
Abstract
Introduction
Despite significant advancements of surgical techniques and instrumentation in skull base surgery, any procedure in the upper parapharyngeal space (UPPS), with its complex neurovascular relationships, still carry great challenges.1-5 The anatomical intricacies of the neurovascular structures and relationships in the UPPS have been described in detail. 6 The UPPS is divided into the pre- and retro-styloid compartments by the styloid process and its attachments. 7 Fat, lymph nodes and the deep lobe of the parotid gland are included in the pre-styloid space. This explains the predominance of tumors that arise in the pre-styloid space, such as pleomorphic adenoma, basal cell adenoma, cavernous hemangioma, and rare malignancies. 8 The retro-styloid compartment, however, comprises the parapharyngeal internal carotid artery (ICA), internal jugular vein (IJV), cranial nerves IX to XII, and the superior sympathetic trunk 9 ; and as such, lesions in this compartment are typically schwannomas and paragangliomas. 10
Surgical approaches such as the transcervical, transcervical-parotid, and infratemporal fossa with or without mandibulotomy were traditionally employed for extirpation of tumors in the UPPS.11-13 The endoscopic endonasal and transoral corridor with or without robotic assistance have gained popularity for the resection of select tumors in the UPPS. 14 Given the complex neurovascular relationships, regardless of the approach, surgical procedures within the UPPS carry the risk of bleeding and nerve injury. 15 This risk increases when the lesion is located close to the skull base or its foramens (eg, jugular foramen, external orifice of the hypoglossal canal). Moreover, lesions arising from the retro-styloid compartment have the propensity of displacing neurovascular structures; therefore, increasing the risk of inadvertent intraoperative neurovascular injury.
Previous studies mainly focused their investigation on the parapharyngeal ICA, assessing its course and relationship with tumors arising in UPPS. Subsequently, great efforts to protect the parapharyngeal ICA have led to safer procedures in the UPPS. 16
The wall of the IJV is thinner than that of the ICA, and it is often compressed by the lesions in UPPS. To the authors’ knowledge, however, the relevance and considerations regarding the IJV during the extirpation of tumors in the UPPS has not been described. This may be more consequential for those minimally invasive procedures that follow a medial to lateral trajectory (eg, transnasal and transoral corridors). 17 Therefore, the purpose of this study included the characterization of the IJV in UPPS using cadaveric dissections, and the assessment of pre-operative imaging to define the role of the IJV for a series of patients undergoing procedures within the UPPS.
Materials and Methods
Cadaveric Dissection
To better understand the anatomical relationships within the UPPS, the segment of the IJV traversing the UPPS was dissected in 10 cadaveric heads (20 sides) via an endoscopic endonasal approach. The endonasal approach is valuable for demonstrating the anatomical relationships closing the skull base. Characteristics of the IJV and its anatomical variations in the UPPS were recorded. The study was conducted at the Anatomy Laboratory Toward Visuospatial Surgical Innovations in Otolaryngology and Neurosurgery (ALT-VISION) at the Wexner Medical Center of The Ohio State University in the United States. ALT-VISION and all co-authors were certified by local regulatory agencies dealing with the use of human tissues and cadaveric studies.
Visualization was achieved using rigid rod-lens endoscopes (4-mm diameter, 18-cm length) with 0° lens (Karl Storz Endoscopy; Karl Storz, Tuttlingen, Germany), coupled to a high-definition camera and video monitor. Both video and still digital images were recorded during dissections using the AIDA recording system (Karl Storz Endoscopy; Karl Storz, Tuttlingen, Germany). A high-resolution CT scan was performed before the dissection and the digital imaging and communications in medicine data were exported to a surgical navigation system (Stryker, Kalamazoo, MI, USA).
Clinical Data
From January 1, 2015 to December 31, 2018, the records of 30 consecutive patients who underwent extirpation of tumors arising at the UPPS at Beijing Tongren Hospital were retrospectively reviewed. Informed consent was obtained from all patients, and the study protocol was approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University in China (No. TRECKY2016-036).
Both the computer tomography angiography (CTA) and gadolinium contrast enhanced magnetic resonance image (MRI) scans of these 30 patients had been obtained to evaluate the course of the IJV and its relationship with the tumor and the parapharyngeal ICA.
Among these 30 patients, tumors arose at the pre-styloid space in 18 patients (60%). The remaining 12 patients (40%) harbored retro-styloid compartment tumors. Based on the surgeon’s preference, the tumor in the UPPS was removed via a transoral or transcervial corridor. A total of 24 patients underwent endoscopic transoral resections (80%). Tumors in the remaining 6 patients were removed trans-cervically (20%). The degree of intraoperative exposure and manipulation of the IJV were also recorded.
Results
Cadaveric Dissection
Technical nuances for endoscopic endonasal exposure of the UPPS have been previously described.6,18 After elevation of the lateral pterygoid muscle, the adipose tissue in the pre-styloid compartment was identified (Figure 1A). Following removal of the adipose tissue, the styloid process and its attachments, and the deep lobe of the parotid gland (Figure 1B) were subsequently exposed.
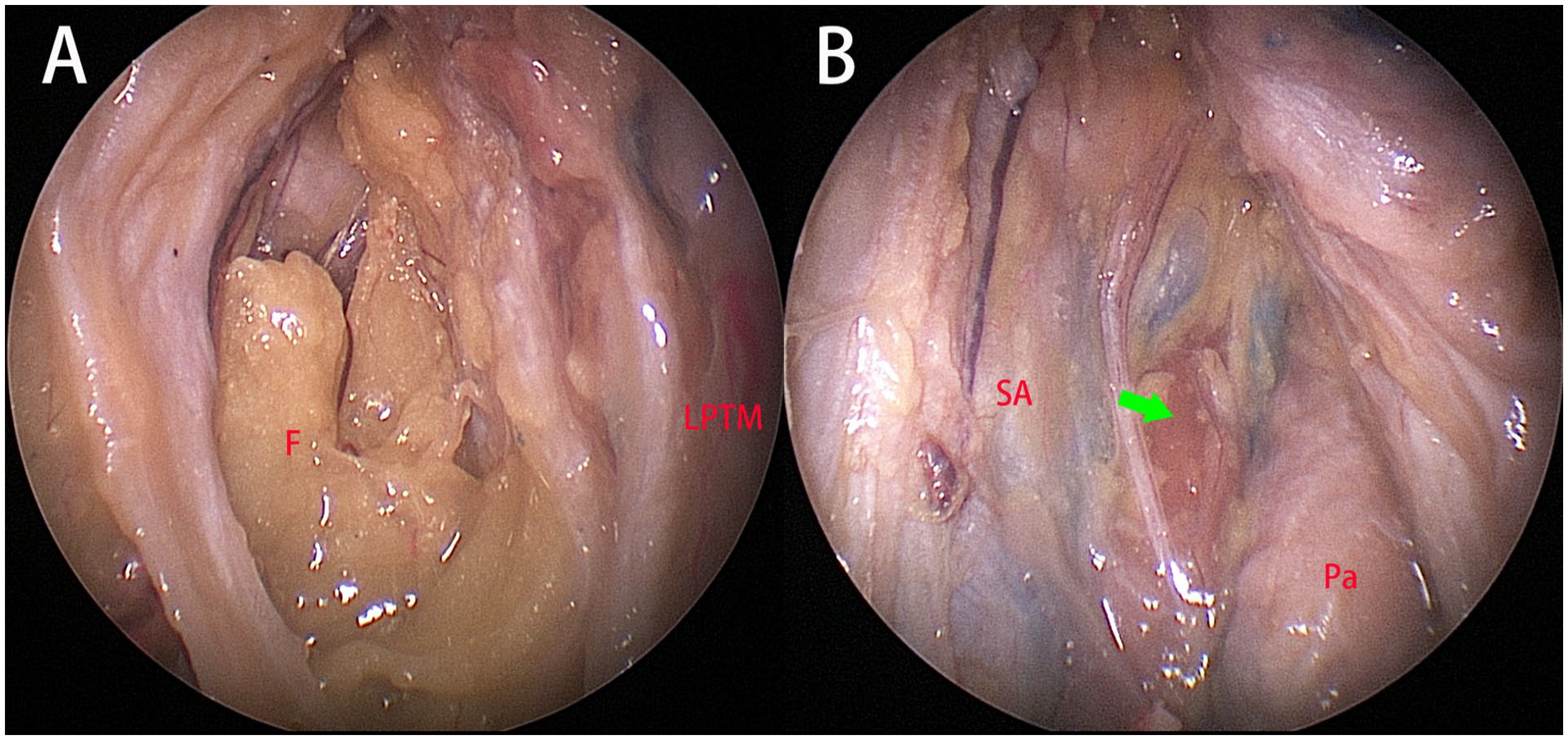
Left side of the specimen, viewed by 0° scope. (A) After laterally displacing the lateral pterygoid muscle (LPTM), the fat (F) in the pre-styloid space was exposed. (B) The deep lobe of the parotid gland (Pa), the stylopharyngeus muscle attached on the styloid process (green arrow), and the sheet-like stylopharyngeal aponeurosis (SA) at the medial aspect of the styloid process were demonstrated.
After dissecting off the stylopharyngeal aponeurosis, the parapharyngeal ICA, glossopharyngeal nerve (CN IX), and the IJV were revealed (Figure 2A). The vagus nerve (CN X) was identified at the posterior aspect of the CN IX, which also lies between the ICA and the IJV; the accessory nerve (CN XI) travels downward posterior to the IJV (Figure 2B). The hypoglossal nerve (CN XII) was clearly revealed after the anterolateral transposition of the parapharyngeal ICA (Figure 2C).
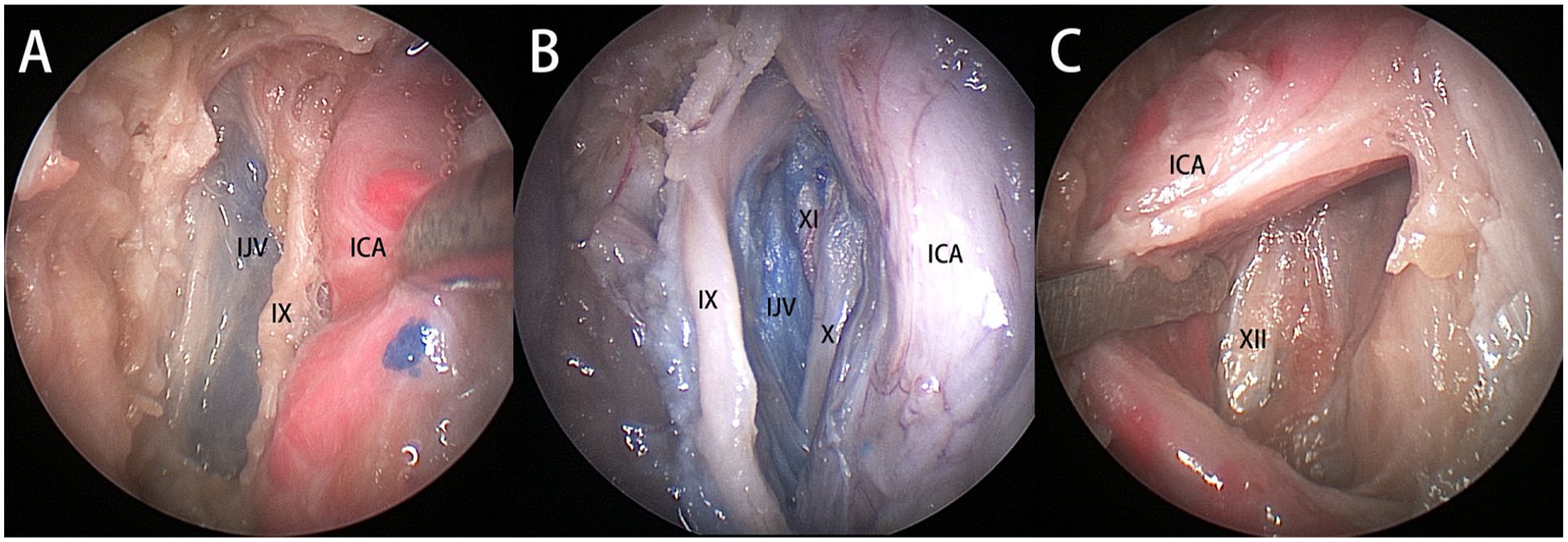
Right side of the specimen, the lateral pterygoid muscle and stylopharyngeal aponeurosis have been removed with part of the styloid process, viewed by 0° scope. (A) The parapharyngeal ICA, glossopharyngeal nerve (IX) and the internal jugular vein (IJV). (B) The glossopharyngeal nerve (IX) lies anterior to the ICA and the IJV, whereas the vagal nerve (X) and accessory nerve (XI) lie posterior to the parapharyngeal ICA and the IJV. (C) After anterior displacing the parapharyngeal ICA, the hypoglossal nerve (XII) located at posterior aspect was observed. ICA, internal carotid artery.
The IJV was identified at the posteromedial aspect of the styloid process in 13 sides (65%, Figure 3A). In the remaining 7 sides (35%), the IJV was detected at the posterolateral aspect of the styloid process (Figure 3B); removal of the styloid process enhance the exposure of the IJV. In all 20 sides no obvious tortuosity of the IJV was detected (Figure 3C). The vaginal process (tympanic part of the temporal bone) was drilled further, exposing the anteroinferior aspect of the jugular bulb (Figure 3D). However, it was not feasible to expose the entire jugular bulb through an endoscopic corridor.
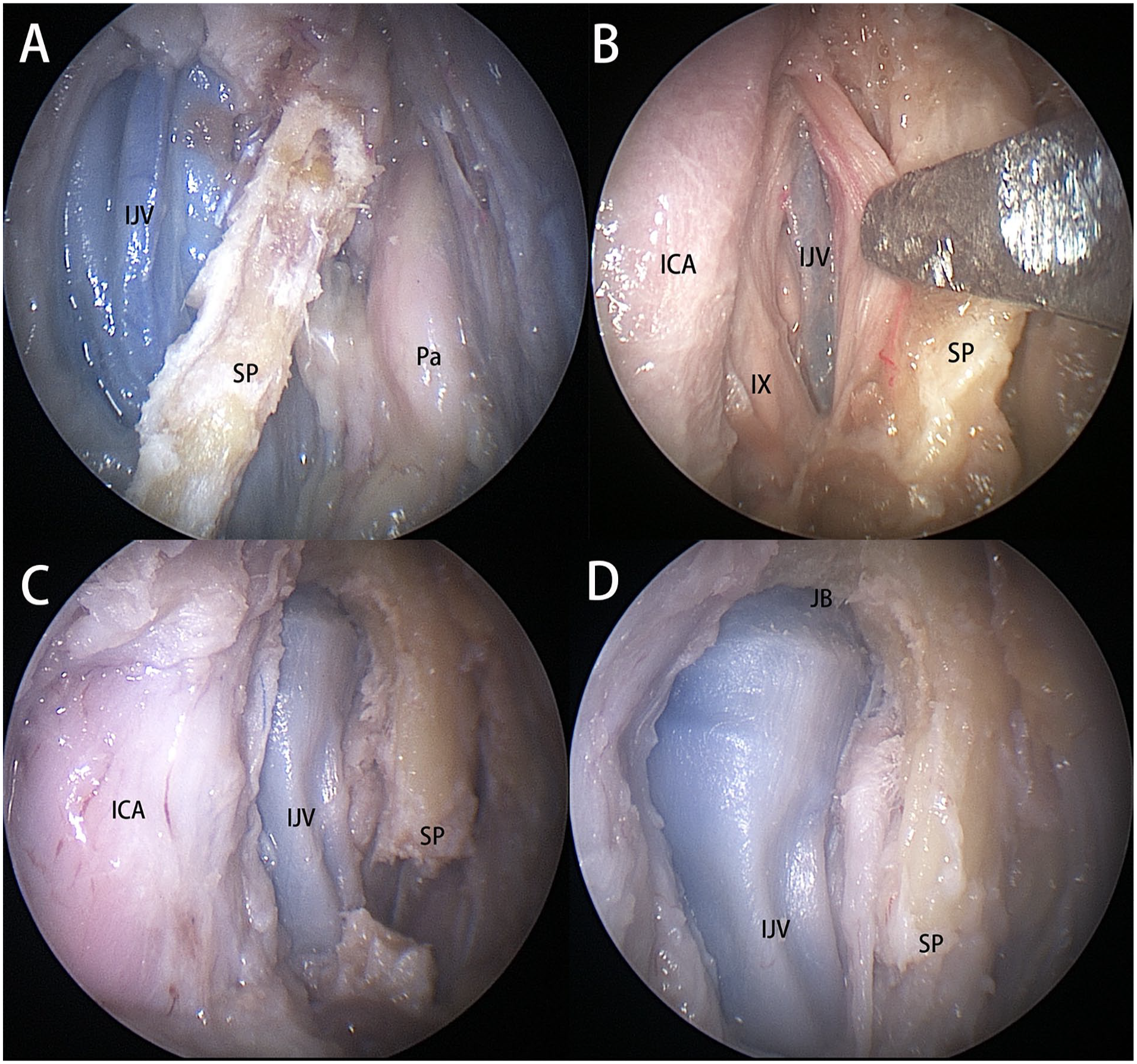
Right side of the specimen, viewed by 0° scope. (A) The internal jugular vein (IJV) lies at the posteromedial aspect of the styloid process (SP). (B) The IJV locates at the posterolateral aspect of the SP. (C) The IJV in the UPPS. (D) The anteroinferior aspect of the jugular bulb (JB) was exposed. Pa, parotid gland; IX, glossopharyngeal nerve.
Radiological Analysis
Both the CTA and MRI could help identify the status of the IJV in pre-operative image evaluation. The IJV in the UPPS ipsilateral to the tumor was observed in a pre-operative CTA or MRI in 23/30 patients (76.67%). In all 18 patients with pre-styloid space tumors, the IJV was identified at the posterior aspect of the tumor (no displacement; Figure 4A). Conversely, CTAs or MRIs in the 12 patients with retro-styloid space tumors, showed the IJV in only 5 patients (41.67%), and in all the vein was plastered against the posterolateral aspect of the tumor, and its patency was significantly compromised (Figure 4B). In the remaining 7 patients, the IJV was totally compressed by the tumors and not identifiable in either the MRI or the CTA.
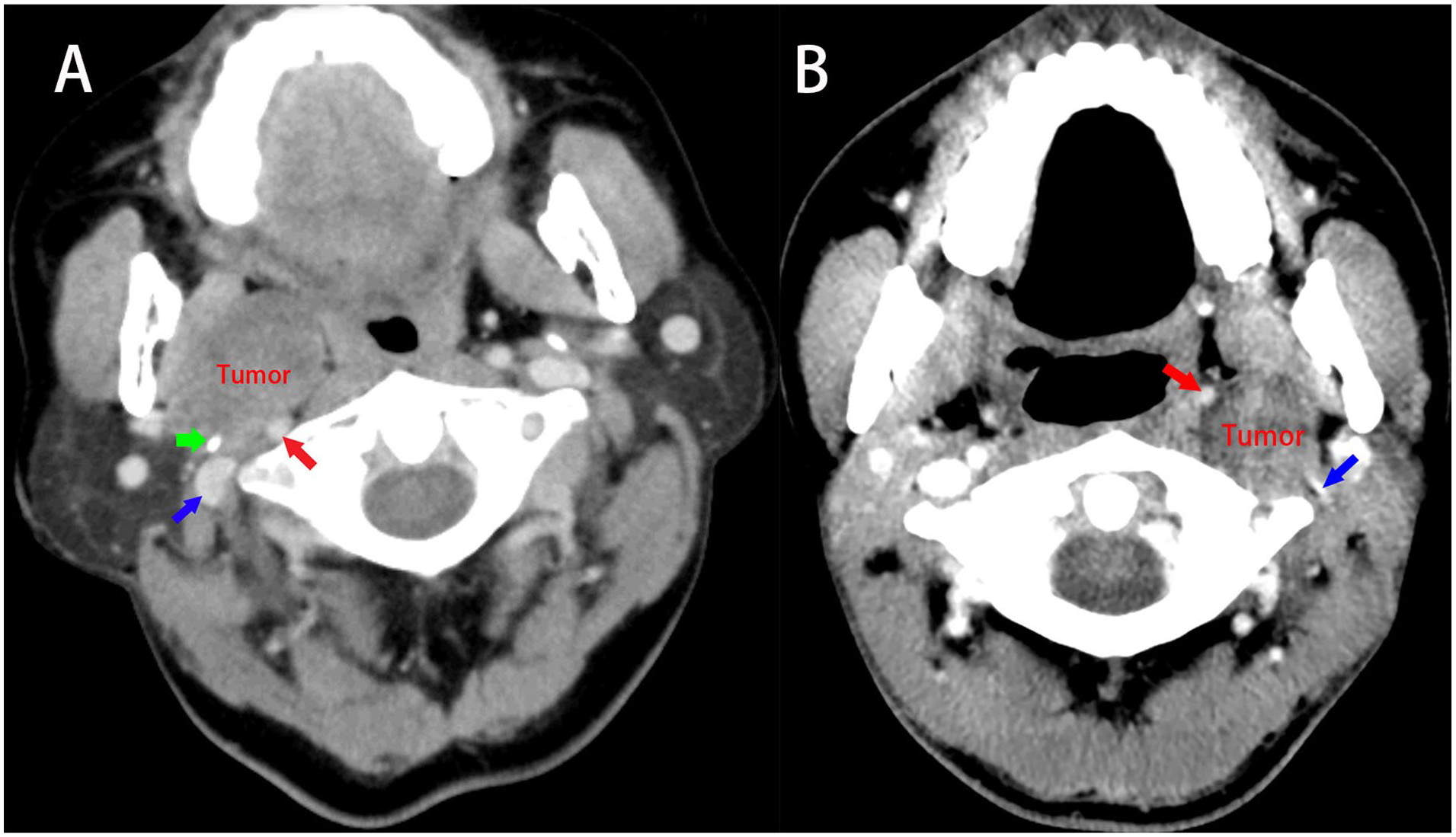
(A) For pre-styloid space tumor, the IJV (blue arrow) lies posterior to the tumor and the styloid process (green arrow), ICA (red arrow) was located at the posterior aspect of the tumor. (B) For retro-styloid space tumors, the ICA was displaced into the anteromedial aspect (red arrow), the IJV was displaced into the posterolateral aspect (blue arrow). ICA, internal carotid artery; IJV, internal jugular vein.
Intraoperative Validation
Of 30 patients harboring UPPS tumors, 24 patients (80%) underwent a transoral tumor resection. This included 18 pre-styloid tumors (pleomorphic adenoma, n = 12; cavernous hemangioma, n = 4; basal cell adenoma, n = 2) and 6 retro-styloid tumors (schwannoma), 18 respectively. The remaining 6 patients (20%) underwent extirpation of the tumor via a transcervical corridor (n = 2, schwannomas) and a transcervical-parotid corridor (n = 4, including 3 paragangliomas and 1 schwannoma).
For open approaches, the IJV was adequately exposed in all 6 patients, ligated in 2 patients with paragangliomas, and no significant bleeding was intraoperatively encountered (Figure 5A). In all 18 patients undergoing transoral resection of tumors in the pre-styloid compartment, the IJV was not encountered intraoperatively, and no significant venous bleeding occurred (Figure 5B). The parapharyngeal ICA was identified to be displaced into the anteromedial aspect of the tumor for patients with retro-styloid tumors (Figure 5C). The tumor was extirpated via an extracapsular en bloc resection in 2 patients. Separation along the lateral and posterior borders was a critical step for avoidance of inadvertent injury of the IJV. For another 3 patients with retro-styloid tumors, the lateral and posterior aspects were clearly exposed after intracapsular internal debulking of the tumor (Figure 5D), and no inadvertent injury to the IJV occurred.
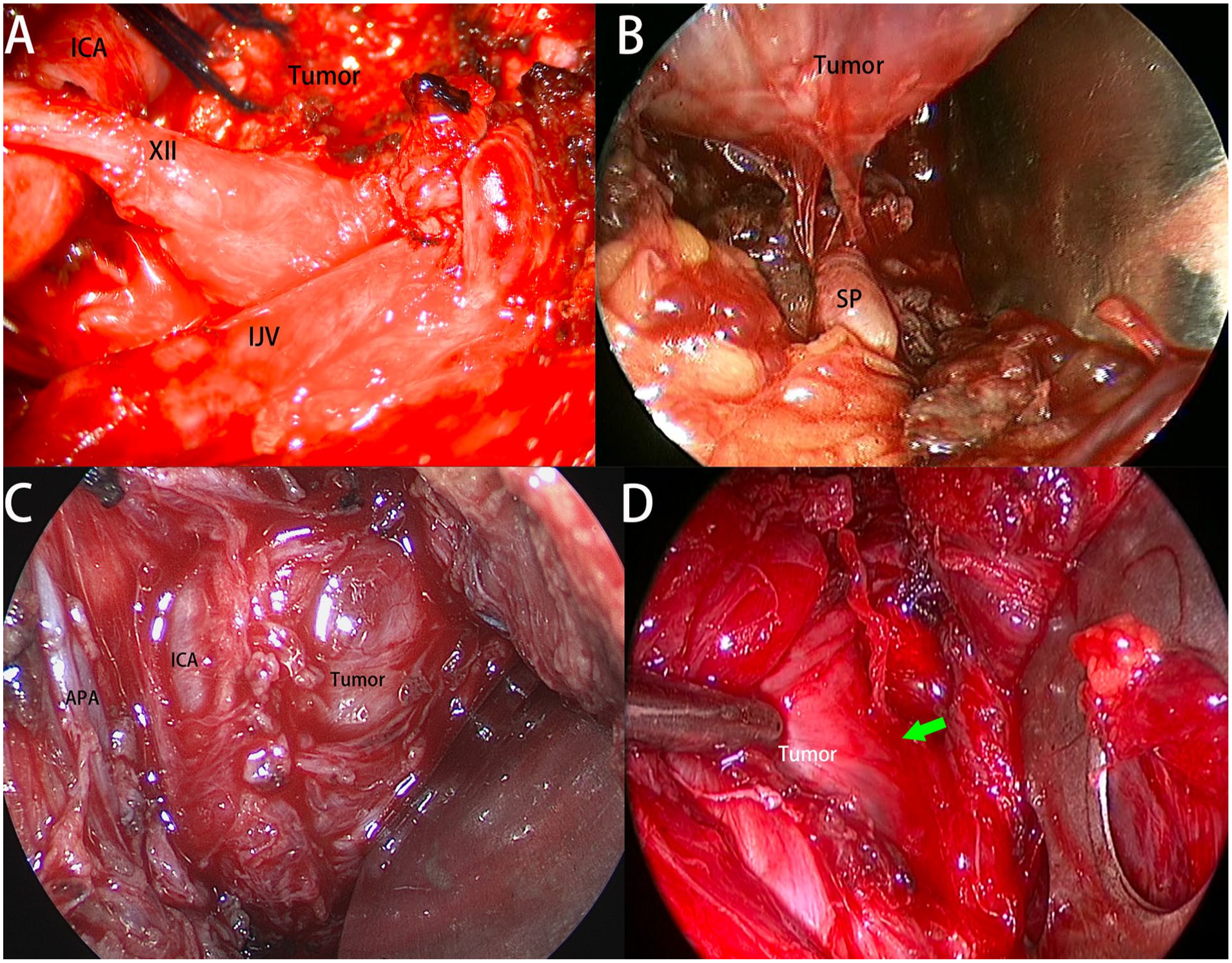
All were from left side. (A) For the open transcervical approach, the internal jugular vein (IJV) was sufficiently exposed. (B) The extirpation of tumors arising from the pre-styloid space limited prior to the styloid process (SP). (C) For retro-styloid space tumor, the ICA was displaced into the anteromedial aspect of the tumor. (D) After internal debulking, the lateral and posterior borders (green arrow) were identified and bluntly separated. APA, ascending pharyngeal artery; XII, hypoglossal nerve; ICA, internal carotid artery.
However, in the remaining patient undergoing transoral resection of the schwannoma in the retro-styloid compartment, copious bleeding was encountered intraoperatively upon dissecting the posterolateral facet of the tumor, rapidly losing around 1100 ml. The oral cavity was packed and the transoral approach was aborted and immediately converted into an open approach. The site of injury at the IJV was identified and the vessel was subsequently ligated through the transcervical approach, and a complete extirpation of the tumor followed and uneventful course.
Discussion
The IJV in the UPPS has a larger diameter and thinner wall than the parapharyngeal ICA. 19 Inadvertent rupture of the IJV may result in catastrophic bleeding during minimally invasive procedures (eg, endoscopic transnasal or transoral approach). 20 This is especially true when the injury occurs close to the skull base and can be very challenging to manage. Previous publications have mainly focused on investigation and protection of the parapharyngeal ICA for surgical procedures in the UPPS. Through description and analysis of the anatomical relationship between the UPPS tumor and the IJV, this study enhances the understanding of the relevance of the IJV during surgeries in the UPPS, also improving the safety of minimally invasive procedures.
During open approaches (ie, transcervical, transcervical-parotid, infratemporal fossa approach) accessing to the UPPS, both the parapharyngeal ICA and the IJV could be adequately exposed. 21 Direct visualization is helpful for preservation or control of the IJV via a lateral approach. 22 In this cohort, no rupture of the IJV and copious bleeding was encountered when dissecting the tumors through a transcervical or transcervical-parotid corridor. In 2 patients, the IJV was adherent to paragangliomas arising in the retro-styloid compartment requiring ligation to facilitate exposure, with no associated complications. Therefore, injury of the IJV does not appear to be a major concern during a transcervical approach to extirpate tumors arising from the UPPS even when the tumor intimately adheres to the vein.
Pleomorphic adenoma arising from the deep lobe of the parotid gland is commonly encountered in the pre-styloid UPPS. 23 A transoral corridor may be appropriate for resection of select benign tumors arising in the pre-styloid compartment.24,25 Cadaveric dissection in the present study found that the IJV was located posterior to the styloid aponeurosis; thus, the risk of IJV injury is very low for procedures restricted to the pre-styloid space. The anatomical findings were clinically confirmed in 18 patients with pre-styloid UPPS tumors resected via a transoral corridor without meeting the IJV.
For any surgical procedure in the UPPS, identification and protection of the parapharyngeal ICA is of paramount importance, 8 which is especially true for management of lesions originated from the retro-styloid compartment. 18 Schwannoma and paraganglioma are more commonly encountered in retro-styloid space. 26 The parapharyngeal ICA was often displaced into the anteromedial aspect for those tumors arising within the retro-styloid compartment. 18 While it is not an absolute contraindication to perform a transoral approach for resection of retro-styloid space tumors, only a team with significant experiences in skull base and infratemporal fossa surgery should tackle such an endeavor to safely remove select retro-styloid tumors after careful identification and protection of the parapharyngeal ICA. 18
Publications regarding the location and significance of the IJV and its relationship with the tumors of the retro-styloid space are sparse. Both the CTA and MRI could help distinguish the status of the IJV through pre-operative assessment, and the 2 methods functioned complementary to each other. For evaluation of the tumor essence (eg, component, blood supply), however, the MRI are better for identification than the CTA. Based on findings derived in the present study, the IJV was found to be partially or totally compressed and displaced into the posterolateral aspects of the tumor for patients with retro-styloid tumors. In our opinion, identification of the tumor capsule and careful blunt separation along the lateral and posterior borders of the tumor are critical steps to avoid injury of the IJV, no matter what the technique of separation is, whether by an extracapsular or an intracapsular fashion. However, risk of the IJV rupture remains and indeed occurred in 1 patient in this cohort.
The jugular bulb and the upper segment of the IJV are difficult to control and address via a minimally invasive approach (ie, endonasal or transoral corridor). 27 For lesions surrounding or infiltrating the jugular bulb and upper segment of the IJV (eg, paraganglioma, meningioma, malignancies), it is contraindicated to employ a transoral or transnasal extirpation from a medial toward lateral trajectory. 28 The infratemporal fossa approach type A or a far lateral corridor may be well indicated for this scenario.
This study contains significant limitations. As the cadaveric dissections were performed via an endoscopic transnasal approach in a cadaveric lab in the United States, while the clinical tumor removal was mainly performed through the transoral or open approaches in a Chinese institution. Therefore, a significant bias existed among the different approaches. However, description of the anatomical relationships and principles regarding the IJV involved in the UPPS are sound. Likewise, the orientation and the perspective regarding the anatomical relationships within the UPPS via a transoral corridor has also been demonstrated in our previous publication,29,30 which did not show much difference with those conducted through the transnasal approach. 6 Moreover, a transnasal dissection is much better for describing the anatomical relationships between the IJV and the other neurovascular bundles close to the skull base, in comparison with a transoral or an open corridor. Furthermore, it is still difficult to directly expose the IJV for transoral or transnasal procedure within the UPPS, and as such, the relevance of the IJV conducted through these minimally invasive corridors still deserves further validation.
Conclusion
The characteristics of the IJV and its relationship with adjacent neurovascular structures in the UPPS were described, providing additional safeguards to surgeries in the UPPS.
Footnotes
Authors’ Note
Abstract was accepted as poster presentation at the Chinese Annual Meeting of Otolaryngology Head and Neck Surgery, Zhengzhou, November 2022.
Data availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N. London holds stock in Navigen Pharmaceuticals and was a consultant for Cooltech Inc. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.