
Abstract

Statement of Significance
Imbedded hypopharyngeal foreign bodies are urgent complaints commonly presenting to all ENT clinics. Historically, these have been removed under general anesthesia in a hospital setting, though there are many reported cases of successful removal in the outpatient clinic. We present the first case of a swallowed spikelet and a novel approach to removing hypopharyngeal foreign bodies in the office with commonly available ENT instruments. We successfully removed 2 foreign bodies from the hypopharynx with this technique, including the unique plant spikelet foreign body not previously reported in the literature. This technique can help reduce costs, avoid delays to treatment, eliminate risks of general anesthesia, and aid in the appropriate allocation of health care resources.
Pharyngeal and hypopharyngeal foreign bodies are commonly referred to ENT otolaryngologists for evaluation and treatment. There can be significant morbidity and mortality with ingested foreign bodies, including airway swelling, obstruction, infection, and abscess development. Office procedures with topical anesthesia can avoid the increased risks associated with the use of general anesthesia, including high cost, increased time, or other potential complications. Commonly reported hypopharyngeal foreign bodies in the literature include ingested fish bones and wire from a grill brush.1-3 Successful removal of such foreign bodies has been accomplished in the office with topical anesthetics and flexible nasopharyngoscopy in combination with various instruments.1-4
Two consecutive patients presented with hypopharyngeal foreign body globus sensations. The first patient was a 75-year-old male attorney with the above complaint in addition to a sharp, poking sensation when swallowing with throat soreness. His symptoms began after drinking a protein milkshake that, unknown to him, was contaminated with spikelets from a dried, hard, decorative ornamental grass (Figure 1). He denied hemoptysis, hoarseness, or dyspnea. He had been evaluated at our emergency department 5 days prior to our visit for the same complaints; however, no foreign bodies were identified by soft tissue neck X-ray or CT imaging.

Sample of dried, hard ornamental grass.
The second patient was a 54-year-old female who presented with globus sensation and increasing odynophagia for 5 days with worsening sore throat. Her symptoms began after eating shrimp that was cooked on a grill recently cleaned with a wire brush. She denied hemoptysis or upper airway obstruction complaints and did not have any imaging.
After verbal informed consent, we applied topical anesthetics to the nose and oropharynx using 20% Benzocaine oral anesthetic spray and ENT solution nasal spray with 0.05% Oxymetazoline and 4% Lidocaine. Both patients were then examined with a JEDMED (St. Louis, MO, USA) ergo-flex nasopharyngolaryngoscope (NPL) introduced transnasally, identifying embedded foreign bodies and surrounding soft tissue injury to varying degrees. Images were taken using a JEDMED high-resolution video camera and laptop monitor. The first patient had an ornamental grass spikelet in the left tongue base without obvious infection or significant swelling (Figure 2). The second patient had a metal wire embedded in the left tongue base, with significant swelling and infection of the left hypopharynx. There was no airway obstruction in either case.

Ornamental grass spikelet.
The NPL scope was operated by one provider, while a second provider performed simple tongue retraction with gauze while introducing Juarez laryngeal side-biting forceps orally (Figure 3). The forceps were used to palpate and locate the foreign body first. The side-biting jaws were then used to gently extract the foreign body with care to avoid aspiration. Both patients had immediate relief of symptoms following extraction.
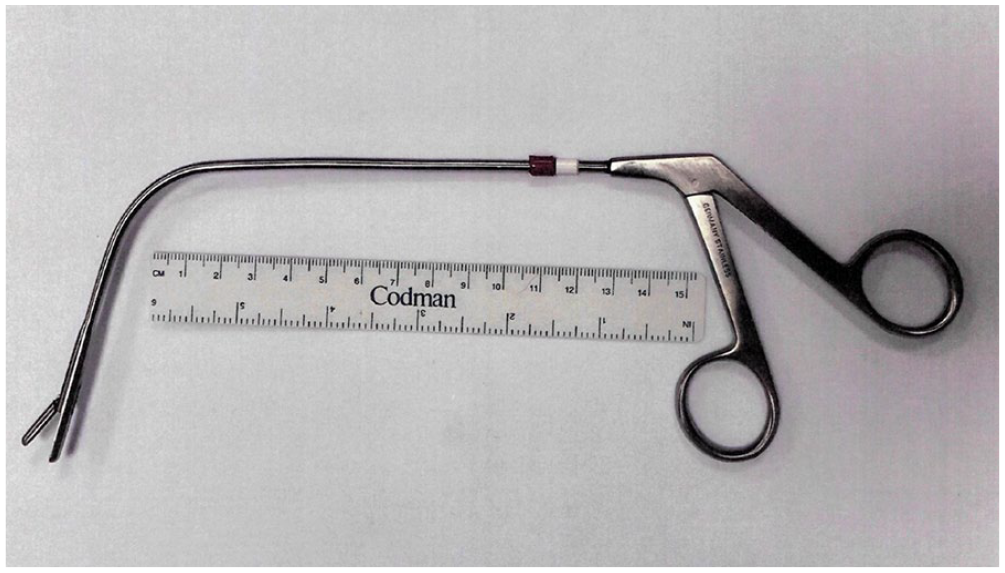
Juarez laryngeal side-biting forceps.
After foreign the bodies were successfully removed, the hypopharynx was reinspected in both patients without significant bleeding identified. The first patient did not have an infection and was advised to use a saline gargle rinse post procedurally. The second patient had significant localized infection, eschar excoriation, and swelling from the metal foreign body and was placed on oral amoxicillin/clavulanate and chlorhexidine gargle mouth rinse post-procedure. Both patients responded well to treatment.
There are multiple reported cases of successful removal of hypopharyngeal foreign bodies in the office under topical anesthesia. Initial techniques reported utilized flexible NPL scopes with working channels and biopsy forceps.1,4 Recent literature has demonstrated successful non-channeled flexible scope with the use of nasal instruments used transorally for foreign body removal. 2 We present the use of a non-channeled scope with Juarez laryngeal forceps used transorally and are unaware of any previous literature demonstrating this use.
Having the right instrument for removal is paramount as ingested foreign bodies can vary in size, shape, and location embedded. Furthermore, there is a narrow window for removal as we are relying on a cooperative patient. Unlike nasal instruments, the Juarez laryngeal forceps have a better design shape for the base of tongue and hypopharynx which means less discomfort for the patient. Most ENT clinics have various instrumentation like this on hand that can be used in combination with standard NPL scopes.
Performing oropharyngeal foreign body removal in the clinic reduces delays in care, eliminates risks of general anesthesia and minimizes costs. Additionally, it is more prudent to perform these procedures in an outpatient setting when possible due to the COVID-19 pandemic. Not all patients are candidates for this, and some will require more intensive care. 5 Treating the appropriate patients in the clinic will decrease the burden on the healthcare system so that healthcare resources can be allocated appropriately.
We present 2 hypopharyngeal foreign body cases that were successfully removed in the outpatient setting using a non-channeled nasopharyngolaryngoscope in conjunction with Juarez laryngeal forceps. We additionally introduce a unique plant spikelet foreign body not previously reported in the literature. This highlights the range of common and unusual foreign bodies that can be removed with carefully considered office-based procedures, thus eliminating the risks of general anesthesia, minimizing time in the operating room, and minimizing health care costs.
Footnotes
Acknowledgements
The authors thank Jessie Casella, MLIS, the librarian at the Department of Veterans Affairs White River Junction Medical Center for her contributions.
Disclaimer
The views expressed are those of the author and do not reflect the official policy or positions of the VHA, DOD, or US Government nor approve or endorse any company products or its services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.