
Abstract

Significance Statement
Trichofolliculoma in the nasal vestibule is rare and can be suspected if the mass has a central pit and a nodular shape. Most trichofolliculomas are asymptomatic but can cause disfiguration; therefore, surgical treatment can be considered. After excision, a histopathological diagnosis can help distinguish it from other skin tumors. This condition does not usually recur; however, long-term follow-up is required if perineural invasion is observed under a microscope.
Trichofolliculoma is a relatively well-differentiated, rare, adnexal hamartomatous follicular tumor originating from the hair follicles. It appears singularly in adults’ heads and necks and was first reported by Miescher in 1944. 1 The external characteristic of a trichofolliculoma is that an umbilical-shaped depression is observed in the center that has the same color as the surrounding skin; there are visible white immature hair bundles.
A 53-year-old man with an 8-month history of a left vestibular mass was referred to our hospital. The patient presented with hypertension, Immunoglobulin A (IgA) nephropathy, polycythemia vera, and gout. Physical examination revealed no skin lesions except for a nodular mass with a smooth surface in the left nasal vestibule. The mass was 0.5 cm in size, smooth-walled, round-shaped with skin color, and with a central pit and multiple immature hairs; there was no pain during palpation (Figure 1). Excisional biopsy was performed under general anesthesia, and the mass was 0.5 cm × 0.5 cm in size, round with clear borders, and showed no adhesions with the surrounding tissues. The pathological report of the mass revealed several large cystic hair follicles, with many small follicles connected radially around them (Figure 2). The wound healed well, and the patient did not experience recurrence during follow-up until 3 months postoperative without any specific complications.
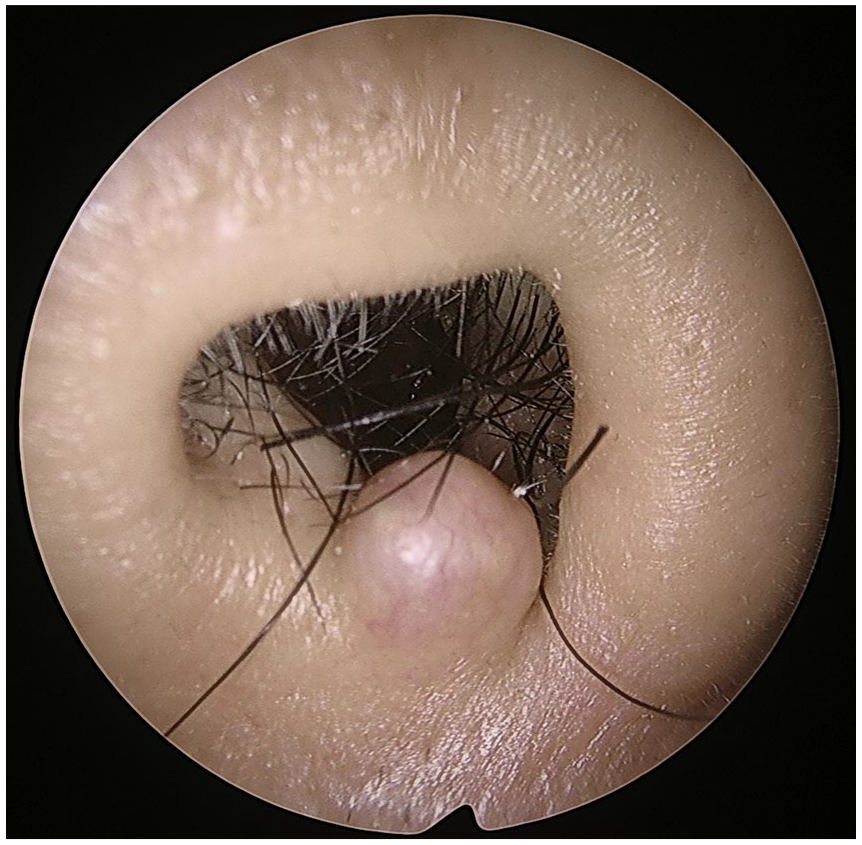
Round nodular non-tender mass of the left nasal vestibule.

(A) Microscopic examination revealed that the cystic lumen contains fragments of hair shaft and keratinous debris (hematoxylin and eosin, original magnification 40×). (B) The tumor has radiating follicular structure associated with fibrotic stroma (hematoxylin and eosin, original magnification 100×).
Trichofolliculoma is prevalent in individuals aged 18 to 49 years, with men having an 84% higher incidence rate than women. 2 Most trichofolliculomas have been reported to occur on the face or scalp and rarely occur in the external auditory canal, intranasal area, genital area, lip, vulva, and upper extremities. 3 Trichofolliculoma shows all stages of hair follicle differentiation and is thought to be located between trichoblastoma and trichoepithelioma. 4 Microscopically, the cystic follicle is lined by a stratified squamous epithelium and communicates with the overlying skin, and secondary small follicles are found around the central cystic follicle. 5
The etiology of trichofolliculoma is not precisely known; however, it seems to be related to previous trauma in the tumor area and is thought to occur due to the discontinuation of the differentiation of pluripotent skin cells toward the hair follicle. 1 Most trichofolliculomas do not require treatment because they have no symptoms. Treatment may, however, be required as disfiguration can occur. Trichofolliculoma treatment involves simple excision, and recurrence is rare.1,3 However, perineural invasion of the cheek has been reported. Although perineural invasion does not suggest malignancy, long-term follow-up may be required when perineural invasion is observed on pathological findings. 6
Trichofolliculoma sometimes has a central depression in hard nodules, such as basal cell carcinoma, and these can be found in various clinical findings from sebaceous adenoma to basal cell carcinoma; thus, histopathological discrimination is essential. 7 The differential diagnosis of trichofolliculoma includes hair follicle nevus, trichoepithelioma, sebaceous cyst, and basal cell carcinoma. Trichofolliculomas are characterized by the intermediate differentiation of hair follicle nevus, which is indicated by simple hyperplasia of hair follicles, and trichoepithelioma, which lacks mature hair follicles. If hair is not observed in a trichofolliculoma, misdiagnosis of a sebaceous cyst, nervus, molluscum contagiosum, or basal cell carcinoma is possible.3,8
Trichoepithelioma is a hamartomatous condition with less follicular differentiation than trichofolliculoma and can be observed as solitary, multiple, or familial lesions. Basal cell carcinoma is a malignant neoplasm arising from pluripotent cells in the basal layer of the epidermis and sometimes occurs in the outer root sheath of the hair follicle. 9 Hair follicle nevus is the most difficult condition to distinguish histologically from trichofolliculoma. It comprises various hair follicles and connective tissues in the subcutaneous fat, with characteristics similar to those of trichofolliculomas. In contrast, trichofolliculomas are characterized by central cysts and radiating hair follicles. Conversely, a lesion may be a hair follicle nevus if radiating hair follicles are not observed.1,5
Footnotes
Author’s Note
We declare that this article is original, has not been previously published, and is not currently being considered for publication elsewhere.
Author Contributions
We confirm that the article has been read and approved by all named authors and that all authors contributed to the study. All the people who satisfied the criteria for authorship are listed. We further confirm that the order of author names mentioned in the article has been approved by all the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study has been approved by the Institutional Review Board of the Jeju National University Hospital.