
Abstract
Ramsay Hunt syndrome is a facial nerve palsy that arises from herpes zoster infection. In rare cases, postherpetic neuralgia is a complication following Ramsay Hunt syndrome. Pain management to address postherpetic neuralgia includes facial nerve blocks, medications such as gabapentin, carbamazepine and botulinum toxin injections, and pulsed radiofrequency. Despite the reported benefits for patients with glossopharyngeal nerve pain, neurectomy as a treatment has rarely been described. A 45-year-old patient visited our ENT clinic for chronic right-sided facial, ear, and jaw pain that persisted for 9 years following the development of Ramsay Hunt syndrome. She trialed multiple medications including gabapentin, carbamazepine, and botulinum toxin injections with minimal relief to her symptoms. The patient underwent a diagnostic myringotomy with topical application of lidocaine to the tympanic nerve. This resulted in temporary relief of her pain until the effects of the lidocaine subsided. The patient was subsequently offered lysis of the right tympanic nerve for more definitive management. The patient experienced significant pain reduction after the right tympanic neurectomy procedure. Chronic postherpetic neuralgia following Ramsay Hunt syndrome can cause significant impairment in a patient’s quality of life. For patients with ear pain refractory to conservative management, a tympanic neurectomy can be considered.
Introduction
Ramsay Hunt syndrome is a facial nerve palsy that arises as a late complication of herpes zoster infection. 1 Primary infection by varicella zoster virus manifests as fever with a diffuse vesicular rash. 2 Following primary infection, the varicella zoster virus remains dormant in the trigeminal and dorsal root sensory ganglia of the body. 3 Reactivation of the dormant virus causes a herpes zoster reaction consisting of pain along the distribution of the affected nerve. 2 When the affected nerve of reactivation is along the geniculate ganglion of the facial nerve (CN VII), the collection of symptoms is termed Ramsay Hunt syndrome. 2
The constellation of symptoms that comprise Ramsay Hunt syndrome was first introduced in 1907 by Dr. James Ramsay Hunt, a World War I physician and neurologist. 1 He used the term “Ramsay Hunt syndrome” to describe the unique clinical presentation of facial paralysis and a vesicular rash. His analysis of this syndrome led to greater understanding of the general somatic sensory function of the facial nerve as well as identification of the geniculate zone of the ear. 1
Common complaints in patients affected by Ramsay Hunt syndrome include facial paralysis, vesicular rash, otalgia, and severe pain. 2 In rare cases, postherpetic neuralgia has been described as a complication following Ramsay Hunt syndrome. 4 Patients affected by postherpetic neuralgia report severe life-altering changes attributable to their pain. 5 Despite the reported benefits for patients with refractory cases of facial and glossopharyngeal nerve pain due to other causes, neurectomy as a treatment option for postherpetic neuralgia in Ramsay Hunt patients has rarely been reported. 6
In this case report, a patient who was diagnosed with Ramsay Hunt syndrome continued to experience right-sided ear pain which radiated from the temporal area to the jaw and neck region—despite medical treatment with gabapentin, carbamazepine, amitriptyline, and botulinum toxin injections. Here, we present the beneficial treatment for persistent pain after Ramsay Hunt syndrome by performing a right tympanic neurectomy.
Case Report
A 45-year-old immunocompetent female patient visited our ENT clinic for assessment of chronic right-sided facial and ear pain after a diagnosis of Ramsay Hunt syndrome. The patient complained of radiating pain that was sharp, burning, stabbing, and throbbing. She endorsed that the pain worsened with eating, talking, or performing any facial movements. The patient noted that the only temporary relief to her pain was while she was sleeping. This patient’s experience with postherpetic neuralgia had significantly interfered with her daily functioning and quality of life, prompting her to seek a more permanent solution.
Her history dates back approximately 10 years ago when she awoke to severe right-sided ear pain accompanied by right-sided visual changes and right-sided facial palsy. Her symptoms included blurry vision, diminished taste, facial asymmetry at rest and moderate right ptosis. On audiogram, she had normal hearing bilaterally and 100% discrimination. An MRI without contrast found no evidence of a mass or abnormal enhancement. A T2 weighted scan demonstrated normal appearance of the cisternal and Meckel’s cave portion of the trigeminal nerve and normal appearance of the seventh/eighth nerve complex.
The patient was subsequently diagnosed with Ramsay Hunt syndrome due to herpes zoster and prescribed oral valacyclovir and prednisone. The patient reported that she was unable to complete the full antiviral treatment due to negative side effects.
The patient had tried numerous medications to alleviate the persistent right-sided facial and ear pain. She visited the Neurology clinic due to severe right-sided facial weakness, tightness around her right eye, and burning pain anterior to the tragus. She reported episodes of fasciculations around the right nasalis muscle. Neurological examination revealed no activation of her right frontalis or zygomaticus muscles, partial activation of the right platysma, and no obvious hearing impairments. She had hyperpathia over the malar region of the right side of her face and synkinetic contractions of the right side of her face with prominent narrowing of the palpebral fissure when she attempted to smile.
Given these findings, the Neurology team began a trial of 10 units of botulinum toxin injections every 3 months.
The patient reported improvement in muscle twitching; however, she continued to endorse persistent right-sided facial and ear pain. The pain was localized anterior to the tragus and extended into the right submalar region. At times, the severe pain was accompanied by nausea and vomiting. Botulinum toxin injections were administered again. Trials of gabapentin and carbamazepine were unsuccessful due to medication allergies of hives and difficulty breathing, respectively. A trial of amitriptyline interfered with the patient’s citalopram. Due to insurance coverage issues, the patient did not receive any subsequent botulinum toxin injections.
During her visit at the ENT clinic, the patient complained of deep lancinating right ear pain. The pain level was persistently 8–9/10 on average but fluctuated in intensity with flares being a 10/10 pain level. She reported that aggravating factors include chewing, talking, and lying on the right side of her face. A diagnostic myringotomy with topical application of lidocaine to the right tympanic nerve was performed to predict the effectiveness of tympanic nerve lysis to help with her pain.
The right tympanic membrane was anesthetized using topical anesthesia. An inferior myringotomy was made and Jacobsen’s nerve (tympanic nerve) was visualized on the promontory. A small piece of compressed gelfoam soaked in 2% lidocaine was inserted through the myringotomy and placed over Jacobsen’s nerve.
The myringotomy procedure provided significant temporary pain reduction. At follow-up 3 weeks later, the decision was made to perform a right tympanic nerve lysis. The patient subsequently underwent right exploratory tympanotomy with lysis of Jacobson’s nerve under general anesthesia.
Jacobson’s nerve originates from the inferior ganglion of glossopharyngeal nerve. 7 The nerve then courses through the tympanic canaliculus into the middle ear. On the promontory of the tympanic cavity, Jacobson’s nerve joins sympathetic nerve fibers to form the tympanic plexus supplying sensation to the middle ear, eustachian tube, mastoid, and parotid gland (Figure 1). 7
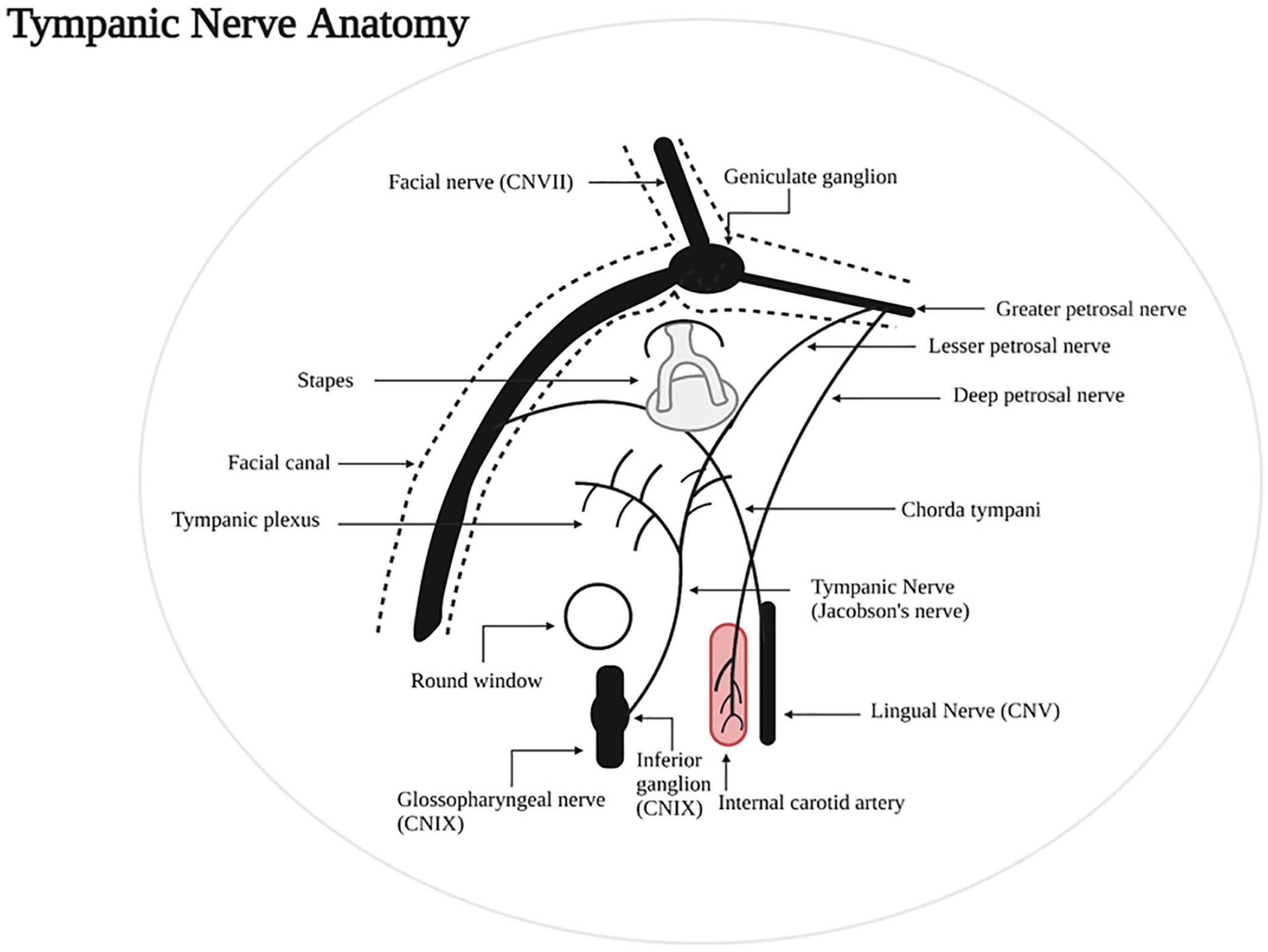
Anatomical landmarks of the tympanic nerve and surrounding structures.
At the 1-week follow-up appointment, the patient reported improvement in ear pain. At the 6-week follow-up appointment, the patient reported a marked reduction of pain. The tympanic membrane appeared intact, and her hearing was normal bilaterally. The patient reported no complications after the procedure at the 6-week follow-up.
Discussion
Ramsay Hunt syndrome is an undesirable consequence of varicella zoster virus reactivation in the cranial nerves or dorsal root ganglia distribution. 2 Reactivation can occur anywhere along the dermatomes of the body, but if facial paralysis is involved it is termed Ramsay Hunt syndrome. 8 Compared to Bell’s Palsy, a more common facial paralysis without a rash, Ramsay Hunt patients are less likely to recover completely. 1 Patients often experience pain in the ipsilateral ear with facial paralysis and vesicles appearing within 2 to 3 days due to reactivation along the facial nerve. 2 Due to the close proximity of the facial nerve to the vestibulocochlear nerve, patients may also experience symptoms of tinnitus and vertigo. 2 Furthermore, Ramsay Hunt syndrome has often been characterized as a polycranial neuronitis due to involvement of other cranial nerves. 9 In order of frequency, the cranial nerves commonly involved in Ramsay Hunt syndrome include CN VIII, IX, V, and VI. 10 Although reactivation is more common among patients experiencing stress and/or immunocompromised states, it can occur in immunocompetent patients as well. 2
Ramsay Hunt syndrome is typically self-resolving; however, the extent of recovery can vary between patients. 2 The most significant prognostic indicator of Ramsay Hunt syndrome is the severity of the initial facial paralysis. 2 One of the most debilitating sequelae of Ramsay Hunt syndrome is postherpetic neuralgia. Postherpetic neuralgia is defined as persistent pain 3 months after the onset of the herpes zoster virus. 11 The patient in the present case experienced pain that persisted for over 9 years in duration. Thus, postherpetic neuralgia following Ramsay Hunt syndrome is the most likely etiology of this patient’s pain.
Current literature supports the prevention of postherpetic neuralgia following Ramsay Hunt syndrome through early diagnosis and treatment of herpes zoster with antiviral agents. 11 Guidelines for Ramsay Hunt syndrome currently recommend treatment initiation within 72 hours of clinical symptoms with valacyclovir and prednisone. In severe cases (eg, vertigo, tinnitus, or hearing loss), IV therapy can be initiated, and the patient can then be transitioned to an oral antiviral agent when the lesions begin to crust. 12 Primary prevention of herpes zoster can be achieved with administration of the recombinant zoster vaccination for all immunocompetent patients over the age of 50. 13
In the rare cases of postherpetic neuralgia, pain management is achieved through medical management. Initial therapies include gabapentin and tricyclic antidepressants following dose escalation until achievement of therapeutic benefit. 14 Alternative therapies include anti-seizure medications, serotonin-norepinephrine reuptake inhibitors and opioids. 14 For patients refractory to the aforementioned treatments, as was the case with the current patient, botulinum toxin injections and neuromodulation techniques can be used. 15
Prior studies have outlined various surgical pain management techniques to address refractory postherpetic neuralgia in Ramsay Hunt patients including facial and great auricular nerve blocks, pulsed radiofrequency, nerve reconstruction, and tympanic neurectomy.4,6,16,17 One such study investigated the efficacy of selective nerve root block for treating postherpetic neuralgia. 16 Researchers demonstrated that early use of selective nerve root block appeared to decrease the incidence and shorten the duration of postherpetic neuralgia in patients treated during the acute phase of herpes zoster. 16 In the present patient, this approach would not have been feasible given the delayed presentation in clinic.
In a case report by Kim et al, 4 researchers treated chronic otalgia due to Ramsay Hunt syndrome using ultrasound-guided pulsed radiofrequency to the greater auricular nerve. This treatment mechanism includes blockage of the temporal nerve signals and enhancement of the descending inhibitory pathway, yielding a reduction in pain intensity by 50%. 4 Due to the novelty of this approach, logistical obstacles prevented the clinician in the present case from utilizing pulsed radiofrequency.
A retrospective study described a minimally invasive surgical nerve reconstruction technique to treat severe periorbital neuropathic pain. 17 A small sample size of patients underwent transection of the affected nerve (supraorbital, infratrochlear, infraorbital zygomaticotemporal or zygomaticofacial) with customized reconstruction and they all reported improvement in pain. 17 In the present case, nerve reconstruction of the lysed tympanic nerve was not deemed medically necessary to achieve therapeutic benefit.
Tympanic neurectomy has been described to treat severe otalgia from other causes such as prior middle ear surgery, following deep space infections with surgical drainage and post sudden sensorineural hearing loss. 6 Among the 12 patients undergoing the procedure, researchers found a complete resolution of otalgia in 69.2% of them. 6 However, tympanic nerve neurectomy has not been widely reported to treat postherpetic neuralgia following Ramsay Hunt syndrome.
Tympanic nerve neurectomy is a safe procedure which may provide benefit for refractory cases of ear pain from postherpetic neuralgia following Ramsay Hunt syndrome. The mechanism of neurectomy includes surgical entry and lysis of the affected nerve. Lysing the tympanic nerve terminates the sympathetic fiber conduction of the tympanic plexus and denervates the affected region. In the current literature, there is a paucity of research outlining the therapeutic benefit of neurectomy in refractory cases of postherpetic neuralgia. The proposed interventions could provide tremendous relief for patients suffering from postherpetic neuralgia.
Persistent postherpetic neuralgia after Ramsay Hunt syndrome can be refractory to medical management. For patients with ear pain, tympanic neurectomy can be a therapeutic option.
Footnotes
Author Contributions
Case report conception: Mirabelle Sajisevi, William Brundage
Drafting of case report: Ashwini Sarathy, Mirabelle Sajisevi, William Brundage
Critical revision of case report: Ashwini Sarathy, Mirabelle Sajisevi, William Brundage, Clemens An
Data Availability Statement
The data used to support the findings of the case report are included within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.