
Abstract
Keywords
Introduction
A pharyngoesophageal diverticulum is a rare clinical condition that can be further classified as Zenker’s diverticulum (ZD), Killian-Jamieson’s diverticulum (KJD), or Laimer’s diverticulum (LD), depending on the site of origin. 1 The most frequent type is ZD, which originates dorsally between the thyropharyngeus and cricopharyngeus muscles (CPM). 2 KJD is an anterolateral diverticulum that originates in an area of anatomic weakness known as the Killian-Jamieson triangle, which is located inferior to CPM, superior to circular muscle, and lateral to the longitudinal muscle of the cervical esophagus; the recurrent laryngeal nerve (RLN) enters this location as it courses into the larynx. 3 LD, arising dorsally from the Laimer-Hackerman’s triangle, which is located beneath CPM, is much rarer. 4 So far, only 4 cases of LD have been reported separately in the literature, all of which underwent open surgical procedures;1,2,4 however, the authors did not explain their choice of open surgery over endoscopic procedures. Here, we report our experience of open surgical management of 3 cases of LD.
Patients and Methods
A retrospective review of LD cases treated at our tertiary medical institution was conducted between July 2018 and May 2023. The clinical and demographic data were retrieved from case notes. The Institutional Review Board approved the protocol of the research project, which conformed to the provisions of the Declaration of Helsinki. A written consent form was obtained from the patients.
Diagnosis
The cervical esophageal diverticula in the first 2 cases were both accidentally discovered, 1 by gastric endoscope and the other by cervical MRI, performed for non-specific symptoms (Table 1), while the third case presented as a cervical mass (Figure 1A). After initial discovery, barium or Urografin swallow studies revealed that the diverticula were dorsally located in the cervical esophagus (Figure 1B). At this point, KJD could be ruled out because they should be anterolateral to the cervical esophagus, but ZD and LD were both possible.
Patient Characteristics of This Series and Literature.
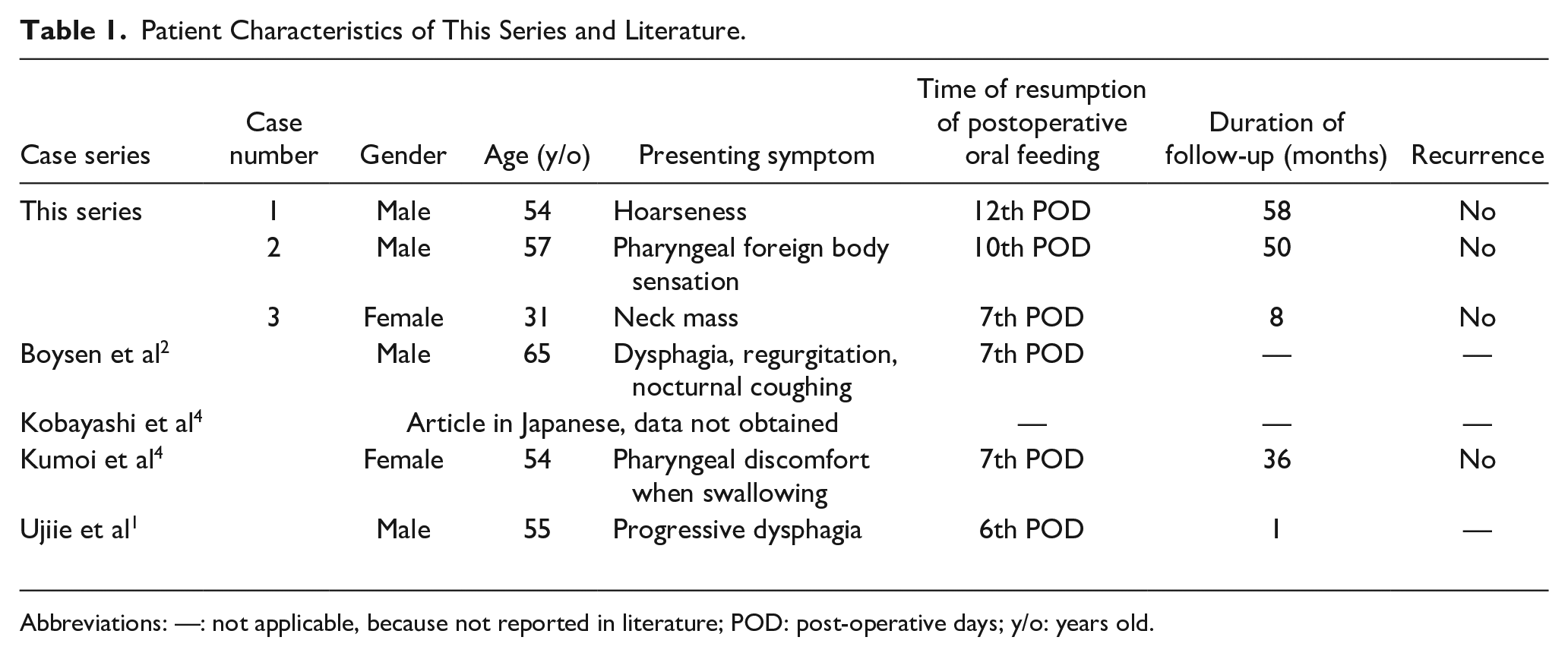
Abbreviations: —: not applicable, because not reported in literature; POD: post-operative days; y/o: years old.
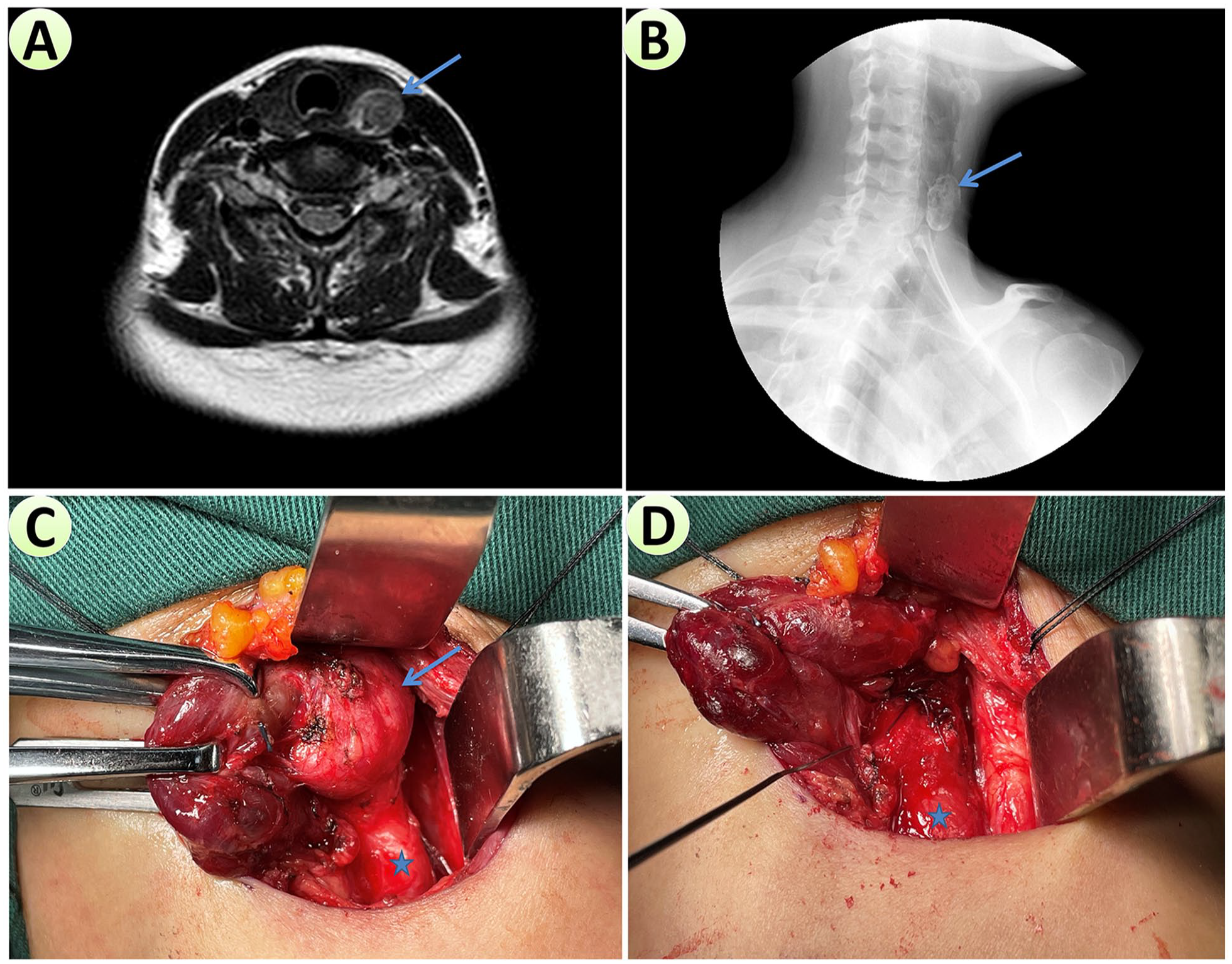
Preoperative evaluations and intraoperative photographs of Case 3. A. Preoperative axial T2WI MRI image showing a left-sided cervical lesion (blue arrow) with potential communication into the cervical esophagus. B. Lateral view of preoperative Urografin swallow study showing a diverticulum (blue arrow) located on the dorsal side of the cervical esophagus. C. Intraoperative photograph showing esophageal diverticulum (blue arrow) after mobilization of the left thyroid lobe (retracted medially by Allis clamps). The cervical esophagus (blue star) was directly continuous with the inferior border of the diverticulum without the CPM separating them, and the diverticulum was dorsally located and away from RLN; hence, this was a Laimer’s diverticulum. D. After identifying the whole course of RLN (at the tip of the monitoring probe), diverticulectomy was performed immediately below CPM (without myotomy of CPM), and manual suturing of the esophagus (blue star) was performed.
All 3 patients agreed to receive an open surgical procedure, after thorough consultation about open surgery, rigid endoscope, and flexible endoscope.
Surgical procedure
After general anesthesia, a nasogastric feeding tube (NG-FT) was inserted. A transverse skin incision was made along the skin crease immediately above the clavicle on the left side for cosmetic considerations, especially for Case 3 (a young female patient), rather than the horizontal incision performed just inferolateral to the cricoid cartilage, which was reported in the literature. 5 Subplatysmal flaps were elevated to expose the anterior border of the sternocleidomastoid muscle (SCM). Then, the SCM was mobilized and retracted laterally to expose the carotid sheath, which was then mobilized and also retracted laterally. The left thyroid lobe could be visualized, mobilized, and retracted medially (Figure 1C) with RLN monitoring. A diverticulum could be identified on the posterior cervical esophagus away from RLN (Figure 1D). After identifying CPM superior to the diverticulum, diverticulectomy was undertaken, and the cervical esophagus was repaired with 3 layers of manual sutures. A negative-pressure drain was placed, and the incision was closed.
The postoperative nothing by mouth (NPO) period with NG-FT feeding lasted no less than a week until esophageal swallow evaluations with barium or urografin proved no esophageal leaks. Then, NG-FT was removed, and oral liquid diet was resumed.
Follow-up
Patients were followed up every 2 weeks in the first 2 months after surgery for postoperative complications, especially the condition of their deglutition. Then, they were followed up every 6 months.
Results
In total, 3 cases were included: 2 male and 1 female patients, with an age range of 31 to 57 years (average and median ages were 47.3 and 54, respectively). Presenting symptoms included hoarseness, pharyngeal foreign body sensation, and neck mass (Table 1). All 3 LDs were on the left side and discovered accidentally without classic symptoms like dysphagia, halitosis, regurgitation, or coughing. 6
The surgical procedures of all 3 patients were uneventful. We believed the carotid sheath should not be opened to prevent infection resulting from potential postoperative complications like esophageal leak. The NG-FT, inserted immediately after general anesthesia, could serve as good guidance in recognizing the cervical esophagus, as palpation of the tube inside the esophagus could facilitate its recognition. It was worth noting that, since we explored from the inferior surgical field superiorly, we discovered no CPM between the cervical esophagus and the inferior border of the diverticulum. Then, further superior exploration would discover CPM superior to the diverticulum, and a diagnosis of LD could be made.
The recovery of all 3 patients was uneventful. Postoperative esophageal evaluations demonstrated no esophageal leakage 7 to 12 days after surgery, and oral feeding was gradually reinstituted. No mediastinal infection, hemorrhage, or hoarseness resulting from RLN injury was documented.
The duration of follow-up was 8 to 58 months (average and median durations were 38.6 and 50 months, respectively). No recurrence of symptoms or diverticulum was observed, and the swallowing function of all 3 patients was excellent.
Discussion
LD is a very rare disease, and our 3 cases could contribute to the literature by expanding the knowledge about this peculiar condition. Combined with data from the literature, only 7 reported cases are available, with 6 providing useful information.1,2,4 There were 4 male and 2 female patients (31–65 years old) whose average and median ages were 54.5 and 52.7 years old, respectively. Only 2 patients presented with the classic symptoms of dysphagia, regurgitation, and coughing, while the other presenting symptoms included pharyngeal discomfort, foreign body sensation, hoarseness, and neck mass (Table 1). All these patients underwent open surgical management for their LD, resulting in relief of symptoms without complications or recurrence.
ZD is thought to develop secondary to CPM dysfunction, and CPM myotomy is considered fundamental in preventing recurrence. 7 The transoral endoscopic endostapler technique, first introduced in 1993, 8 is currently the most commonly used method.5,9 The critical step in this technique is adequate exposure of the partying septum, which might be difficult in patients with prominent teeth, cervical kyphosis, retrognathia, or temporomandibular joint disease. 5 Both flexible endoscopy and rigid transoral approach have been proven effective in dividing the partying septum between the esophagus and the pouch, restoring the pharyngoesophageal transit. 9 However, in a systematic review including 33 studies (1990 patients) with open diverticulectomy and 22 studies (1089 patients) with endoscopic stapler diverticulotomy, the failure rates of open and endoscopic approaches were 4.2% and 18.4%, respectively. 10 Hence, open surgery is still recommended for patients with diverticulum sizes of <2 cm or >5 cm, and it is more effective in resolving symptoms with minor risks of leaks or fistulas. 11
ZD was classified and named for Friedrich Albert von Zenker in 1877, most commonly affecting elderly individuals (with 50% of patients over 70). Previous studies have estimated it to affect 2 in every 100,000 persons annually, 6 with a male predilection (female/male ratio 1:5). 12 Hence, it surprised us that a young female patient (31 years old) would suffer from cervical esophageal diverticulum. The significantly younger age of LD patients than ZD patients might suggest a different etiology from ZD, which is still unclear. It was more surprising that open surgical exploration revealed her diverticulum to be of the very rare form of LD rather than ZD. Therefore, it is our belief that one of the major merits of open surgery for LD is that it could provide an important differential diagnosis in determining whether the origin of the diverticulum was above or below the CPM. 1 It is not unlikely that previous authors have perceived LD as a variant of ZD and could not effectively differentiate between them without confirmation through open surgical exploration. Therefore, LD might not be as rare as the literature suggests. 2 Indeed, if open surgical management had not been performed, the diagnosis of LD might not have been possible for 5 of the 6 reported cases, except for the case with 2 simultaneously occurring hypopharyngoesophageal diverticula. 2 Additionally, endoscopic procedures (both through a rigid and a flexible endoscope) could had been very difficult (if not impossible) to be carried out, for a diverticulum situated below the CPM. Therefore, it is our assumption that open surgical exploration could be the choice of treatment, for patients with dorsally located pharyngoesophageal diverticula, especially those in economically undeveloped countries with the unavailability of special devices (like Dohlman diverticuloscope or the modified Weerda diverticuloscope) for the rarity of this disease, and the limited resources of their hospitals.
Furthermore, another inherent advantage of open surgical management for LD is the ability to determine whether CPM myotomy is necessary or not. If the diverticulum is determined to be LD, diverticulectomy should be performed, and choice of adding a myotomy of the cervical esophagus beneath the diverticulum should be considered case by case during the operation, even if not always necessary. 1 On the other hand, in endoscopic procedures, this determination cannot be achieved; hence, endoscopic procedures might be associated with an inherent risk of failure. Endoscopic procedures like Zenker’s PerOral endoscopic myotomy (Z-POEM) involve CPM myotomy with distal extension by 1 to 2 cm on the esophageal side to ensure complete dissection. Serious adverse events have been reported in 4/32 patients (12.5%), including 2 leaks and 2 mucosotomies (perforations), as potentially life-threatening complications. 13
So far, traditional flexible endoscopic septotomy has been reported as a well-tolerated and effective treatment for ZD, and novel endoscopic submucosal tunneling techniques, namely Z-POEM and peroral endoscopic septotomy, have been proposed to obtain complete muscular septum exposure and deeper myotomy. 14 But after consultation about the cost and potential complication (especially mediastinitis) with our patients, they all chose the less expensive and safer choice: open surgery.
It is also worth noticing that an open surgical procedure is safe and effective, as demonstrated by the outcomes of our series and literature. In addition, it is our experience that the open surgical procedure is relatively easy to master, especially with the help of RLN monitoring. However, due to the cervical incision and the manual suture of the esophagus, the postoperative NPO period is longer than endoscopic procedures.15,16 And the NG-FT is rather discomfortable for patients, until they could resume oral feeding.
Although the small number of included patients limited our study significantly, this work could draw attention to the accurate differentiation between LD and ZD, which could be achieved in open surgical exploration, and might be crucial in the following choice of treatment regarding whether myotomy on the esophageal side of the diverticulum should be performed or not. Together, our work and cases reported in literature showed that for LD, muscles on the esophageal side of the diverticulum could be left intact, and the prognosis of patients were satisfactory. Hence, our work might contribute to literature. However, so few such cases have been reported that the proposed merits of our treatment algorithm needed validation of larger cohorts.
Conclusion
Open surgical management is a safe and effective approach for LD, which is a very rare clinical entity. In addition, open surgical exploration could further assist differential diagnosis from ZD, by determining the spatial relationship between the origin of the diverticulum and CPM.
Footnotes
Acknowledgements
None.
Author Contributions
Ting-Ting Guo and Yan-Bo Dong reviewed medical records, analyzed data, and participated in patient follow-up. Yu-He Liu made contributions to revising manuscripts. Cheng Lu participated in treatment of patients, and made major contributions to the revising of multiple versions of manuscripts. Wan-Xin Li participated in treatment of patients, reviewed literature, and wrote multiple versions of manuscripts.
Availability of Data and Materials
All data, models, and code generated or used during the study appear in the submitted article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Beijing Hospitals Authority’s Ascent Plan [grant number DFL20220102], and Beijing Friendship Hospital Seed Project, Capital Medical University [grant number YYZZ202125]. National Natural Science Foundation of China for Young Scholars [grant number 82303642], and the Foundation for Scientific Research and Cultivation, Capital Medical University [grant number PYZ22076].
Ethics Approval
The protocol for the research project has been approved by Bioethics Committee of Beijing Friendship Hospital, Capital Medical University.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Institutional Review Board’s approved protocols (2022-P2-404-01).
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.