
Abstract
Invasive pituitary adenomas can infiltrate the dura mater, sphenoid sinus, or cranial bone. Endoscopic transsphenoidal sinus surgery is considered the standard of care; however, several potential complications must be noted. These complications can include cerebrospinal fluid leaks, infection, bleeding, optic nerve damage, and endocrinological complications such as diabetes insipidus. We present a case of a 69-year-old female with multiple recurrent invasive pituitary adenomas who has previously undergone 5 transsphenoidal procedures. Intraoperatively, the patient suffered from a left-sided carotid artery injury that was repaired with a muscle graft. Management of carotid artery injury during transsphenoidal surgery is optimized in a step-by-step approach which includes early recognition of the injury, briefing the surgical team, immediate control using compression, use of additional tissue graft for wound repair, and postoperative care. Through the use of the approach mentioned above, we were able to control the complication successfully.
Keywords
Introduction
Invasive pituitary adenomas occur when a slow-growing tumor within the stella turcica begins to grow rapidly and infiltrates the dura mater, sphenoid sinus, or cranial bone or metastasizes to other areas. Some potential complications during endoscopic transsphenoidal surgery can include cerebrospinal fluid (CSF) leaks, infection, bleeding, optic nerve damage, and endocrinological complications such as diabetes insipidus. 1
Transsphenoidal sinus surgery (TSS) followed by radiotherapy, in the case of remnant or recurrence, remains the standard of care for the treatment of invasive pituitary adenoma.2,3 Alternative treatment modalities include microsurgery and radiosurgery, which have shown great results regarding controlling further tumor growth; however, these modalities are associated with an increased risk of developing hypopituitarism, especially in patients previously treated with radiotherapy. 3 Furthermore, the use of temozolomide and rapamycin combined with octreotide has shown potential in slowing tumor growth since chimeric single-stranded template DNA (sst-DNA) analogs inhibit proliferation in vitro; however, additional clinical trials are needed to support the efficacy of these agents in the treatment of pituitary adenomas.
TSS poses risk for potential injury to the optic nerve, internal carotid arteries (ICA), pituitary gland, olfactory nerve, abducens nerve, oculomotor nerve, and the sphenoid sinus. Among these, ICA is a rare injury with an incidence of up to 0.1%. Still, it can be the most devastating, with high morbidity and mortality that can significantly impact prognosis for patients.1,4 While there are currently no validated guidelines on the management of ICA injuries, some studies have demonstrated that packing with a crushed muscle graft at the injury site is a safe and effective way to control bleeding and ensure longevity of the vessel. 5 We present a case of a multiple recurrent metastatic pituitary adenoma with intraoperative complication of ICA injury successfully managed with packing and a muscle graft.
Case Presentation
A 69-year-old female with a complex case of multiple recurrent metastatic pituitary adenomas with a history of panhypopituitarism and diabetes insipidus. She has had 5 prior transsphenoidal procedures, prior radiation therapy, and treatment with temozolomide who presented with diplopia and worsening of vision. Repeat imaging showed recurrent intrasellar and suprasellar tumor with cavernous sinus invasion and abutment of the left carotid artery, notable compression of the optic chiasm, and metastatic disease in the pons and cerebellum (Figure 1).
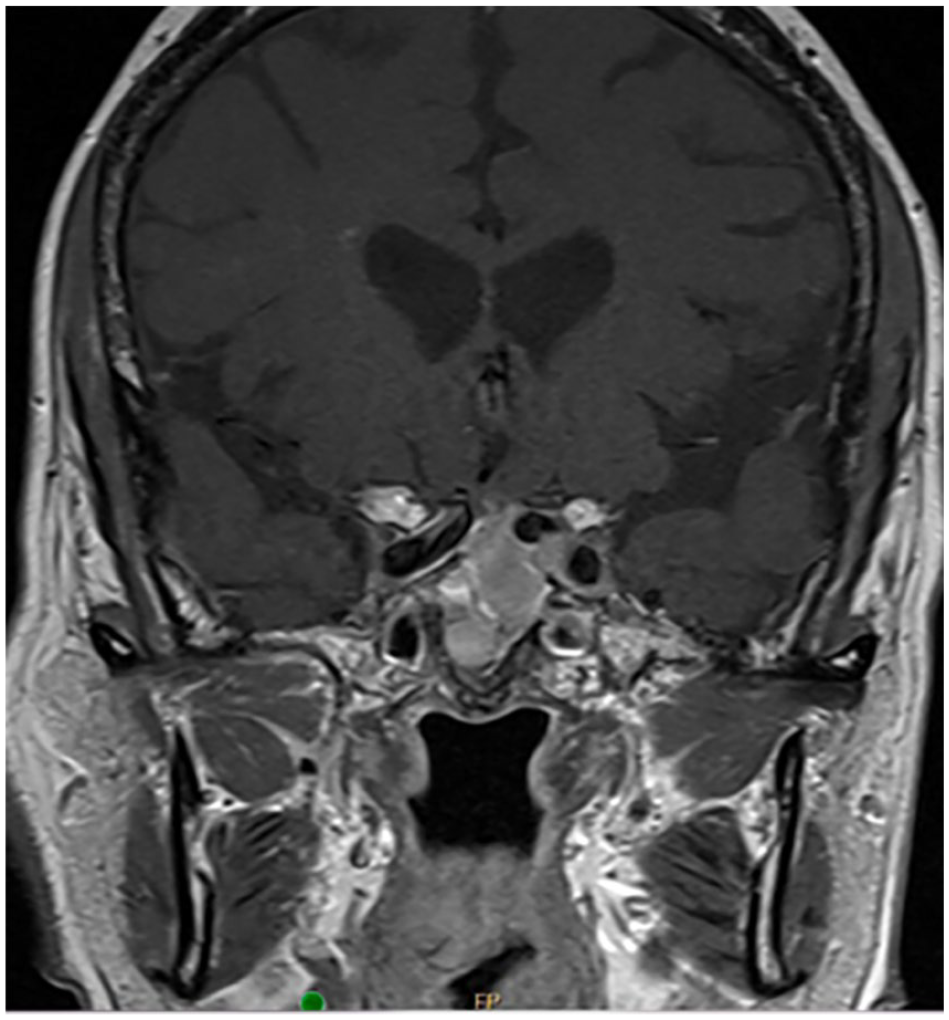
The intrasellar tumor has expanded substantially and extended into the suprasellar space, displacing the infundibulum to the right and impressing on the undersurface of the left side of the chiasm. There is also increased expansion into the retroclival space and the sphenoid sinus. Also has notable medialization of the left carotid.
After discussing options, a decision was made to proceed with debulking and decompression of the optic chiasm through a transsphenoidal approach. During the procedure, the left carotid artery was injured along the superior paracavernous segment when using a feather blade to take down scar tissue over the left cavernous sinus. Two suctions were used to clear the field and visualize the defect. The bleeding was immediately controlled via tamponade with gel foam and cottonoid pledgets (Figure 2). A fascia lata graft was harvested from the thigh and placed as an onlay, secured in place using surgical adhesive and dissolvable packing. A computed tomography (CT) angiogram was performed, which showed slight narrowing of the carotid vessel but no evidence of extravasation. The patient was neurologically intact initially. On post-op day 1, she became lethargic with left-sided weakness, and a repeat scan showed a new left medial thalamus stroke. Her deficits slowly recovered, and she was discharged to acute rehabilitation on day 6. On 4-month follow-up, her neurological deficits had recovered except for the left lower extremity, which was noted to be 4+/5.
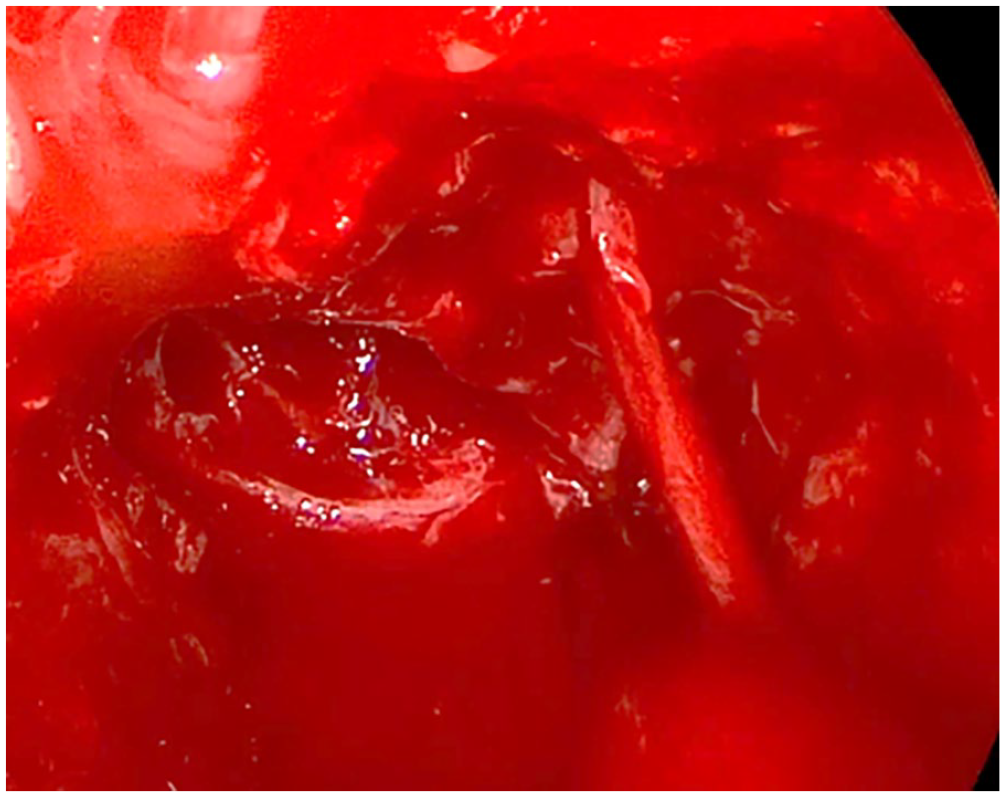
Active hemorrhage from a small left carotid injury encountered during surgery.
Discussion
TSS remains the standard of care for treating pituitary adenomas, despite risks for bleeding, CSF leak, carotid artery injury, and infection. Multiple studies have shown that endoscopic TSS has provided the greatest objective outcomes after surgery, with which some studies have shown a major complication rate of about 1%. Major complications would include CSF leak, hemorrhage, or temporary blindness. Although ICA artery injury is quite rare during TSS, with an incidence of 0.1%, preoperative measures are imperative to reduce the risk of carotid injury as much as possible. 6 Preoperative evaluations prior to TSS generally include a multidisciplinary disease management approach and preoperative imaging such as CT and magnetic resonance imaging, allowing the surgical team to gauge the risk of a carotid injury. A multidisciplinary team including surgeons and physicians from an array of specialties is recommended when treating pituitary adenomas for preoperative planning, planning treatment decision-making, and discussing all possible options.
The multidisciplinary tumor board will benefit the patient and the surgical team when undergoing decision-making, planning outcomes, and exploring all possible options regarding treatment.
Since carotid artery injury occurs at such a low incidence during endoscopic TSS, very few studies or meta-analyses provide enough statistical information to draw significant conclusions. A study published by Sharma et al 6 found that anatomic aberrations and wide dissection margins shown by preoperative imaging can increase the risk of carotid artery injury. However, 1 multicenter study on internal carotid artery injury showed that 82% of instances of carotid injury during transsphenoidal procedures involved patients who had anatomic aberrations of the internal carotid artery. 7 Aberrations include variations in the anatomy of the carotid artery itself or surrounding muscle and tissue, which may displace the ICA, making it more susceptible to injury during surgery. This could include incomplete bony coverings of the ICA, which can be seen during preoperative imaging. Other types of aberrations could include lesions and abnormalities which change the shape of the vessel wall, such as aneurysm, pseudoaneurysm, or carotid cavernous fistula. Previous sinus surgery, especially radiosurgery, can also pose a risk factor for ICA injury during TSS. Due to possible extensive scarring and osteonecrosis of the protective bone, there is an increase in the risk of damaging the ICA. 8
Intraoperative measures involve image guidance for endoscopic surgery. Endoscopic means for surgery can provide significant advantages. However, a drawback of endoscopy is that it can create a perceptual distortion by creating a 2-dimensional view in a 3-dimensional space. The use of image guidance during the surgery can provide 3-dimensional localization intraoperatively.
If an ICA injury is encountered during TSS, proper management would include visualizing the site of injury, fluid replacement, packing, and angiography. Since bleeding can significantly block the surgical view, it is imperative to be able to first visualize the site of injury by using suction. Using a large-gauge suction or multiple suctions has proven most useful during an ICA for clearing the field of vision. Once the field of view is cleared and the bleeding site is identified, hemostatic control can be done by packing the surrounding tissue with gauze, cottonoid pledgets, fibrin, gel foam, cellulose packing, or other materials. Packing must be executed cautiously, as excess packing can result in occlusion and stenosis of the ICA. 5 Long-term control of bleeding and repair of the defect can be done by harvesting muscle from an easily accessible region, crushing it, and placing it over the injury with tamponade. 5 Lastly, if the surgeon deems it appropriate, the injury can be managed by direct closure using endoscopic clips. 9 Once bleeding is under control, the next recommended course of action would be to send the patient to angiography to screen for the extent of damage.
Regarding postoperative care, the patient must be managed closely as rupture of pseudoaneurysm in the ICA may occur months or even years after the surgery, based on a study done by Valentine et al 10 on postoperative care for ICA injury. Lastly, minimizing the chances of ICA injury during TSS is based on prevention through imaging and preoperative management.
Conclusion
Although rare, carotid injury can be a devastating complication for the patient. Appropriate preoperative assessment is critical in risk stratifying for possible carotid injury. Rapid identification of the defect and tamponade is paramount to minimizing morbidity. Clear communication and an experienced multidisciplinary team are critical to success.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Dennis M. Tang is a consultant for Acclarent, Inc and 3-D Matrix.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was waived and not sought in our case study due to the lack of any identifying patient information.
Submission Statement
This article is original and has not been submitted elsewhere in part or in whole.