
Abstract
Foreign bodies, particularly fish bones, in the hypopharynx and cervical esophagus are a common complaint. A swallowed foreign body can be embedded in the tonsil, the base of the tongue, the pyriform fossae, or any region of the upper esophagus. A 70-year-old woman presented with persistent left-sided pharyngeal pain with the sensation of a foreign body for 10 days. She felt a sudden sharp pain in her pharynx while eating a fish head 10 days before the presentation. On examination, an elderly woman was found in painful distress. Flexible fiberoptic laryngoscopy revealed a pool of saliva in the pyriform fossae and a diagnosis of a foreign body in the esophagus was suspected. She was planned for direct laryngoscopy, left (lateral/external) pharyngotomy, and removal of foreign bodies under fluoroscopic guidance of the C-arm. A metallic fish hook that hung over the greater left horn, buried in the neck muscles, was found during the surgery and was extracted. The patient did well postoperatively and was discharged from the clinic. Foreign bodies, particularly fish bones, in the hypopharynx and cervical esophagus are a common complaint, particularly in the African setting.
Introduction
Ingestion of a foreign body is a common problem in otolaryngological practice. 1 In adult subjects, this is often accidental and commonly ingested foreign bodies are food items. 2 The symptoms are variable and depend on the size, location, and time of presentation. Some common symptoms may include drooling, emesis, dysphagia, chest pain, neck pain, or pharyngeal pain, and cough. 3 Early presentation and quick intervention are vital to prevent the serious morbidity that can occur as a result of such a condition, especially with a sharp foreign body. 4 One of the uncommon complications of ingested foreign bodies is the migration of the object and the penetration of contiguous structures, which can lead to serious morbidity and mortality. 1
Foreign bodies, particularly fish bones, in the hypopharynx and cervical esophagus are a common complaint. A swallowed foreign body can be embedded in the tonsil, the base of the tongue, the pyriform fossae, or any region of the upper esophagus. More than 80% of foreign bodies ingested that need removal are located in the esophagus, 76% of which are lodged within the upper esophagus, at a level that corresponds to the thoracic inlet. 5 There have been documented reports of fish bone and meat and meal boluses in the esophagus. 6 However, accidental ingestion of a foreign body hidden in a food item is rare. The fish hook is metallic and sharp; hence, the attendant risk of impaction, extraluminal migration, and fatal complications.
From a 9-year retrospective study conducted in our hospital (the University of Ilorin Teaching Hospital), the prevalence of foreign body ingestion was 57.6%, with dentures being the most common (30.3%). With the advent of more sophisticated imaging methods and the advancement of upper aerodigestive endoscopic procedures, most of these foreign bodies can be easily removed. 7 However, in rare cases, sharp/impacted foreign bodies can perforate the upper digestive tract and migrate into the soft tissues of the neck. If this condition is not anticipated, it could lead to serious complications with high-risk morbidity and mortality. 8
We present a rare case of a 70-year-old woman who had accidentally ingested a fishing hook while eating fish and presented to the A&E unit of the hospital with a 10-day duration of persistent left-sided throat pain and foreign body sensation on the same side of the throat. The fish hook migrated into the neck without serious morbidity and was removed by an external approach, with satisfactory result.
Case Report
A 70-year-old woman presented with persistent left-sided pain in her pharynx and the sensation of a foreign body for 10 days. She felt a sudden sharp pain in her pharynx while eating a fish head 10 days before the presentation. The pain became throbbing and persisted. There was an associated sensation of a foreign body in the throat, dysphagia, and odynophagia. There were no hemoptysis, choking spells, neck pain, neck swelling, or fever, but subsequently developed left otalgia. She first presented at a peripheral health center where an X-ray of the soft tissue neck was done and was referred to our facility due to the finding of a suspected fish hook in the pharynx.
On examination, an elderly woman was found in painful distress. She was not pale, anicteric, afebrile (36.8), or dehydrated. Her vital signs at the time of presentation were as follows: heart rate: 74 bpm, blood pressure: 130/70 mmHg, SPO2: 98% in room air, and respiration rate: 18/pm. Fiberoptic laryngoscopy revealed a pool of saliva in the pyriform fossae and a diagnosis of a suspected foreign body was made in the esophagus.
A rigid esophagoscopy was done but the localization and removal of the foreign body were unsuccessful. A yellowish tough thread with purulent discharge was seen on the left side of the hypopharynx, at a level corresponding to 15 cm on the rigid esophagoscope (from the upper incisor). Subsequently, a CT scan + 3D reconstruction was performed which revealed a fish hook in the left parapharyngeal space, hooked around the left greater horn of the hyoid bone (Figure 1a). This patient found it difficult to believe. Ten days later, a repeat surgery was performed which included direct laryngoscopy, left (lateral/external) pharyngotomy, and foreign body removal under C-arm fluoroscopic guidance (Figure 1b).
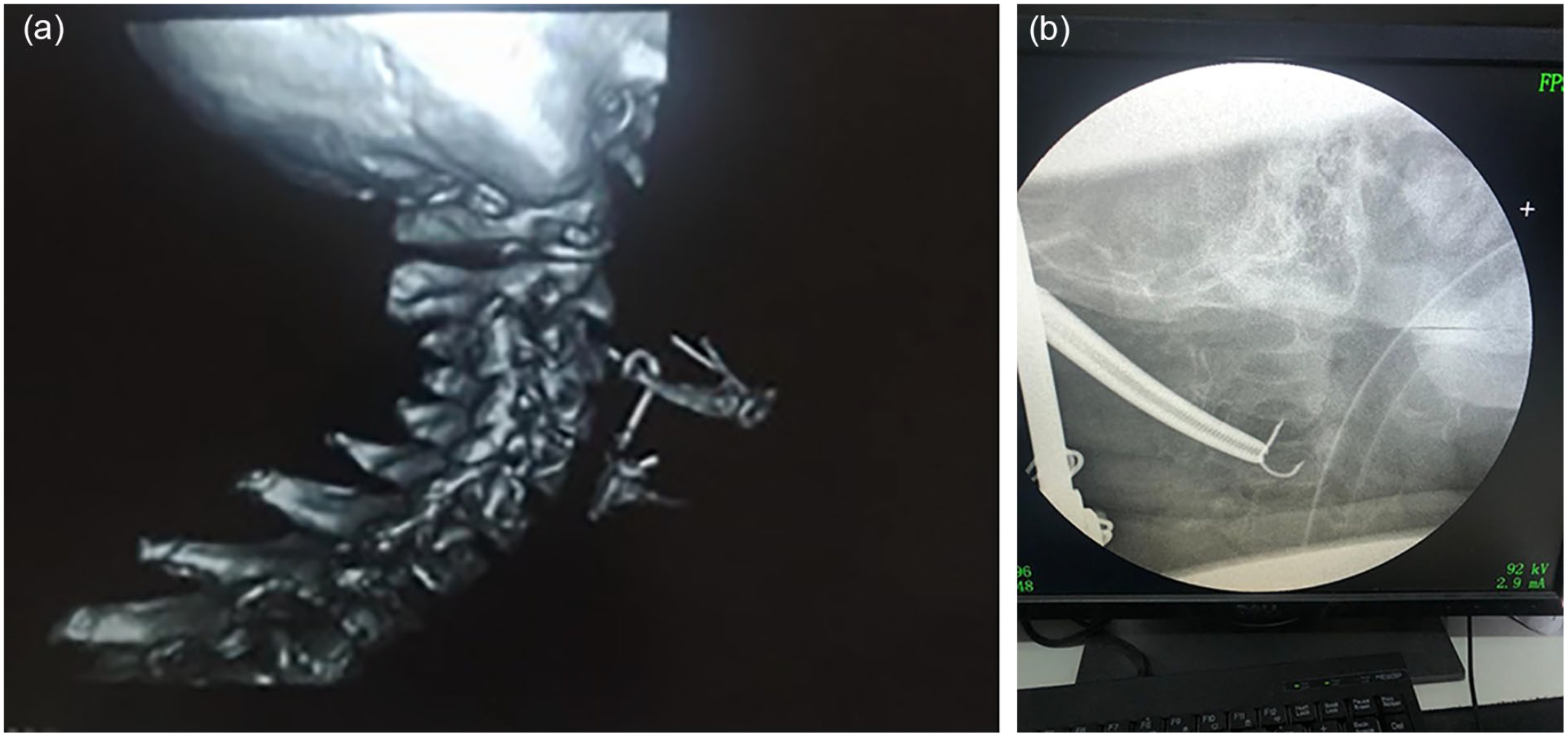
(a) 3D CT reconstructed image showing a C-arm fishing hook hung on a hyoid bone. (b) Localization of foreign body (fishing hook) under fluoroscope guidance.
Intraoperative findings included the following: (1) Hyperemic, edematous lateral wall of the left pyriform sinus with a yellowish thread protruding from its upper part on laryngoscopy. (2) A metallic fish hook hanging over the left greater horn, buried in the neck muscles on the left external lateral pharyngotomy (Figure 2a). After extraction of the fish hook (Figure 2b), the wound was closed in layers. The postoperative condition was satisfactory. The patient recovered well on the ward and was discharged to the clinic on the seventh postoperative day, with satisfactory follow-up result.
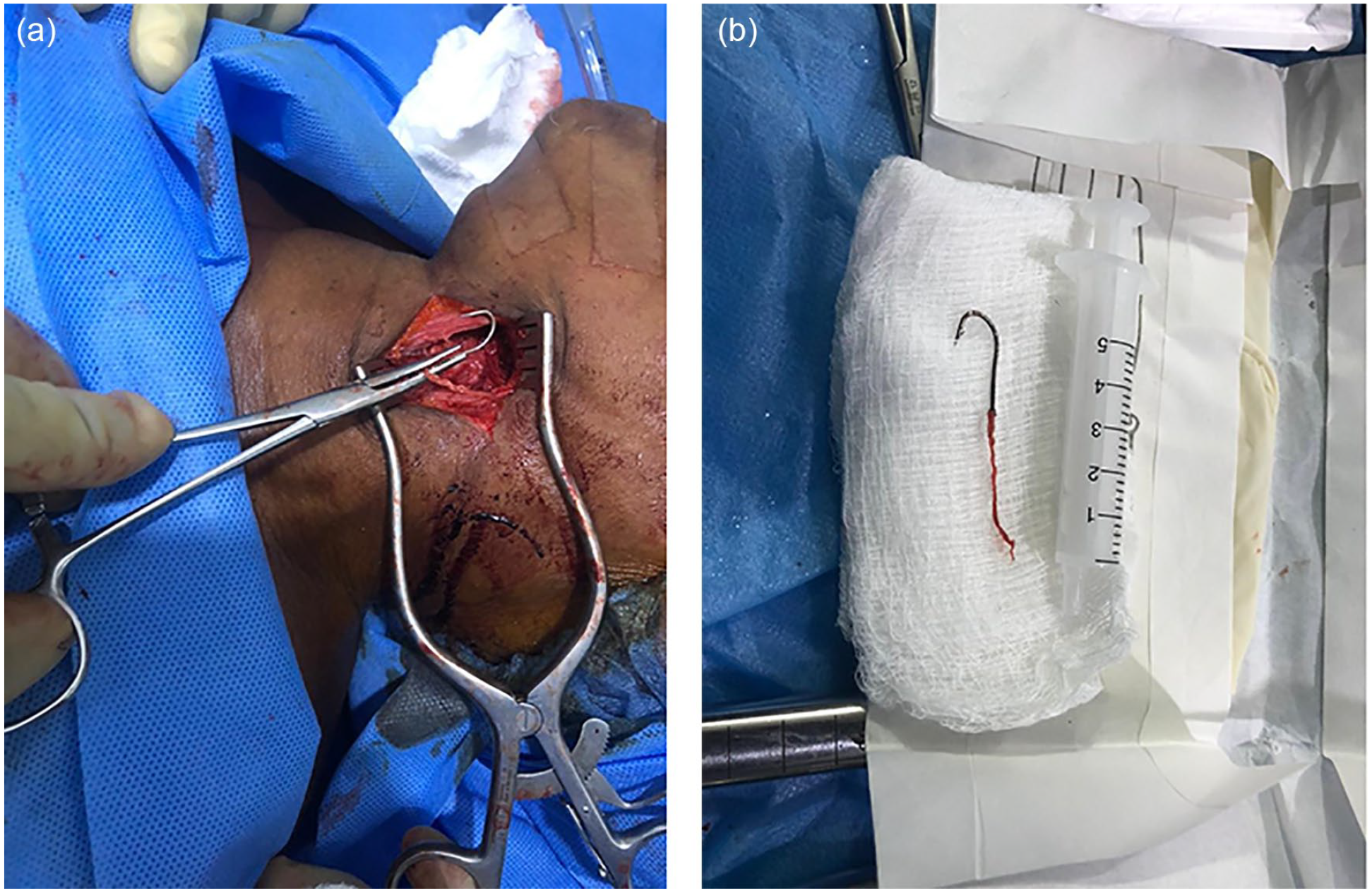
(a) Exposing the foreign body (fishing hook) using a self-retaining retractor on the neck. (b) A fish hook extracted.
Discussion
Foreign bodies, particularly fish bones, in the hypopharynx and cervical esophagus are a common complaint, particularly in the African setting where unfilled fish consumption is taken as a delicacy in pepper soup and several other traditional soups and stews. The ability to navigate through the mesh of bones and sift them out with the aid of the tongue is assumed to be an art and some claim makes the meal more delicious. However, this was not successful in the index case.
A series reported a higher incidence of foreign bodies perforating the upper aerodigestive tract in women (7 out of 11) and more on the left (7 out of 11) with ages ranging from 23 to 75 years. 1 The patient presented here is a 70-year-old woman who had a foreign body perforation on the left.
The suspicion of foreign body perforation on upper aerodigestive endoscopy is heightened by the findings of localized hyperemia and edema, ulceration, or laceration. Depending on its nature, a foreign body lodged in the esophageal or pharyngeal wall could be dislodged and removed endoscopically using a reusable rat tooth, alligator jaw, and rotatable grasping forceps. 9 However, this was not possible in the index case because as a sharp object it perforated the pharyngeal wall and got hooked to the hyoid bone. Therefore, pulling the attached thread at endoscopy would have caused more harm than good if successful, hence the decision to adopt an external approach.
In the case presented here, what gave away the location of the foreign body is the string attached to it which that juts into the pharyngeal lumen. However, the esophagus can be a temple of surprise when there is a sharp foreign body impaction that may be far away from what is believed to be. In the presence of negative endoscopic findings, radiography is an important tool for locating a perforated foreign body in the neck but can be misleading in cases with cartilage calcification of the upper airway. A neck computed tomographic scan is considered the investigation of choice in such cases 1 as it is highly essential for the prompt diagnosis and removal of a foreign body perforation. 1 However, it is important to note that a foreign body seen in the upper aerodigestive tract on a CT scan may not be visible on endoscopy as in the index case. 1 On some occasions, an intraoperatively C-arm fluoroscopy machine may be employed for an on-time localization, which facilitates retrieval, as done in this case.
Conclusion
This report suggests that a sharp foreign body impact in the pharynx during a fish meal may not necessarily be a fish bone, and its migration out of the aerodigestive tract can present diagnostic and therapeutic challenges for ENT and/or cardiothoracic surgeons. In the same breath, the traditional fishing method that involves the use of fish hooks should be discouraged, or the practitioner educated/enlightened to always ensure the hook is retrieved before selling or eating the fish caught with it.
Footnotes
Data Availability Statement
The data related to the manuscript are available with the corresponding author and will be provided upon the request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/Consent Statement
Written informed consent was obtained from the patient for the publication of this case report.