
Abstract
Acoustic neuromas are the most common tumor of the cerebellopontine angle that are associated with a number of symptoms that negatively impact a patient’s quality of life. While the mainstay of treatment for these benign tumors remains microsurgical resection, there is limited research exploring how certain modifiable risk factors (MRFs) may affect the perioperative course. The purpose of this study was to investigate how MRFs including malnutrition, obesity, dyslipidemia, uncontrolled hypertension, and smoking may affect postoperative rates of readmission and nonroutine discharges. We utilized the 2016 and 2017 Healthcare Cost and Utilization Project Nationwide Readmissions Database. MRFs were queried using appropriate International Classification of Diseases, Tenth Revision (ICD-10) coding for categories including malnutrition, obesity, dyslipidemia, smoking, alcohol, and hypertension. The statistical analysis was done using RStudio (Version 1.3.959). Chi-squared tests were done to evaluate differences between categorical variables. The Mann–Whitney U-testing was utilized to evaluate for statistically significant differences in continuous data. The “Epitools” package was used to develop logistic regression models for postoperative complications and post hoc receiver operating characteristic curves were developed. Pertaining to nonroutine discharge, predictive models using malnutrition outperformed all other MRFs as well as those with no MRFs (P < .05). In the case of readmission, models using malnutrition outperformed those of obesity and smoking (P < .05). Again, an increase in predictive power is seen in models using dyslipidemia when compared to obesity, smoking, or uncontrolled hypertension. Lastly, models using no MRFs outperformed those of obesity, smoking, and uncontrolled hypertension (P < .05). This is the first study of its kind to evaluate the role of MRFs in those undergoing surgical resection of their acoustic neuroma. We concluded that certain MRFs may play a role in complicating a patient’s perioperative surgical course.
Keywords
Introduction
Acoustic neuromas are benign tumors of cranial nerve VIII that can cause various clinical symptoms such as hearing loss, tinnitus, vertigo, ataxia, and headache. 1 Although the occurrence rate of these tumors is relatively low (1.4 per 100,000), they can significantly affect the patient’s quality of life, and thus, many patients elect to undergo microsurgical resection. 2 To date, there remains a limited body of research analyzing the effects of modifiable risk factors (MRFs) on postoperative outcomes for those patients opting to undergo surgical resection of their acoustic neuroma. Broadly, MRFs can be stratified into 3 categories: vascular, substance abuse, and nutrition.3-6 While there may be cause and effect relationships within these categories, they may also have their own unique impact on patient’s postoperative course. Understanding how MRFs are related to perioperative complications, and thus readmissions and nonroutine discharges may guide clinicians in tailoring care to best suit their patients.
Previous literature has examined certain non-MRFs and their impact on perioperative complications. One study comparing frail to non-frail patients, found that frail patients had statistically significant increased rates of a number of perioperative complications and readmissions following microscopic resection of their acoustic neuroma. 7 While non-MRFs are important for surgeons to consider in the perioperative period, MRFs are of particular importance because of their ability to be mitigated through certain lifestyle interventions.
Understanding how MRFs may contribute to perioperative complications can assist surgeons in deciding whether to adopt a conservative approach or addressing MRFs prior to surgery, especially given these benign tumors do not necessitate immediate intervention. 8 Obesity has been heavily researched for its link to cerebrospinal fluid leak following microscopic resection of acoustic neuromas, and has also been associated with postoperative myocardial infarction and wound infection.9-12 Although hypertension and dyslipidemia have not been studied in this context, perioperative hypertension and dyslipidemia, in noncardiac surgeries has been linked to increased hospital stay as well as morbidity and mortality.13-15 Finally malnutrition has also been associated with postoperative morbidity, mortality, increased length of stay (LOS), readmission rates, and overall hospital costs.16-18 The objective of this study is to do an analysis of MRFs and their effects on postoperative outcomes in frail patients undergoing acoustic neuroma resection using the national readmission database.
Methods
This study utilized the 2016 and 2017 Healthcare Cost and Utilization Project Nationwide Readmissions Database (NRD) to examine hospital readmissions and mortality rates. The database contains verified patient linkage numbers, which maintain patient privacy and aim to follow patients across hospitals through various states.
International Classification of Diseases, Tenth Revision (ICD-10) codes were used to select patients with acoustic neuromas (ICD-10: D33.3) and those patients who had underwent surgical intervention for resection of their tumor (ICD-10: 00BN0ZZ). Patient frailty in the subpopulation was evaluated using the Johns Hopkins Adjusted Clinical Groups (JHACG) frailty-defining diagnosis indicator, which assess a patient’s frailty using a number of ICD-10 codes related to comorbidities and phenotypic criteria. These include dementia, malnutrition, vision impairment, difficulty ambulating, decubitus ulcer, history of fall, urine or fecal incontinence, weight loss, and social support. A patient who is identified to have at least one of these is categorically frail. Furthermore, the JHACG uses 5 phenotypic criteria, which include: unintentional weight loss, exhaustion, low energy expenditure, low grip strength, and/or slow walking speed. This scale encompasses decline across multiple physiological systems and was developed to clinically identify those with increased vulnerability to adverse health outcomes. MRFs were queried using appropriate ICD-10 coding of categories including malnutrition, obesity, dyslipidemia, smoking, alcohol, and hypertension. These were based on previous studies that validated their efficacy for predictive modeling.3,19,20 Routine discharges were defined as any discharge home, whereas nonroutine discharges encompassed those to places other than home, which may include short-term care facility, skilled nursing facility, etc.
Statistical Analysis
The statistical analysis was performed using RStudio (Version 1.3.959). 21 Differences between categorical variables were evaluated using chi-squared tests. Mann–Whitney U-testing was used to evaluate for statistically significant differences in continuous data. Logistic regression models were developed for postoperative complications using the “Epitools” package, and post hoc receiver operating characteristic (ROC) curves were generated. The area under the curve was calculated and DeLong’s test was used to assess statistical significance when comparing ROCs. All statistical tests were 2-sided with a significant P-value being defined as P < .05. All patients with multiple MRFs were excluded so that we compared patients with only single-variable MRFs.
Results
Demographics
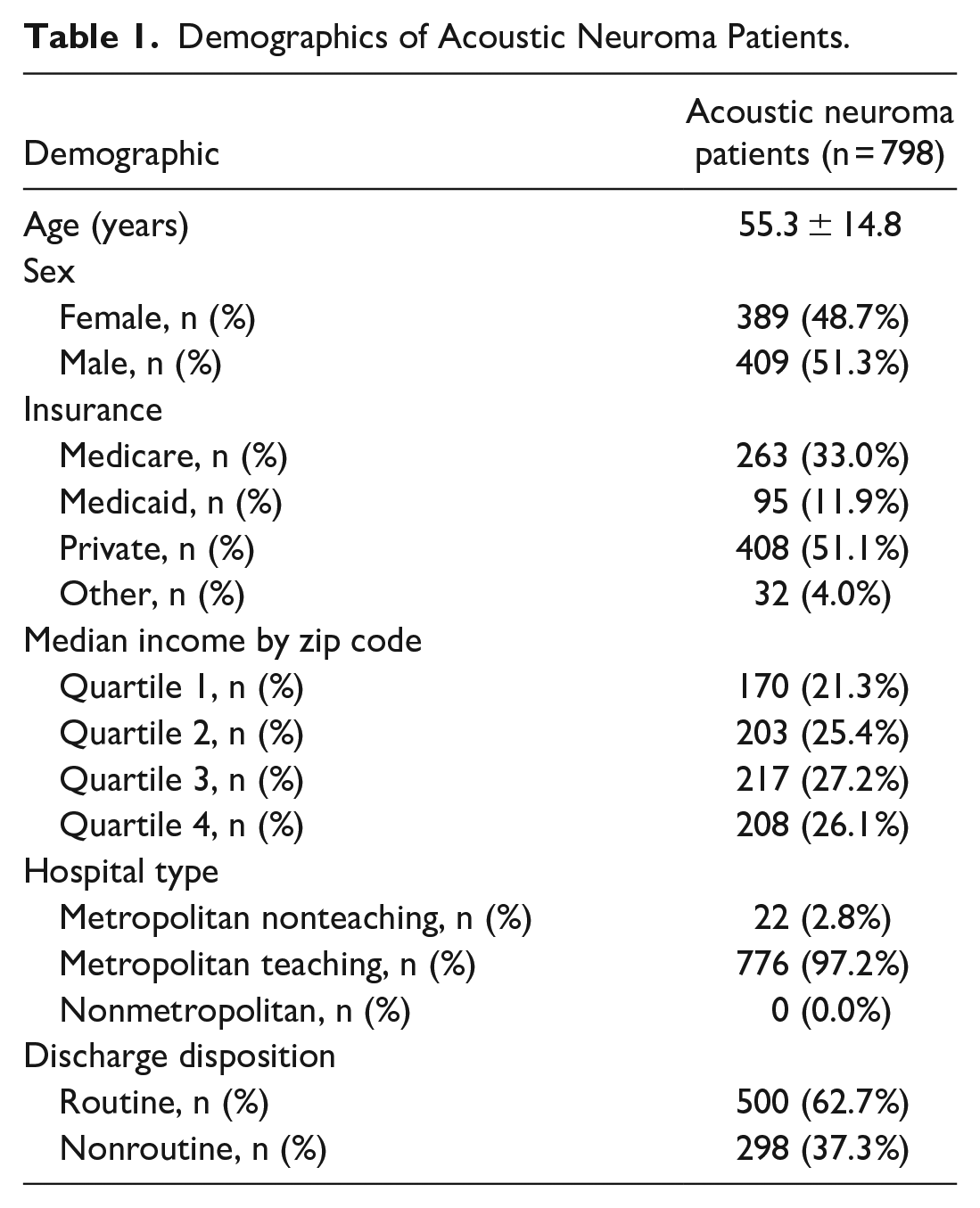
In the years of 2016 and 2017, there were 3951 patients admitted for an acoustic neuroma resection. A total of 798 patients were included in the analysis. The average age of the frail cohort was 55.3 ± 14.8, with 48.7% being female and 51.3% being male. Demographics including age, sex, insurance types, median income by zip code, and hospital type are demonstrated as Table 1. With regard to MRFs, 26 (3.3%) patients were malnourished, 35 (4.4%) were obese, 61 (7.6%) had dyslipidemia, 26 (3.3%) smoked tobacco, 0 (0.0%) had alcohol use disorder, and 123 (15.4%) had uncontrolled hypertension (Table 2).
Demographics of Acoustic Neuroma Patients.
Management and Complications in Acoustic Neuroma Patients.
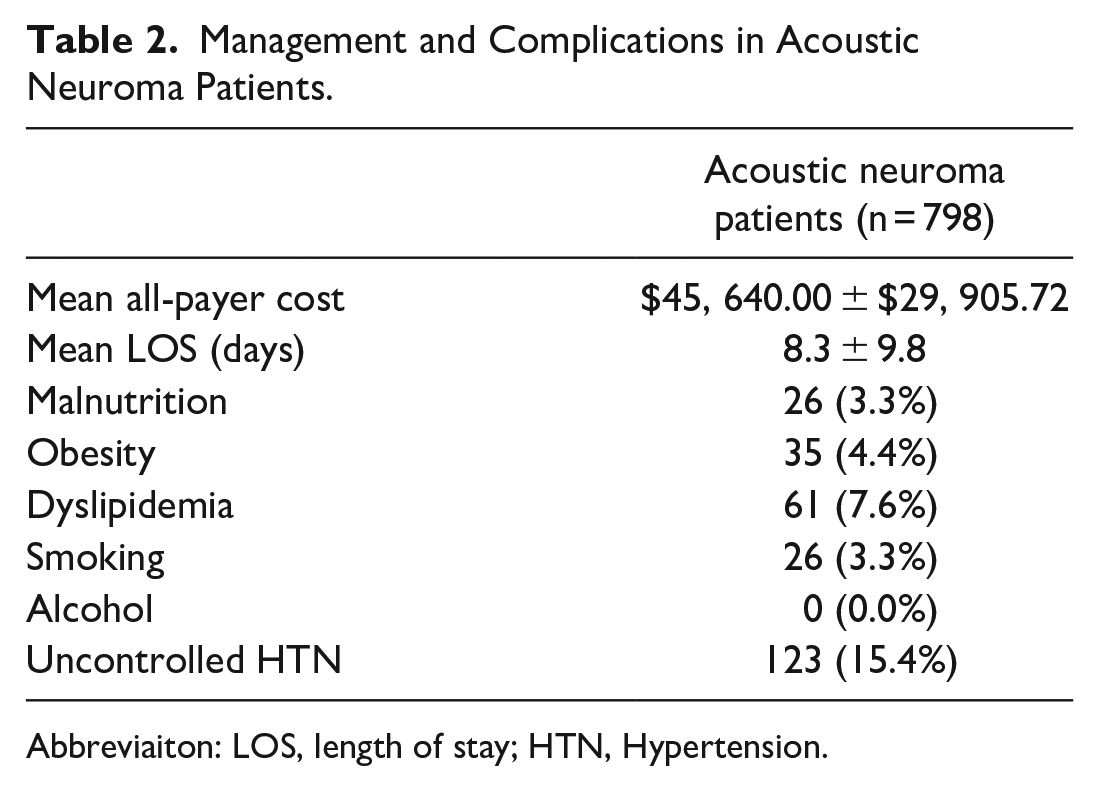
Abbreviaiton: LOS, length of stay; HTN, Hypertension.
Predictive Models and ROC Analysis
There were 2 logistical regression models developed, each using one of the above MRFs as the primary predictor. Models using alcohol use disorder were not included since 0 patients were reported in our study. These models were subsequently used to evaluate the occurrence of the postoperative complication of nonroutine discharge and readmission.
For nonroutine discharge, predictive models using malnutrition outperformed all other MRFs as well as those with no MRFs (P < .05) (Figure 1).
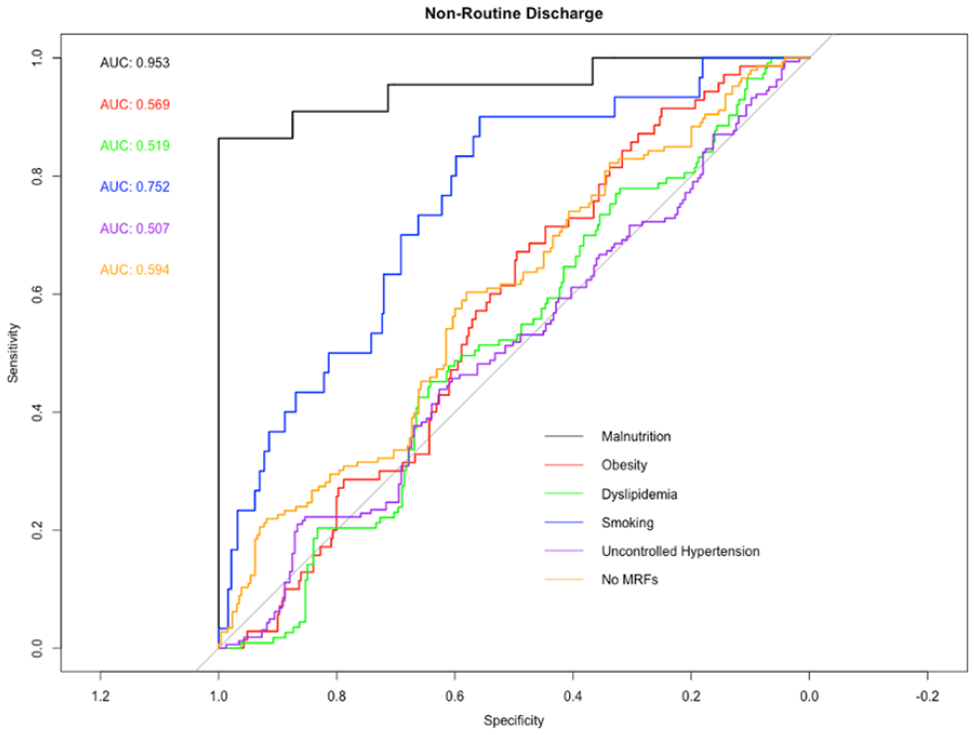
Receiver-operating characteristic (ROC) curve analysis for nonroutine discharge based on 5 modifiable risk factors (MRFs): malnutrition, obesity, dyslipidemia, smoking, and uncontrolled hypertension. The area underneath the ROC curve, the AUC, is labeled by color for each risk factor. A statistically significant increase in predictive power occurs when malnutrition is considered as opposed to obesity, dyslipidemia, smoking, uncontrolled hypertension, and those with no MRFs. This increase again occurs when smoking is considered as opposed to obesity, dyslipidemia, uncontrolled hypertension, or those with no MRFs, and when those with no MRFs are considered as opposed to uncontrolled hypertension (P < .05).
In the case of readmission, models using malnutrition outperformed those of obesity and smoking (P < .05). Again, in the case of readmission, an increase in predictive power is seen in models using dyslipidemia when compared to obesity, smoking, or uncontrolled hypertension. Lastly, models using no MRFs outperformed those of obesity, smoking, and uncontrolled hypertension (P < .05) (Figure 2).
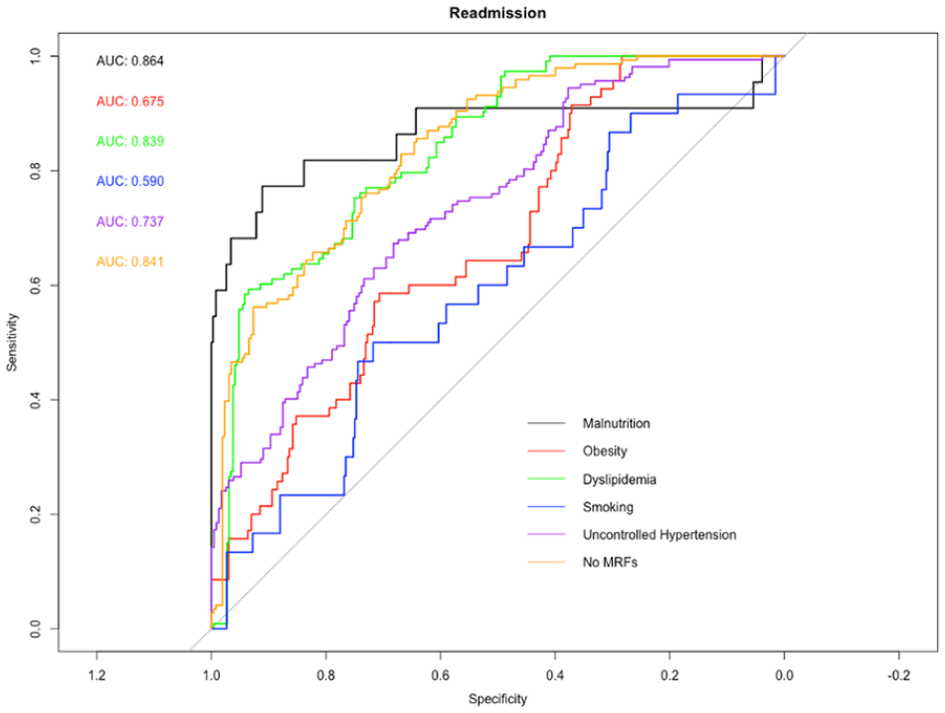
Receiver-operating characteristic (ROC) curve analysis for readmission rates based on 5 modifiable risk factors: malnutrition, obesity, dyslipidemia, smoking, and uncontrolled hypertension. The area underneath the ROC curve, the AUC, is labeled by color for each risk factor. A statistically significant increase in predictive power occurs when malnutrition is considered as opposed to obesity or smoking. This increase again occurs when dyslipidemia is considered as opposed to obesity, smoking, or uncontrolled hypertension and when those with no MRFs are considered as opposed to obesity, smoking, and uncontrolled hypertension (P < .05).
Postoperative Complication Rates
During the initial admission, the mean cost for patients receiving surgery for acoustic neuroma was $45,640.00 ± $29,905.72. Additionally, the mean LOS was 8.3 ± 9.8 days (Table 3). Furthermore, 298 (37.3%) patients had nonroutine discharges to places other than home (skilled nursing facilities, short-term hospitals, home healthcare, etc.). A total of 135 people were readmitted within 1 calendar year.
P-values Comparing all ROC Curve AUC Values.
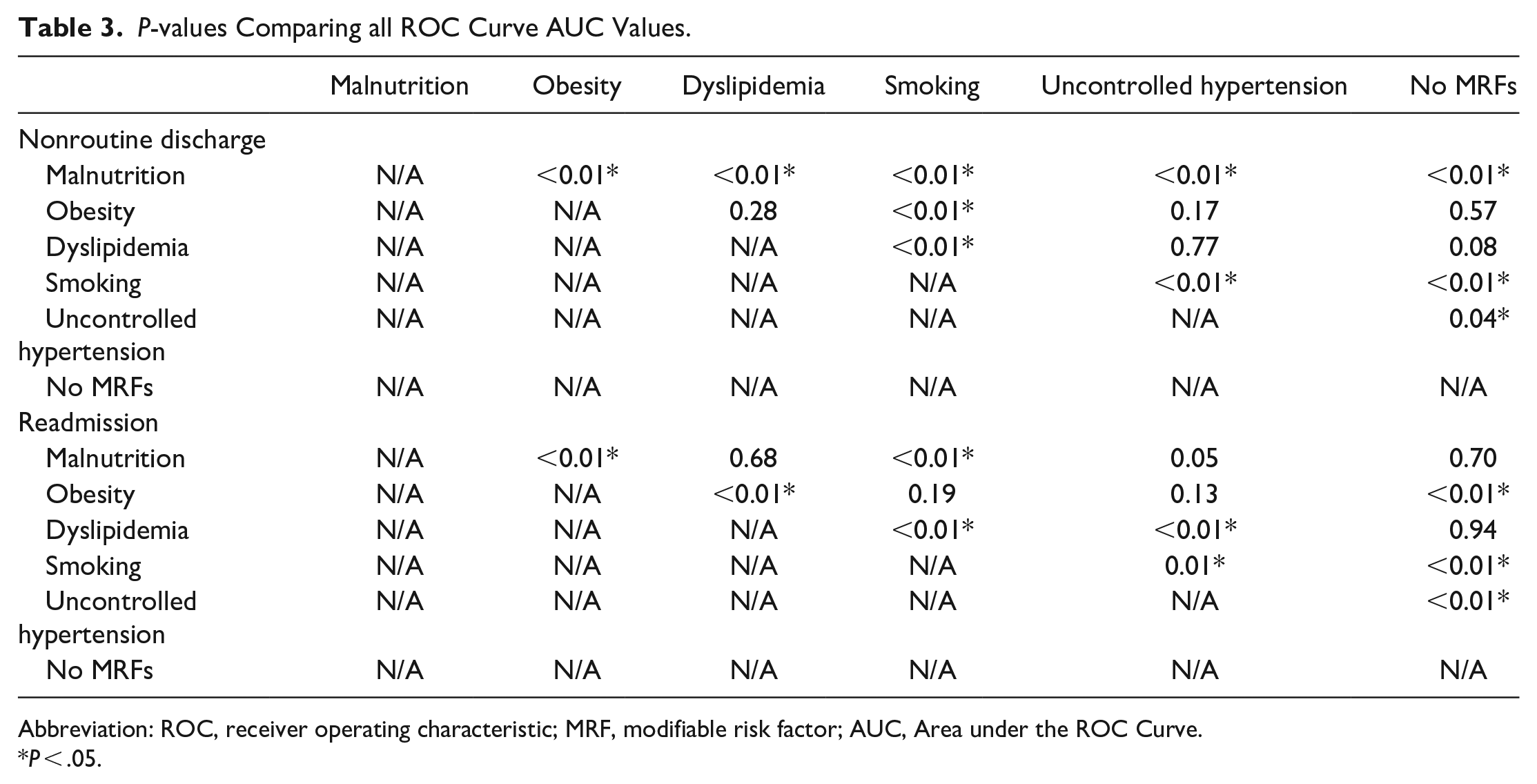
Abbreviation: ROC, receiver operating characteristic; MRF, modifiable risk factor; AUC, Area under the ROC Curve.
P < .05.
Discussion
Regarding nonroutine discharge, our findings revealed an increase in predictive power in models using malnutrition when compared to other MRFs and no MRFs. Regarding readmission, there was an increase in predictive power in models using malnutrition compared to models using obesity and smoking. Again, this increase is seen in models using dyslipidemia compared to those using obesity, smoking, or uncontrolled hypertension. Finally, an increase in predictive power was seen in models using no MRFs compared to obesity, smoking, and uncontrolled hypertension.
Understanding which MRFs in the frail population demonstrate an increase in predictive power of certain unfavorable outcomes is of great importance to the practicing physician, especially as it pertains to prioritizing which specific lifestyle factors should most urgently be addressed. There have been a number of studies that aimed to investigate the role of non-MRFs with postoperative outcomes in microscopic resection of acoustic neuroma, most commonly those NMRFs being age and clinical frailty.7,22-24 These studies found that clinical frailty was associated with increased risk of certain complications including postoperative hemorrhagic or ischemic stroke, infection, facial paralysis, urinary tract infection, hydrocephalus, dysphagia, as well as increased length of hospital stay and nonroutine discharge.7,22-24 While understanding how Non-Modifiable Risk Factors (NMRFs) can affect the perioperative course is important for clinicians, there is also an urgent need to investigate MRFs because of their unique ability to be amended through lifestyle intervention. This study aims to expands on previous studies, which used predictive modeling to demonstrate frail patient’s increased risk of readmission, nonroutine discharge, and postoperative morbidity, and further risk stratify this subpopulation according to MRFs. 7
The findings of our study are the first of its kind which aim to guide practitioners when tailoring patient management, especially in the case of vulnerable frail populations. Because of this tumor’s benign and slow growing nature, there is the flexibility to defer treatment either in the short term or indefinitely. The knowledge that there are certain risks associated with the perioperative course can be utilized by clinicians to mitigate certain lifestyle factors before opting for surgery. This may also be an area where radiosurgery may prove to be a superior treatment modality depending on its size and degree of hearing loss and presence of other symptoms such as dizziness. In older individuals, radiosurgery may be comparable in terms of tumor control, as demonstrated in certain types of malignancy. 25
While there is a paucity of literature regarding MRFs in acoustic neuroma resection, there have been studies demonstrating their effects across other specialties. While the investigated MRFs are not specific for acoustic neuroma, it is of great clinical value to understand how certain risk factors of interest influence disease states. In a study of those undergoing surgery for colorectal carcinoma, it was found that smoking, malnutrition, and alcohol consumption resulted in more frequent instances of severe complications and longer hospital stays. 26 Malnourishment is a topic that has been rather broadly investigated in the surgical world, and it is estimated that as many as 2 out of every 3 patients are malnourished preoperatively. 16 Malnutrition has been found to be an independent risk factor for complications, increased mortality, length of hospital stay, and costs.17,18 Our findings seem to corroborate this in the realm of nonroutine discharges. The National Surgical Quality Improvement Program relays that malnutrition is among the most easily targeted MRFs, while historically there has been less emphasis placed on perioperative nutrition intervention and counseling. 18
Investigating the effects of obesity is often done in the context of patients with metabolic syndrome, and thus it is often evaluated concurrently with hypertension and hyperlipidemia. A study done by Elsamadicy et al 27 found that obesity was an independent risk factor for unplanned 30-day readmissions after elective spine surgeries. Another study investigating MRFs in pituitary surgery found that malnutrition, obesity, and elevated lipid levels put patients at a higher risk of increased LOS, higher inpatient costs, and ultimately readmission. 28 The results of our study did not seem to uphold similar findings in obese patients in the case of nonroutine discharge or readmission, whereas those models evaluating dyslipidemia as a primary predictor showed a significant increase in AUC and thus, predictive ability compared to obesity, dyslipidemia, smoking, uncontrolled hypertension, and those with no MRFs.
Smoking is one MRF that has been studied in greater depth in various neurosurgical studies and has been found to have clear associations to perioperative complications and 90-day readmission.20,29-31 Additionally, smoking has been well studied across a number of surgical specialties, where it has shown repeated association with increased rates of wound infection, skin necrosis, and delayed healing.32-34 More relevant to neurosurgery, it was found that in patient’s undergoing craniotomy for tumor resection, cigarette smoking was associated intraoperative blood loss, postoperative complication risk, and lower 1-year survival.29,35 Our study did find that smoking was predictive in the case of nonroutine discharge when considered against obesity, dyslipidemia, uncontrolled hypertension, and those with no MRFs.
As more people are suffering from chronic disease states, there has been a shift in the medical narrative toward emphasizing preventative medicine. In doing so, many of these MRFs can be addressed and amended. Unfortunately, there is not a one-size-fits-all model for simultaneously addressing many of these issues, but there have been proven systems studied for individual risk factors. More specifically, there has been evidence that behavioral counseling and cessation medication interventions have been beneficial in addressing smoking cessation.36,37 Nutritional education, supplementation, and meal delivery programs providing better food access has been the adopted method for counteracting malnutrition.38,39 Focus on diet and exercise has been associated with better management and/or resolution of hypertension and dyslipidemia.40-42
Limitations
Limitations of this study include the lack of specific complications leading to the nonroutine discharge, readmission, and mortality, although this is an area of interest for future research. Additionally, the study is retrospective nature and thus only captures a small sample of time from the years of 2016 to 2017. These dates were specifically chosen because of the implementation of ICD-10 coding in 2015. The NRD is only to capture about 60% of the population, meaning that it may not be entirely representative of the US population. Additionally, because we are using a nationwide database and relying on ICD-10 diagnoses of these MRFs, it is likely that many cases are not documented and are therefore underreported in this patient sample. Unfortunately, due to the lack of granularity in ICD-10 coding, we are also unable to identify which method was utilized for resection of the acoustic neuroma. The database does not allow for granularity beyond the ICD-10 diagnoses listed, and thus we cannot investigate location, size, and nature of the tumor. Additionally, because this study was done using an inpatient national database, we were unable to investigate the effects of radiosurgery versus microsurgery, being as radiosurgery is routinely done on an outpatient basis. This may be an area for future research. We are also limited by the NRD in the MRFs available for investigation.
Conclusion
Overall, our findings suggest that non-MRFs, such as uncontrolled HTN, Body Mass Index (BMI), malnutrition, smoking, and dyslipidemia, can negatively impact a patient’s perioperative course leading to potentially increased incidence of nonroutine discharge, and readmission. Future research using prospective multicenter longitudinal data, which can investigate specific complications associated with these non-MRFs, may be further illuminating.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SS has conflicts of interest, including being: Consultant for the Mac Parkman Foundation for Adolescent Concussive Trauma. Stock/Equity holder in StrokeDx.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board (IRB) approval was unnecessary as this study utilized a publicly available de-identified dataset.
Informed Consent
No patient identifiers were collected.