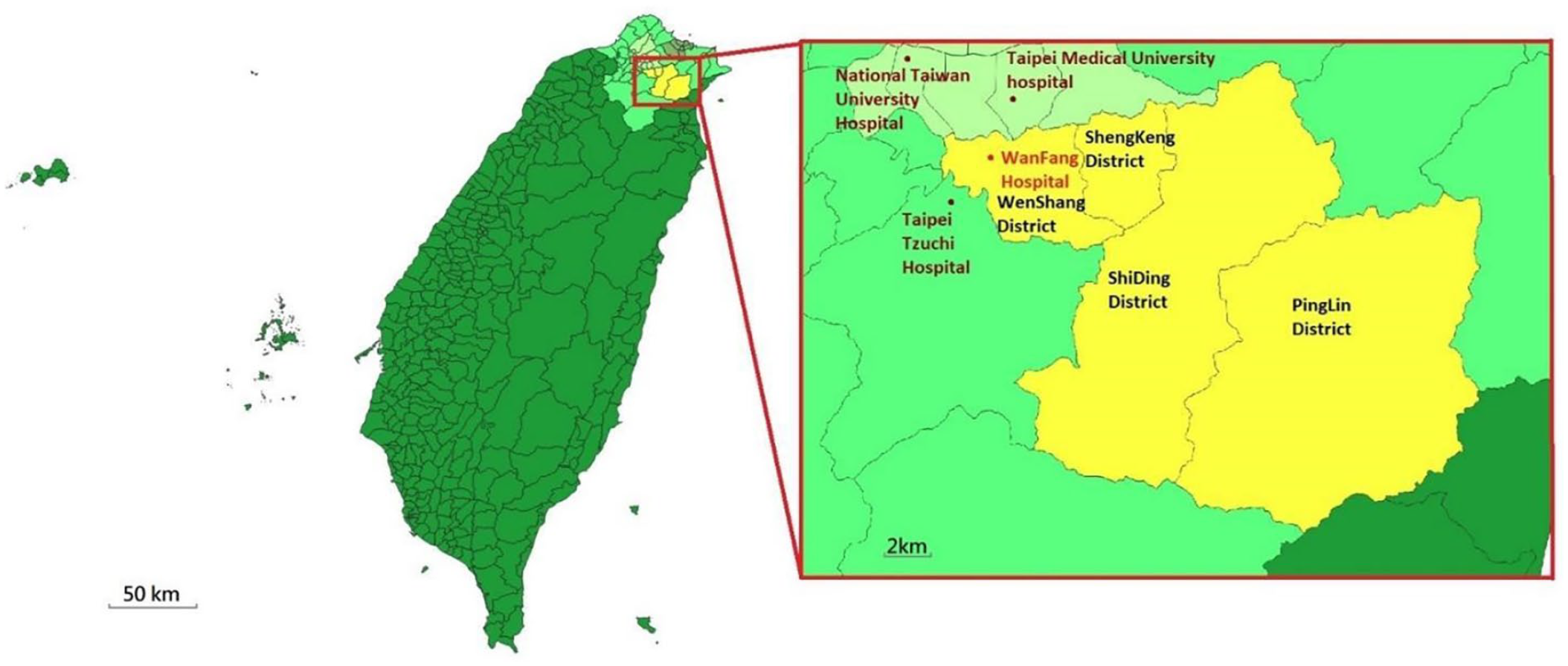
The territorial dominion of Wan Fang Hospital. Taiwan and outlying islands (dark green), New Taipei City (fluorescent green), Taipei City (light green), Keelung City (gray-green), and the region of Wan Fang Hospital (yellow). The location of Wan Fang Hospital and the other nearby hospitals (Taipei Tzuchi Hospital, Taipei Medical University Hospital, and National Taiwan University Hospital) are marked as red and brown dots, respectively. This figure was made with QGIS version 3.16 (Open Source Geospatial Foundation, Chicago, USA) using map resources from the open data platform of the Taiwanese government.
Multidisciplinary Team Care
The patient’s treatment recommendations and planning were performed by a specialized head and neck tumor board team comprising otolaryngologists, surgeons, oncologists, radiologists, pathologists, rehabilitation physicians, nutritionists, social workers, and case managers.
Ethical Approval
All procedures performed in studies involving human participants followed the ethical standards approved by the TMU-JIRB (Approval Number: N202101050).
Statistical Methods
Data were analyzed using SPSS version 16.0 (IBM, Armonk, NY, USA). Group comparisons of quantitative parameters used the t-test, and categorical parameters were analyzed using χ2 test to examine differences in patient compliance and factors such as age, gender, primary cancer site, T stage, N stage, M stage, overall stage, residency, and the impact of COVID-19. Binary logistic regression analysis was conducted to explore associations between patient compliance and potential factors. Independent variables with a P-value < .1 (chi-square test/t-test) were included in the logistic regression model. A backward stepwise approach in our regression model was applied with significance defined as P < 0.09.
Results
Patient Demographics and Descriptive Statistics
From January 2018 to September 2020, 193 eligible patients were included. The on-time group had 117 patients, while the delayed group had 76 patients. The average age was 58.3 ± 12.1 years, ranging from 27 to 93 years, and the male/female ratio was 4.87:1.
Factors Affecting the Compliance With Curative-Intent Treatment
Table 1 displays the factors potentially influencing initial compliance with standard cancer treatment recommendations. Gender did not significantly impact patient compliance. Patients ≥55 year old had higher treatment delay rates (P = .097). Compliance decreased with advancing T stage (19.7% delay and 17.9% on-time in T4 patient, respectfully, P = .074), N stage (10.5% delay and 13.7% on-time in N3 patient, respectfully, P = .023), and over all stage, with 56.9% of stage IV patients experiencing delays (P = .001). Patients with nasopharyngeal carcinoma (NPC) have better compliance (30.3% delay and 15.4% on-time, respectfully, P = .013). Patients living far from the hospital had higher noncompliance rates compared to those in the Wan Fang territorial dominion (56.6% vs 34.7%, P = .003). Compliance improved after the COVID-19 pandemic (13.2 vs 28.2%, P = .019).
Comparison of Factors on Compliance and Noncompliance Group.
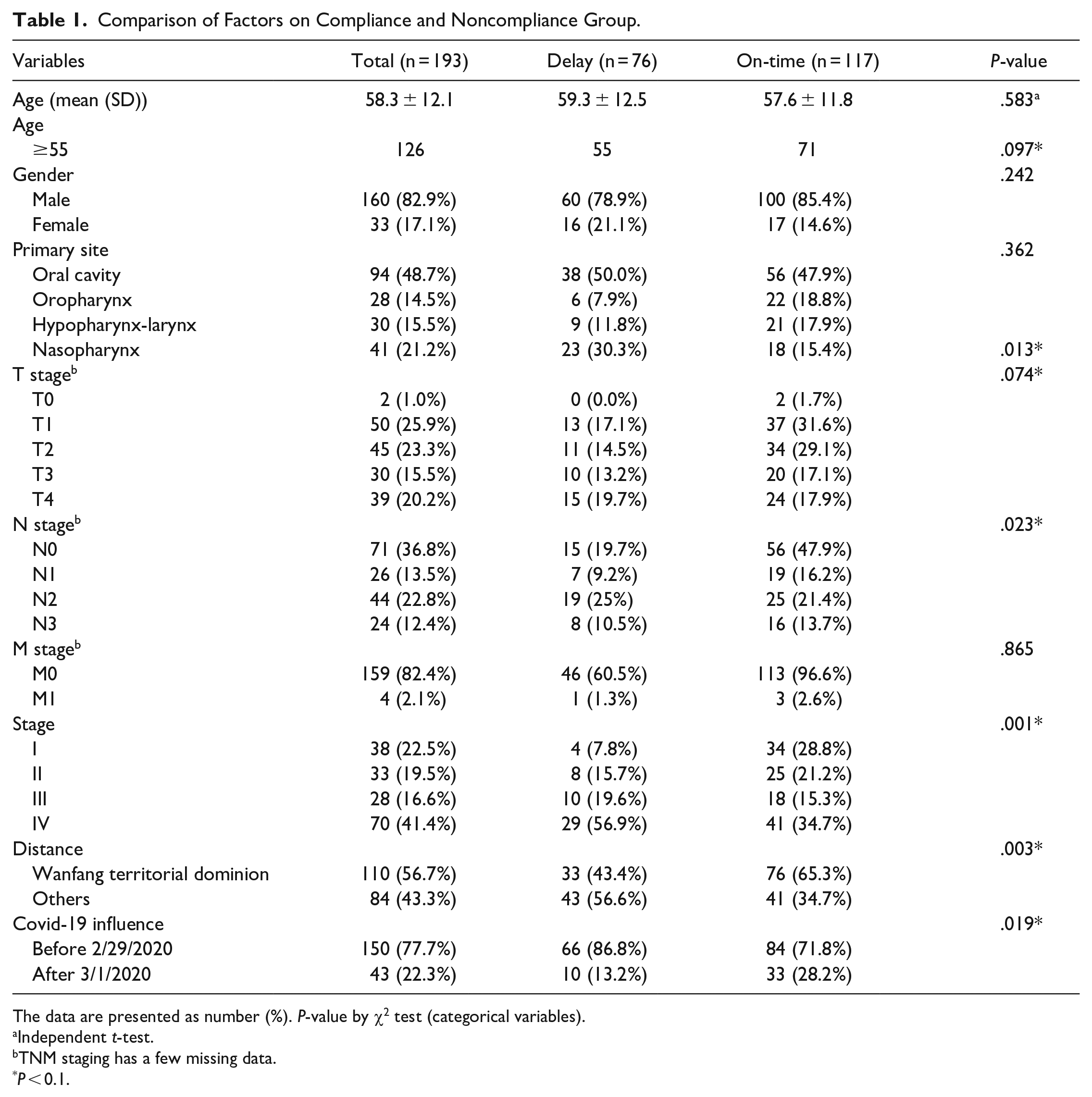
The data are presented as number (%). P-value by χ2 test (categorical variables).
Independent t-test.
TNM staging has a few missing data.
P < 0.1.
Table 2 presents the multivariate analysis of factors affecting patient compliance. Stage IV cancer patients had higher treatment delay rates than stage I (P = 0.048; 95% CI: 1.178, 2.229). Patients living far from the hospital were more likely to delay treatment than those in the Wan Fang territorial dominion (P = 0.022; 95% CI: 1.129, 4.757). A trend of increased initial treatment compliance in NPC patient (P = 0.224; 95% CI: 0.689, 4.913) and after the COVID-19 pandemic was observed (P = 0.184; 95% CI: 0.213, 1.346).
Determinants for Patient’s Noncompliance.
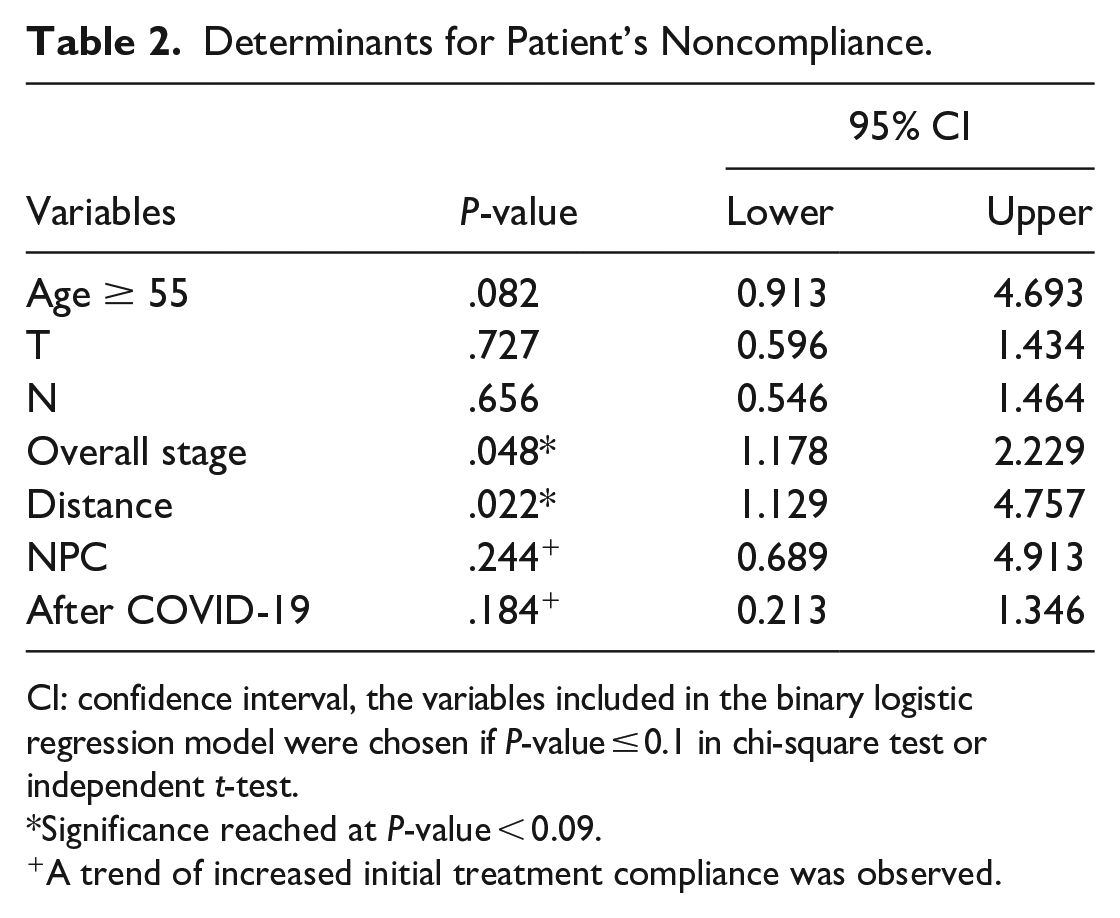
CI: confidence interval, the variables included in the binary logistic regression model were chosen if P-value ≤ 0.1 in chi-square test or independent t-test.
Significance reached at P-value < 0.09.
A trend of increased initial treatment compliance was observed.
Discussion
In this study, factors (over all stage, distance to hospital, patient with NPC, and COVID-19) affecting treatment compliance in newly diagnosed head and neck cancer patients were identified. These findings provide valuable insights into treatment initiation and intention, an area often overlooked in existing literature on head and neck cancer therapy compliance.
Treatment compliance is vital in achieving favorable outcomes across various diseases. 11 Numerous studies have highlighted its importance in head and neck cancer treatment. Patel et al investigated the impact of poor compliance on persistent neck disease in 40 patients with advanced squamous cell carcinoma. They found that noncompliance was significantly associated with positive pathology results. 12
Despite patients’ reluctance to engage in treatment or follow standard recommendations, timely care is crucial for the survival of head and neck cancer patients. However, unanswered questions persist, such as identifying barriers to timely care. In this study, we aim to investigate these issues and develop strategies to overcome them. 9 Liao et al reported that patients with a delay in time to treatment initiation exceeding 60 days had poorer survival and a greater risk of recurrence. 7 Chang et al studied 1095 HNC patients to identify factors impacting treatment plan discordance. They found that advanced cancer stages, advanced age, and treatment plans involving best supportive care or surgery combined with radiation, chemotherapy, or chemoradiation were associated with higher rates of discordance. 13
Duvvi et al proposed a 2-week rule for suspected head and neck cancer in the UK NHS system in 2006. Compliance with this guideline was linked to higher cancer detection rates and improved outcomes. 14 In India, early treatment decisions and referrals have been shown to reduce patient dropout rates and improve compliance. 15 The authors suggested decentralizing cancer care to handle the large number of patients at tertiary care centers. These studies highlight healthcare availability issues. In Taiwan, where over 98% of the population is covered by national health insurance, our study’s findings are particularly interesting.16,17 Factors influencing patients’ initial treatment intentions may be noteworthy, as they might not be easily resolved with socioeconomic growth and increased health investments.18,19
In our study, patients with stage IV diseases showed a higher likelihood of noncompliance with treatment recommendations. This finding may be related to the significant impact of advanced stage cancer treatment, which often results in noticeable changes in appearance, speech, smell, and swallowing functions.20,21
The impact of distance on initial treatment intentions is significant in this study, especially in the context of Taiwan. Despite a high density of healthcare providers, even areas outside the territorial dominion of Wan Fang Hospital are often within a 1-hour driving distance. Previous studies on colorectal cancer patients have shown that uncontrolled pain and lack of social support are associated with transportation barriers. Thus, it is crucial to routinely inquire about accessible transportation as part of cancer care. 22 More recently, a study revealed that transportation barriers significantly influence cancer patients’ treatment decisions, including discontinuation of treatment. 23 This study also showed that limited access to private vehicles can specifically impact radiotherapy. Therefore, we suggest assessing patients’ residence areas and transportation methods, including those of their caregivers, during initial interactions. If transportation barriers are identified, exploring possible aids or subsidies should be considered.
Limited by case numbers, a trend of increased initial treatment compliance was observed after the COVID-19 pandemic. Changes in patient behavior and the impact on healthcare systems require further exploration. As head and neck cancer treatment shifts to virtual settings, healthcare providers should be aware of patients seeking treatment at the nearest accessible facility. The hardware, software, and resources for the multidisciplinary team should be reassessed and reinforced to manage the anticipated increase in patient volume post-pandemic.
Our study has limitations. The retrospective design introduces selection bias, potentially impacting the actual disease incidence rate. Address information documented may differ from actual residence, and caregiver addresses were not investigated. Therefore, the transportation barrier identified should be considered a rough estimation.
Conclusion
The overall stage, patient proximity to the Wan Fang territorial dominion, patient with NPC, and the impact of COVID-19 may influence compliance with curative-intent treatment for newly diagnosed head and neck cancers. Although the impact on outcomes is uncertain, physicians and healthcare providers can enhance patient information, promote shared decision-making, and address transportation barriers to improve treatment compliance in these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from TMU Wan Fang Hospital research grant (no. 112-wf-eva-25) and National Science and Technology Council grant (no. 111-2222-E-038 -003 -MY2).