
Abstract
Introduction
Nasal airway obstruction (NAO) is a common condition among patients in otolaryngology practices and is characterized by limited airflow through the nose. 1 This condition is often associated with multiple symptoms including difficulty breathing, poor quality of sleep, and a reduced quality of life. 2 NAO can result from many factors, including sinonasal inflammatory disorders and anatomic causes. 3 Many times, patients may not know that their nasal breathing problems are due to NAO or even recognize it as a condition that can be treated.
Anatomical Contributors of NAO
When considering causes of NAO, it is important to understand the role and relative importance of potential anatomic contributors as well as the fact that many, if not most, patients with NAO have more than 1 contributing cause of NAO.3–5 The nasal valve, sometimes referred to as the internal nasal valve, is the narrowest part of the nasal airway and, according to Poiseuille’s Law, even small reductions in this area can substantially limit nasal airflow. The nasal valve is bounded laterally by the caudal margin of the upper lateral cartilage (lateral wall), anteriorly by the head of the inferior turbinate, and medially by the nasal septum. (Figure 1). Nasal valve dysfunction with lateral nasal wall collapse is often referred to as nasal valve collapse (NVC). NVC can be further classified as static (no lateral wall movement) and/or dynamic (lateral wall movement during inspiration). Patients may have NVC that occurs as unilateral or bilateral static, dynamic, or a mix of both.5,6
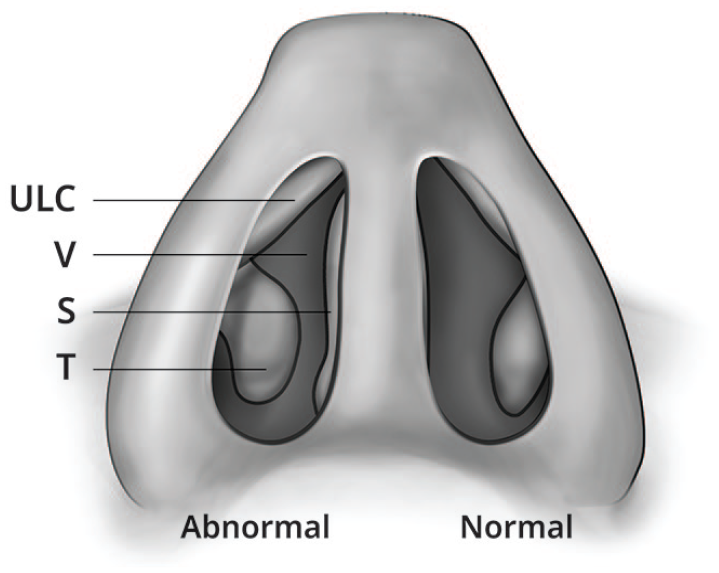
Nasal valve anatomy (internal), showing the abnormal right and normal left internal nasal valves (V): the space bounded by the caudal aspect of the upper lateral cartilage (ULC), the anterior part of the inferior turbinate (T), and the nasal septum (S).
A previous large US-based survey of patients complaining of severe/extreme NAO showed a high prevalence and multifactorial contribution of anatomic anomalies such as septal deviation (80%), NVC (73%), and inferior turbinate hypertrophy (77%). 4 A recently published study also shows a strong association between the presence of septal swell body hypertrophy and the severity of NAO symptoms. 7
Diagnosis of NAO
Physical Exam
Despite common patient complaints about symptoms related to NAO, nasal examinations historically have not evaluated all contributors to NAO, such as NVC. Due to the many potential anatomic contributors to NAO, nasal exams should include evaluations of the lateral wall of the nasal valve, as well as the septum, septal swell body, and inferior turbinate.3,8 Ideally, the nasal valve should be inspected prior to insertion of the nasal speculum to avoid falsely opening (and bypassing) a narrowed nasal valve. Additionally, conducting a portion of the nasal exam prior to the use of a nasal decongestant can help assess the swelling of soft tissue structures (e.g., inferior turbinates, septal swell bodies) in their normal state.3,8
Cottle and Modified Cottle Maneuvers
Patients who present with decreased nasal air flow and suspicion of changes in the nasal valve angle or compromise can be evaluated by the Cottle maneuver (Figure 2a) or modified Cottle maneuver (Figure 2b). The traditional Cottle maneuver is a simple test using the fingers on the cheeks and pulling laterally to see if nasal inspiration improves. The modified Cottle maneuver, a more precise maneuver, assesses the lateral cartilage support by using a curette or similar instrument to gently support the lateral wall while the patient inspires. If nasal breathing improves during either of these maneuvers, the test is positive for potential contribution of the lateral wall to the NVC. Inclusion of these tests can aid in a shared decision-making approach to identify a solution based on patient preferences.
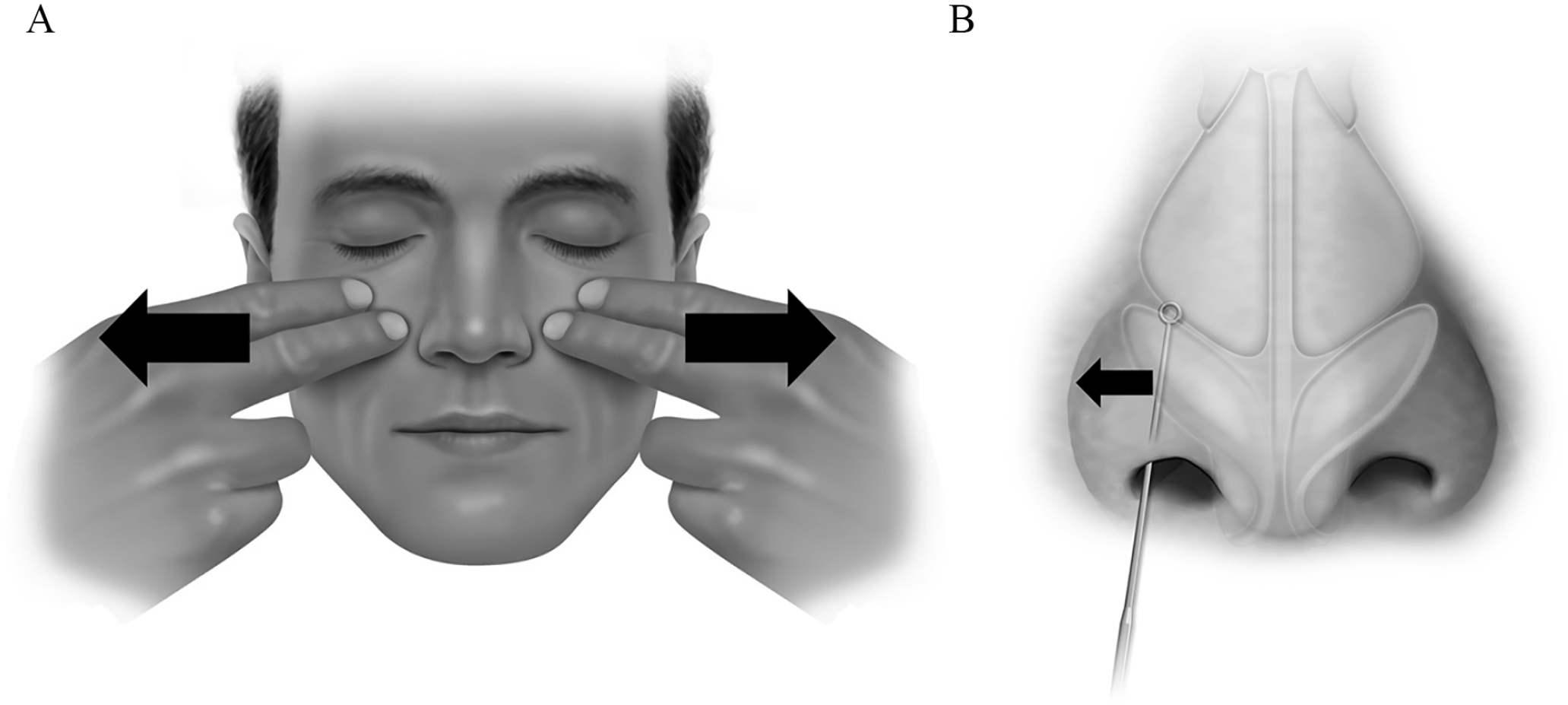
(A) Cottle Maneuver: The physician or patient temporarily lifts and lateralizes the skin around nose and cheek, increasing the nasal valve angle. (B) Modified Cottle Maneuver: Manual lateralization of the nasal valve with a rigid instrument to test for the lateral nasal wall’s contribution to nasal valve dysfunction.
Home Assessments
To complement the initial consultation and physical exam where NAO is suspected, physicians can choose to send patients home with additional instructions to better understand their contributors to NAO. These home assessments typically include trials of nasal breathing strips/intranasal dilators and decongestant sprays, with the patient reporting back effectiveness in improving nasal breathing. Alternating tests can help identify independent contributors to NAO, with at least 1 day trialing each test by itself, and 1 day using a combination (Table 1).
Home Nasal Airway Obstruction Assessment Measures.
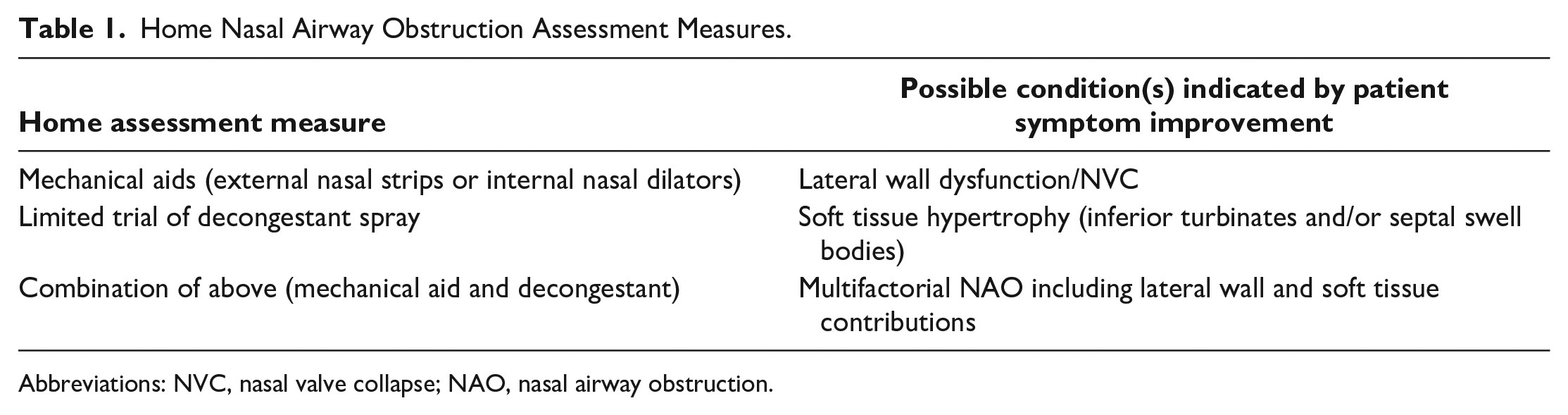
Abbreviations: NVC, nasal valve collapse; NAO, nasal airway obstruction.
As is the case during an evaluation in the clinic, these assessments are a continuation of the shared decision-making process, which is a potential solution for improving quality of care. 9
NOSE Scale Patient Intake Form
The Nasal Obstruction Symptom Evaluation Scale (NOSE), a validated, disease-specific quality of life instrument, was developed to help address some of the diagnostic shortcomings of a traditional nasal exam and allow for a subjective evaluation of nasal obstruction. 10 The NOSE Scale is a five-item, 100-point symptom severity questionnaire: mild (5-25); moderate (30-50); severe (55-75); and extreme (80-100). The NOSE Scale is a reliable, validated instrument for patient-reported symptoms when used for NAO evaluation. 10 Building upon a previously reported survey study that focused solely on sinonasal patients, 4 the purpose of this study was to evaluate the impact of incorporating the NOSE Scale assessment as part of general all-comers otolaryngology patient intake activities to identify patients with NAO.
Patients and Methods
This large, physician practice descriptive survey was conducted in a real-world setting of 149 general otolaryngology clinics geographically distributed throughout the United States. No patient identifying data were collected, therefore Institutional Review Board and informed consent were not required. Clinic staff administered the NOSE Scale assessment consecutively to patients who presented to the clinic over a 1-week period, regardless of the reason for the visit. The patients completed the NOSE Scale, assessing the degree to which various symptoms were a problem for them over the prior 4 weeks. As categorical variables, the NOSE Scale scores, NOSE severity categories, and the primary reason for the clinic visit were summarized using frequencies and percentages.
Results
Survey data were collected for 3533 individual patient visits. The overall mean NOSE Scale score was 37.6 (SD 31.5), indicating moderate NAO for the overall population. Approximately one-third [37.4% (1320/3533)] of the patients had severe or extreme symptoms of NAO, 15.5% (547/3533) had moderate symptoms, 28.7% (1015/3533) had mild symptoms, and 18.4% (651/3533) of patients did not have NAO symptoms (Figure 3).
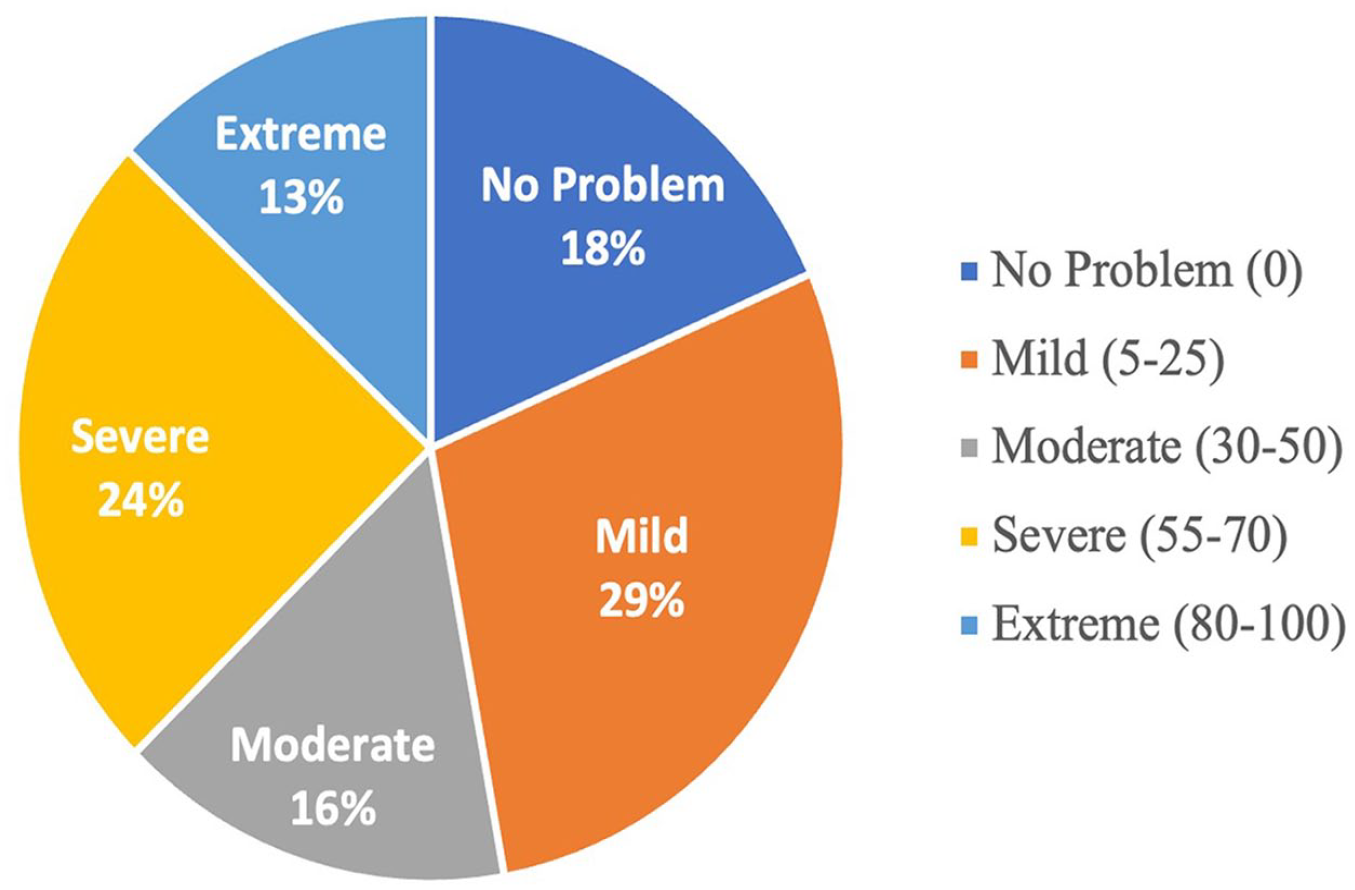
Percentage of patients by NOSE severity class for all visit types (N = 3533).
The primary patient complaint for each clinic visit was categorized as related to “NAO,” “Sinus,” or “Other” complaints. The most common visit category was “Other” (61.2%, 2162/3533), followed by “NAO” (22.6%, 798/3533) and “Sinus” (16.2%, 573/3533). The mean NOSE scores for patients in each of the visit categories were 23.4 (SD 25.9), 64.7 (SD 23.3), and 53.3 (SD 28.1), for “Other,” “NAO,” and “Sinus,” respectively. In the cohort specifically coming in with “NAO” or “Sinus” as a primary complaint,76.2% (608/798) and 57.2% (328/573) had severe or extreme NOSE scores, respectively. Figure 4 shows the distribution of NOSE scores by severity category for each category of visit complaints.
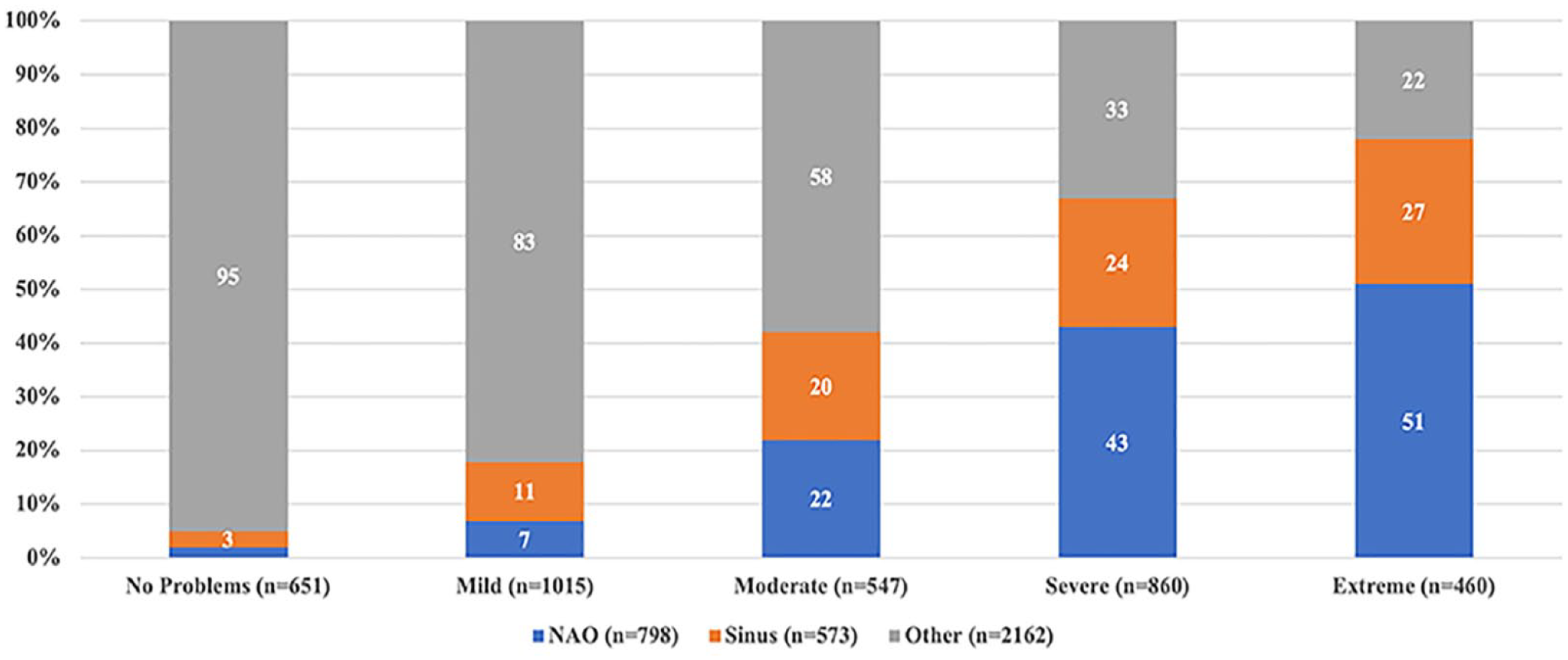
Percentage of patients by visit type and NOSE Scale severity category (N = 3533).
The “Other” visit category was further broken down into the following subcategories: Allergies/rhinitis/congestion, Ear (e.g., wax removal, otitis, hearing evaluations, tinnitus), Nose (i.e., epistaxis, polyps, olfactory dysfunction), Throat (e.g., tonsillitis, dysphagia, thyroid nodules), Oral (sialolithiasis, mouth, or tongue lesions), Preoperative/Postoperative examinations, Sleep (e.g., snoring obstructive sleep apnea), Miscellaneous (e.g., headaches, dizziness, mass evaluation), and Unknown. Of these, the Allergies/rhinitis/congestion, Nose, Pre/Postoperative Exam, Sleep, and Unknown subcategories all had 20% or more of patients with severe or extreme NAO (Figure 5).
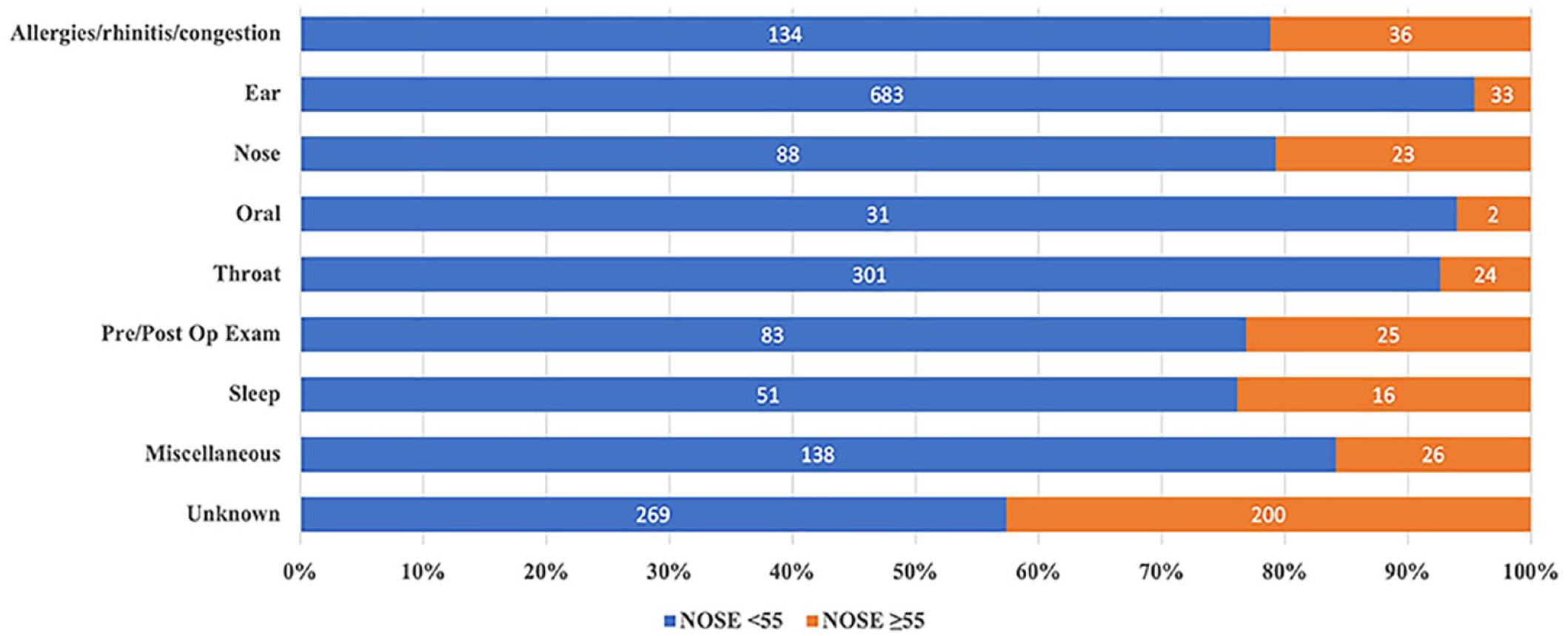
Percentage of patients by “Other” subgroup and NOSE Scale severity (N = 2162).
Discussion
This present study identified a high prevalence (37.4%) of severe and extreme symptoms of NAO, among general ENT patients—even if their main reason for the clinic visit was not specifically related to NAO (e.g., “Sinus” or “Other”). Analysis of the data based on the primary reason for clinic visit revealed some interesting findings. As expected, the patients who reported “NAO” and “Sinus” as their primary complaints had higher NOSE scores with 68.3% (936/1371) falling into the severe/extreme category; this percentage is in line with previously reported data. 4 On the other hand, looking specifically at the group coming in for non-NAO/non-sinus reasons, 14.7% (318/2162) were in a moderate NOSE severity class and another 17.8% (384/2162) had severe to extreme NAO, indicating that one-third of these patients could suffer from symptomatic nasal obstruction even when this was not their main complaint. The findings of this study indicate that there are likely many patients presenting to otolaryngology clinics with symptomatic NAO who may not mention their symptoms. Assuming that an average US otolaryngologist sees 277 outpatient visits per month 11 and applying the prevalence of severe/extreme NOSE severity (37.4%) derived from this study, an approximate 100 patients per month from surveyed physician practices could potentially fall into this highly symptomatic NAO category. This translates into a lot of possible missed NAO patients, especially in high-volume practices, that ENT physicians could be helping otherwise with a multitude of treatment options currently available. A lot of these patients may be used to their symptoms and do not bring them up with their doctor because they may think there are only invasive treatment options available. If physicians can discuss their NAO in more detail with them, they can educate them about less invasive treatment options available and alleviate some of their suffering.
The American Academy of Otolaryngology—Head and Neck Surgery (AAO-HNS) recently published a position statement recognizing surgical repair of the nasal valve as a distinct procedure that can improve symptoms of nasal obstruction for appropriately selected patients with nasal valve collapse. 12 The AAO-HNS position statement recommends a shared decision-making approach when feasible between the clinician and patient to review the available treatment options and ensure a well-informed and practical plan of action. The statement cautions that septoplasty or inferior turbinate reduction alone without repair of the dysfunctional nasal valve could result in incomplete symptom resolution and unnecessary additional surgical encounters. In addition to traditional septoplasty and inferior turbinate reduction surgeries, there are now less invasive treatment options, available in either office or surgical settings, that have been shown to be effective in treating NAO due to NVC, with some studies showing long-term benefit for as long as 4 years.13–16
Approximately half of the patients in the otolaryngology clinics surveyed experienced symptomatic NAO. This surprisingly large proportion includes all patients, regardless of their primary reason for visit. It is well recognized that NAO can negatively affect many aspects of a patient’s life including, but not limited to, difficulty in sleeping, experiencing nasal congestion, and struggling to breathe through the nose during exertion or exercise.2,17 Improving NAO identification can open the door to further evaluation and discussion of treatment options for patients. In addition to the NOSE Score, there are many additional options for assessing NAO and NVC, including visualizing the nasal valve and associated soft tissue structures prior to decongestant spray, using a Cottle/modified Cottle maneuver, asking patients about nasal breathing difficulties, and using at home assessments.
To our knowledge, the prevalence of NAO in the general otolaryngology outpatient clinic population has not been established. Prevalence is an important and useful measure of the burden of disease. Understanding the prevalence of NAO, a condition associated with untoward health effects, enables the clinician to better understand the burden of this condition in their own population, thereby raising awareness and providing them with an opportunity to address it clinically to improve their patients’ well-being.
Furthermore, this article provides important information regarding the prevalence of NAO in otolaryngology patient populations that can be useful for further study and forward planning for activities such as estimating outcomes for population-based interventions, studying health resource utilization, and performing health economic assessments to compare various NAO treatment options.
Conclusions
The findings of this large, descriptive otolaryngology practice survey found a high prevalence of moderate to severe/extreme NAO among general patient populations presenting to otolaryngology practices. Incorporating assessments, such as the NOSE Scale score, a Cottle/modified Cottle maneuver and other diagnostic practices into the patient intake workflow and examination, may help identify symptomatic NAO patients who may otherwise be overlooked.
Footnotes
Acknowledgements
Writing assistance provided by Megan Shen, Ph.D., an independent consultant of Aerin Medical. Support for medical writing was provided by Aerin Medical.
Correction (September 2023):
Article updated to make a small correction in Results section of the Abstract.
Data Access
Data will not be made available in a public repository; however, it may be made available upon reasonable request made to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Raithatha is a consultant for Aerin Medical.
Dr. Del Signore has no declarations of conflicting interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Aerin Medical.