
Abstract
Keywords
Introduction
Benign recurrent vertigo (BRV), also known as benign paroxysmal positional vertigo (BPPV), is a balance disorder along with labyrinthitis and Meniere’s disease (MD).
It was first described by Slater, who diagnosed recurrent episodes of vertigo lasting from a few minutes to a few hours without neurological or any auditory symptoms as benign vertigo. 1 Since the duration and the symptoms are similar to MD and vestibular migraine, many scholars believe that BRV may be a subtype of MD or migraine. 2
Vestibular-evoked myogenic potentials (VEMPs) are short latency reflexes produced by the otolithic apparatus in response to acoustic or mechanical stimuli. 3 cVEMP is the short latency inhibitory potential recorded by the sternocleidomastoid muscle in response to acoustic or bone-conducted stimuli by the balloon. At the same time, oVEMP is the short latency excitatory potential recorded by the ellipsoidal bursa in response to acoustic or bone-conducted stimuli by the contralateral subocular oblique muscle. 4 Therefore, abnormal VEMPs would be caused if otolithic apparatus or conduction pathways are impacted. Previous studies have shown that the amplitude and frequency of VEMPs are best produced by acoustic stimulation at 500 Hz. In contrast, increasing studies demonstrated that the optimal amplitude frequency shifts from 500 to 1000 Hz in patients with MD.5,6 This may be due to the endolymphatic hydrops of patients with MD to a certain extent, causing the otolithic apparatus to resonate at this frequency. 7 Therefore, VEMP examination can detect otolithic involvement and predict underlying pathological manifestations of the vestibular disease to some extent.
For the sake of the absent studies on the clinical manifestation and etiological characteristics associated with BRV, this study would focus on exploring the clinical disease characteristics and etiological mechanisms of BRV through the clinical manifestation and VEMP tests in BRV patients.
Materials and Methods
Clinical Data
A total of 34 patients diagnosed with BRV by the Vertigo Specialist Clinic of the General Hospital of the People’s Liberation Army were enrolled, and 30 healthy volunteers matched in age and gender without ear or vestibular symptoms ever were recruited. All patients owned a detailed medical history of vertigo and underwent pure-tone audiometry, spontaneous and horizontal head-shaking nystagmus, video impulse testing, temperature sensation test, and VEMPs during vertigo episodes to rule out other vestibular disorders. The brain MRI is conducted to exclude the internal auditory canal and central nervous system disease. All patients were divided into 3 groups based on concomitant symptoms: Group A consisted of 17 patients (21 ears) diagnosed with BRV with ear symptoms, including tinnitus and stuffy ears; Group B included11 patients (22 ears) diagnosed with BRV and a history of migraine, who possessed a history of phonophobia, photophobia, or headache without cochlear symptoms; Group C included 7 patients (14 ears) with BRV without cochlear symptoms and a history of migraine. Group D consisted of 30 healthy volunteers (60 ears) who had never experienced cochlear symptoms, migraine symptoms, or vertigo. All participants conducted with VEMPs were explained before the trial, including the purpose, the method, and the presence of risks while signing the consent forms.
Inclusion Criteria
The inclusion criteria for BRV patients,
(1) At the age of 18 to 60;
(2) Match the BRV standard of Slater’s 1979 diagnostic criteria;
(3) Tremor has a latent and fatiguing character; and
(4) The Dix–Hallpike posture test or flip test can induce typical positional nystagmus and vertigo attacks on the affected side.
The inclusion criteria for healthy participants:
(1) At the age of 18 to 60 years and
(2) No brain-related and ear-related diseases.
Exclusion Criteria:
(1) Patients with low-frequency hearing loss and hearing loss with a clear cause;
(2) Vertigo caused solely by vestibular neuronitis, vertebrobasilar artery ischemia, and other disorders;
(3) Severe underlying illness, inability to complete postural tests and other investigations;
(4) Inability to communicate appropriately or cooperate in completing the test; and
(5) Incomplete clinical information
Clinical Methods
The Danish International Hearing Vestibular Myogenic Evoked Potential Analyzer (EPX5 type, International Hearing, Denmark) was used for recording the VEMPs of each participant. Stimulation frequencies were short pure tones in 500 Hz or 1000 Hz with a rise/fall time of 2 minutes, a plateau time of 1 minute, and an intensity of 100 dB nHL. The priority of ear testing and frequency were randomized in all participants.
The cVEMP was conducted by placing the patient in an upright sitting position with the ground electrode in the middle of the forehead. When cVEMP was conducted, the participants were requested to sit in an upright position. The recording electrode was applied on the outer edge of the upper one-third of the double sternocleidomastoid muscle, while the reference electrode was placed in the middle above the sternum. The ear of the subject side will hear the sound from the inserted air conduction earphone and turn the head to the other side vigorously during the test to maintain the tension of the sternocleidomastoid muscle on the recording side >49.9 μv. Finally, the waveform on the same side was recorded. The cVEMP amplitude is the peak amplitude between P13 and N23.
When the oVEMP was conducted, the grounding electrode was placed in the middle of the forehead, and the recording electrode was placed directly below the bilateral pupils at a distance of 1 cm from the lower eyelids. In contrast, the reference electrode was placed in the middle of the lower jaw with the participants in an upright position. The participant was requested to keep the head facing forward during the test and look at the target point 30° directly above during the recording, leading to the tensest state of the inferior oblique muscle. The waveform on the same side was finally recorded. The oVEMP amplitude is the peak amplitude between P15 and N10.
The frequency amplitude ratio (FAR) was generated by dividing the interpeak amplitude of the VEMPs generated by the harsh pure tone at 1000 Hz by the interpeak amplitude of the VEMPs induced by the harsh pure tone at 500 Hz in the same ear (FAR = 1000/500 Hz FPA, the frequency peak amplitude). To calculate the FAR in the absence of induced VEMPs, the amplitude ratio was artificially set as 1 μv. The actual zero value was applied in the calculation of the mean amplitude.
Statistical Processing
Continuous variables were expressed as mean ± standard deviation (SD) and median. Statistical analyses were performed using the SPSS software version 23.0 (SPSS Inc., Chicago, IL, USA). Since the data of VEMPs mismatch the normal distribution, the nonparametric Kruskal–Wallis test was performed to compare the difference between experimental groups (A, B, C) and control group (D). Moreover, the nonparametric Mann–Whitney test was performed to compare the difference between experimental groups (A, B, C) and control group (D). The categorical variables were expressed as numbers (percentages) while comparing groups was performed using the chi-square test. P value <.05 was considered to indicate statistical significance.
Results
Patients
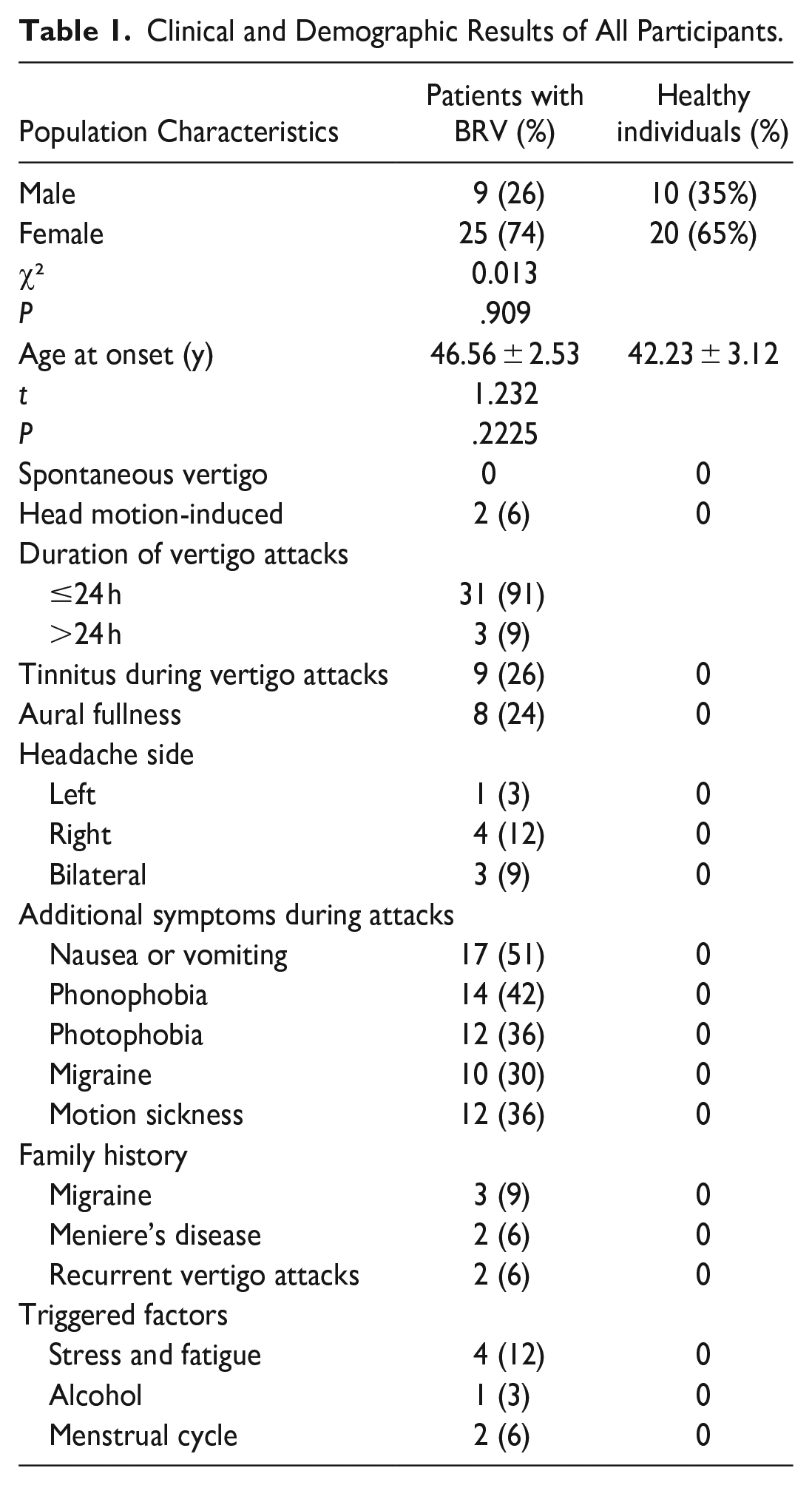
The study population (n = 64) consisted of 30 healthy volunteers and 34 patients, including 17 patients with BRV and ear symptoms, 11 with BRV and a history of migraine, and 7 with BRV sorely. The patients comprised 9 men and 25 women with a mean age of 46.56 ± 2.53 years, while the healthy volunteers comprised 10 men and 20 women with a mean age of 42.23 ± 3.12 years. Most patients in group A suffer from vomiting and phonophobia during the onset (100% and 82.4%), and some patients are accompanied by photophobia and migraine (70% and 59%). For Group B, only around 1/3 of patients had a history of migraines, while around 20% had a history of MD and recurrent vertigo attacks (Table 1).
Clinical and Demographic Results of All Participants.
cVEMP
At 500 Hz cVEMP, the elicitation rate was 81% in Group A, 86% in Group B, 78% in Group C, and 98% in Group D. The mean of cVEMP amplitudes of Group A and Group C was significantly different from Group D under 500 Hz, respectively (P = 0.017, 0.044). The cVEMP amplitudes of BRV patients with cochlear and BRV patients without cochlear symptoms and migraine history were lower than the healthy participant group at 500 Hz.
At 1000 Hz cVEMP, the elicitation rate was 81% in Group A, 91% in Group B, 72% in Group C, and 98% in Group D. The mean amplitudes of cVEMP in the BRV patient groups were significantly different between Groups D and A, and Group B, respectively (P = .008, .020). The mean amplitude of cVEMP in the BRV patients with migraine history and the BRV patients without cochlear symptoms and migraine history was significantly lower than the healthy participant group at 1000 Hz (Table 2; Figures 1 and 2).
Characteristics of cVEMPs in Different Groups.
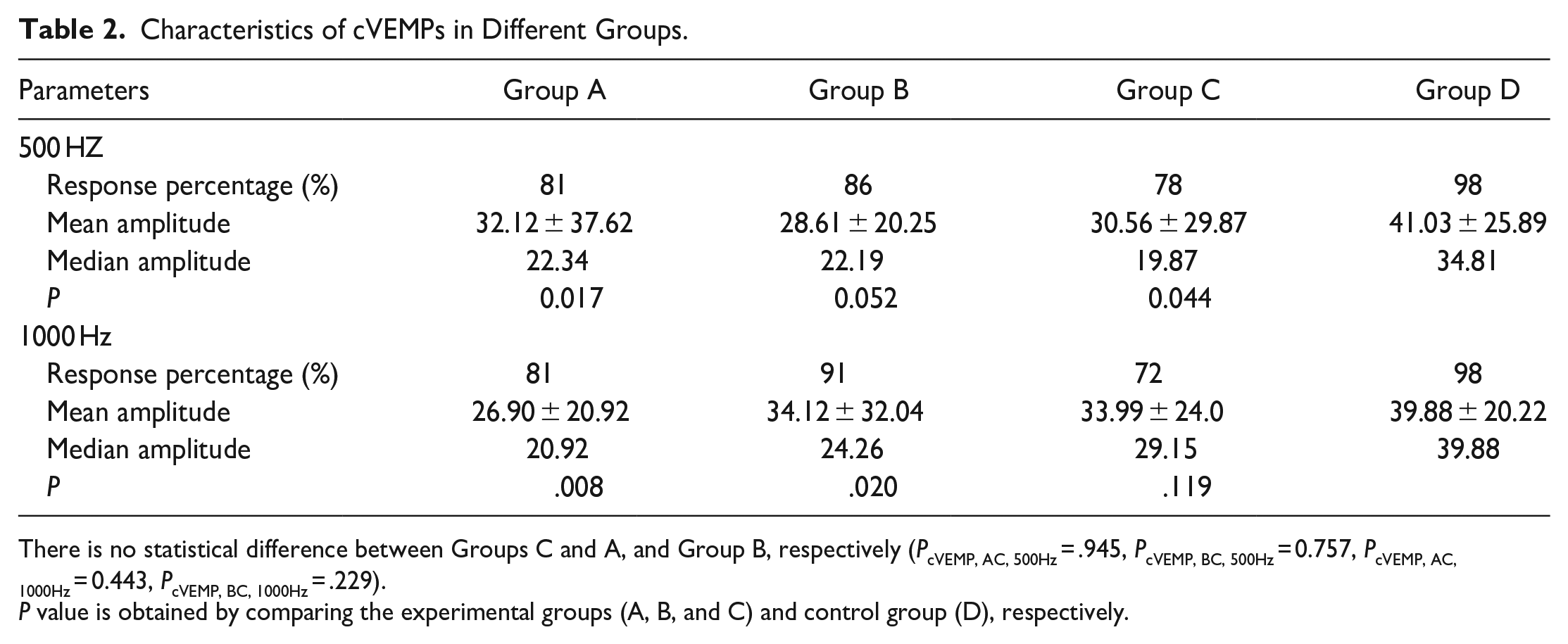
There is no statistical difference between Groups C and A, and Group B, respectively (PcVEMP, AC, 500Hz = .945, PcVEMP, BC, 500Hz = 0.757, PcVEMP, AC, 1000Hz = 0.443, PcVEMP, BC, 1000Hz = .229).
P value is obtained by comparing the experimental groups (A, B, and C) and control group (D), respectively.
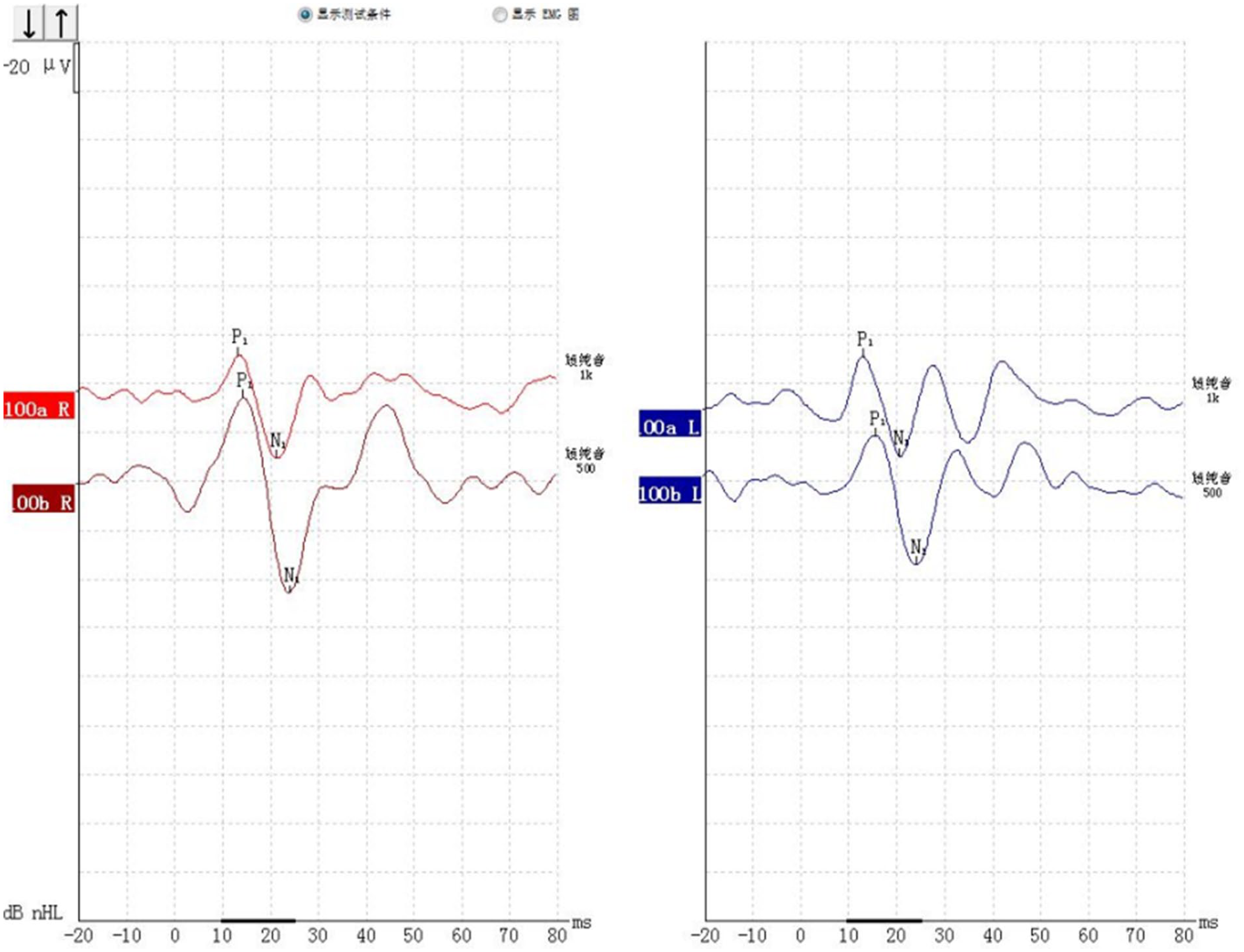
cVEMP under 500 Hz and 1000 Hz tracing from a 42-year-old healthy volunteer without any ear issues (P13/N23).
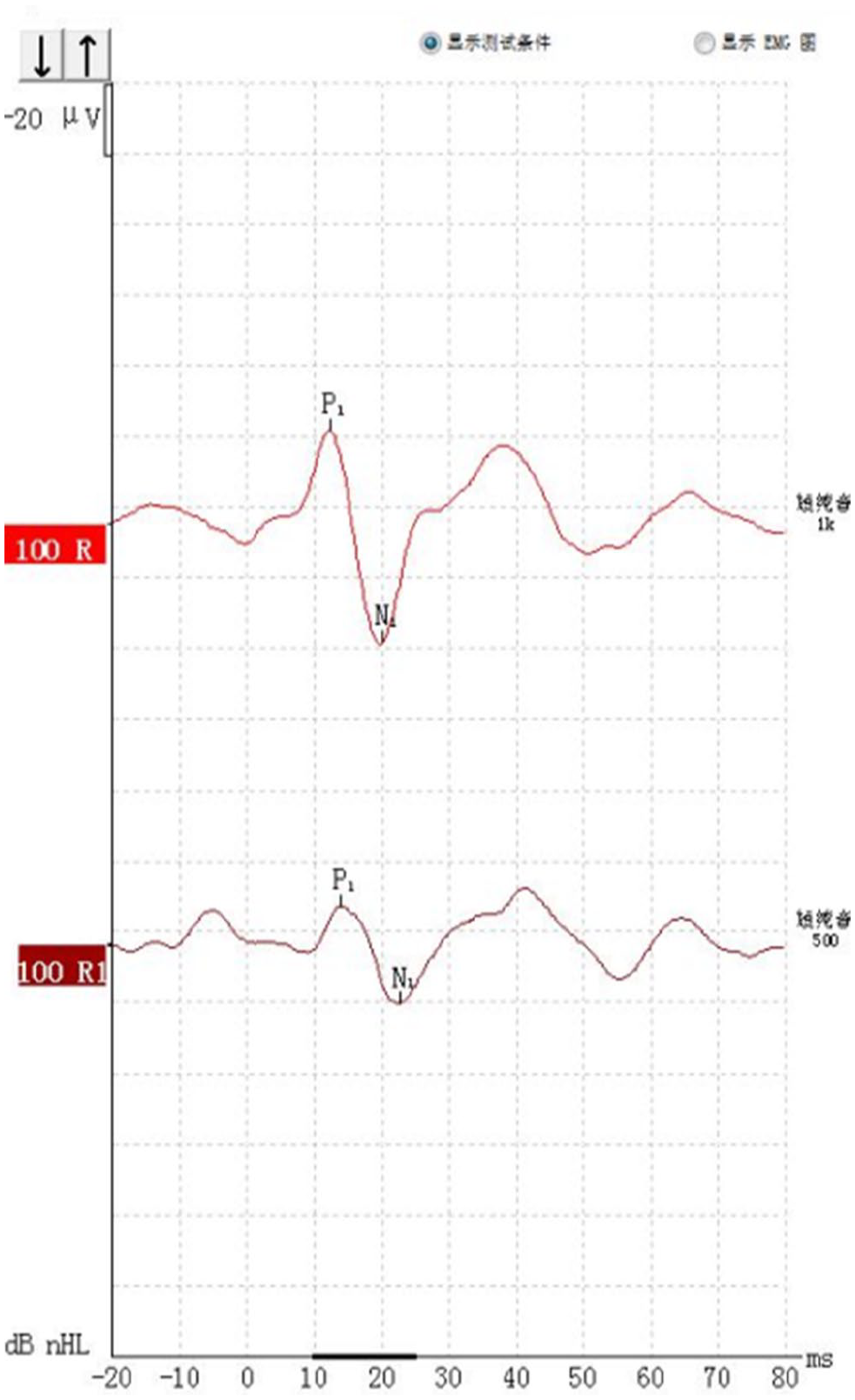
cVEMP under 500 Hz and 1000 Hz tracing from a female patient with BRV (P13/N23).
oVEMP
At 500 Hz oVEMP, the elicitation rate was 38% in Group A, 50% in Group B, 72% in Group C, and 83% in Group D. There was a significant difference in the mean amplitude between Groups D and A, and Group B, respectively (P = .029, .005). The mean amplitude of oVEMP in the BRV patients with cochlear symptoms and BRV patients with migraine history were significantly lower than the healthy participant group at 500 Hz.
At 1000 Hz oVEMP, the elicitation rate was 86% in Group A, 82% in Group B, 83% in Group C, and 95% in Group D. There was a significant difference in mean amplitude between Group D and Group A, respectively (P = .049). The mean amplitude of oVEMP in the BRV patients with cochlear symptoms and BRV patients with migraine history were significantly lower than in the healthy participant group (Table 3; Figure 3).
Characteristics of oVEMP in Different Groups.
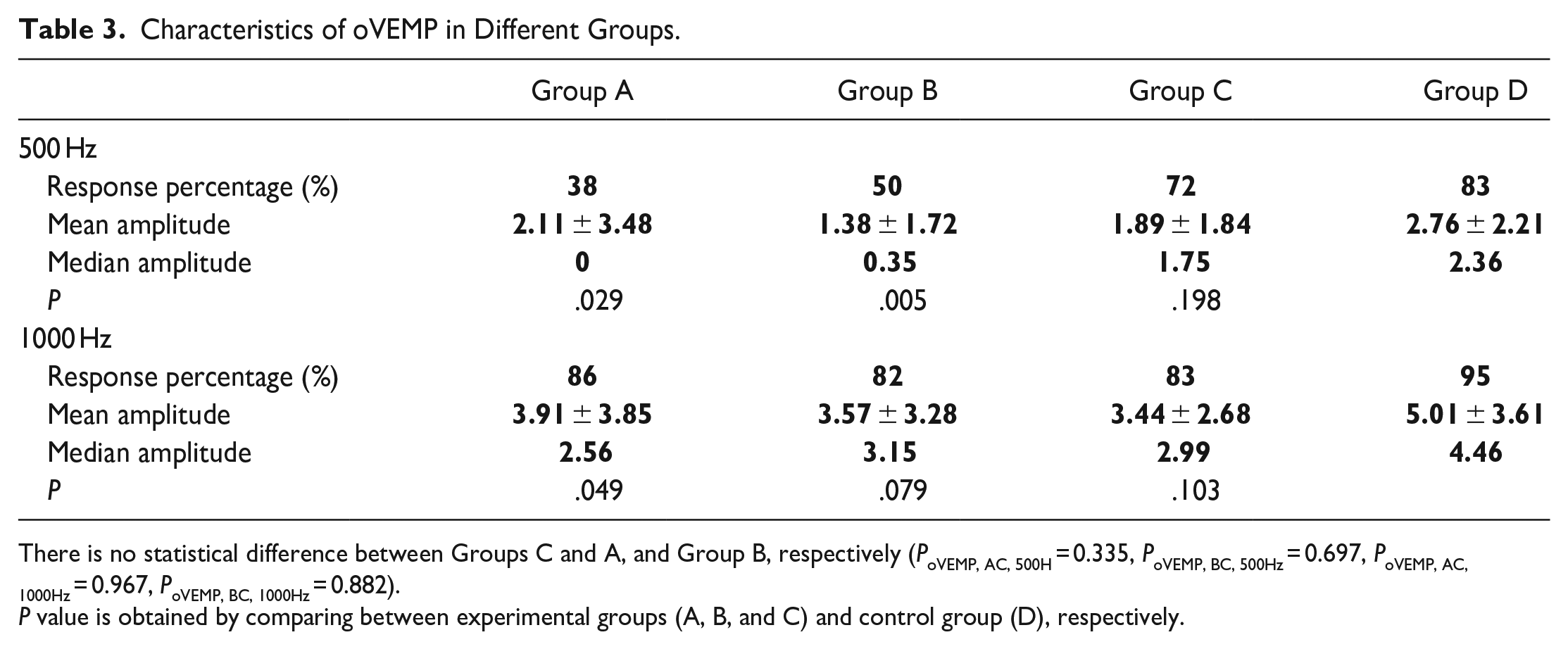
There is no statistical difference between Groups C and A, and Group B, respectively (PoVEMP, AC, 500H = 0.335, PoVEMP, BC, 500Hz = 0.697, PoVEMP, AC, 1000Hz = 0.967, PoVEMP, BC, 1000Hz = 0.882).
P value is obtained by comparing between experimental groups (A, B, and C) and control group (D), respectively.
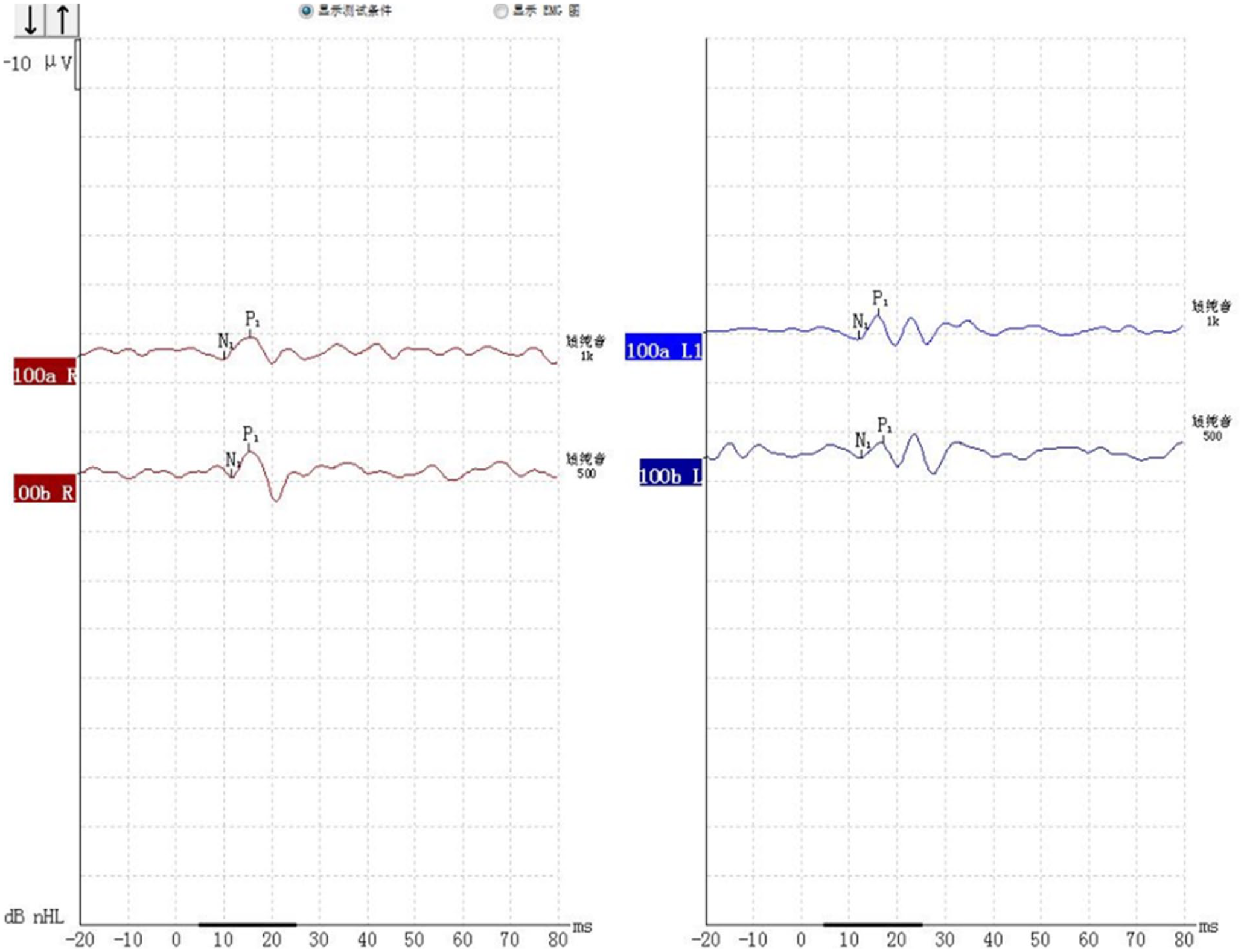
oVEMP under 500 Hz and 1000 Hz tracing from a 36-year-old female healthy volunteer without any ear issues.
Frequency Amplitude Ratio
There was no significant difference in the FAR of cVEMP between Group D and Groups A, B, and C, respectively (P = 0.525, 0.917, 0.374). Besides, there was no significant difference in the FAR of oVEMP between Group D and Groups A, B, and C, respectively (P = .678, .523, .427; Table 4).
Characteristics of oVEMP in Different Groups.
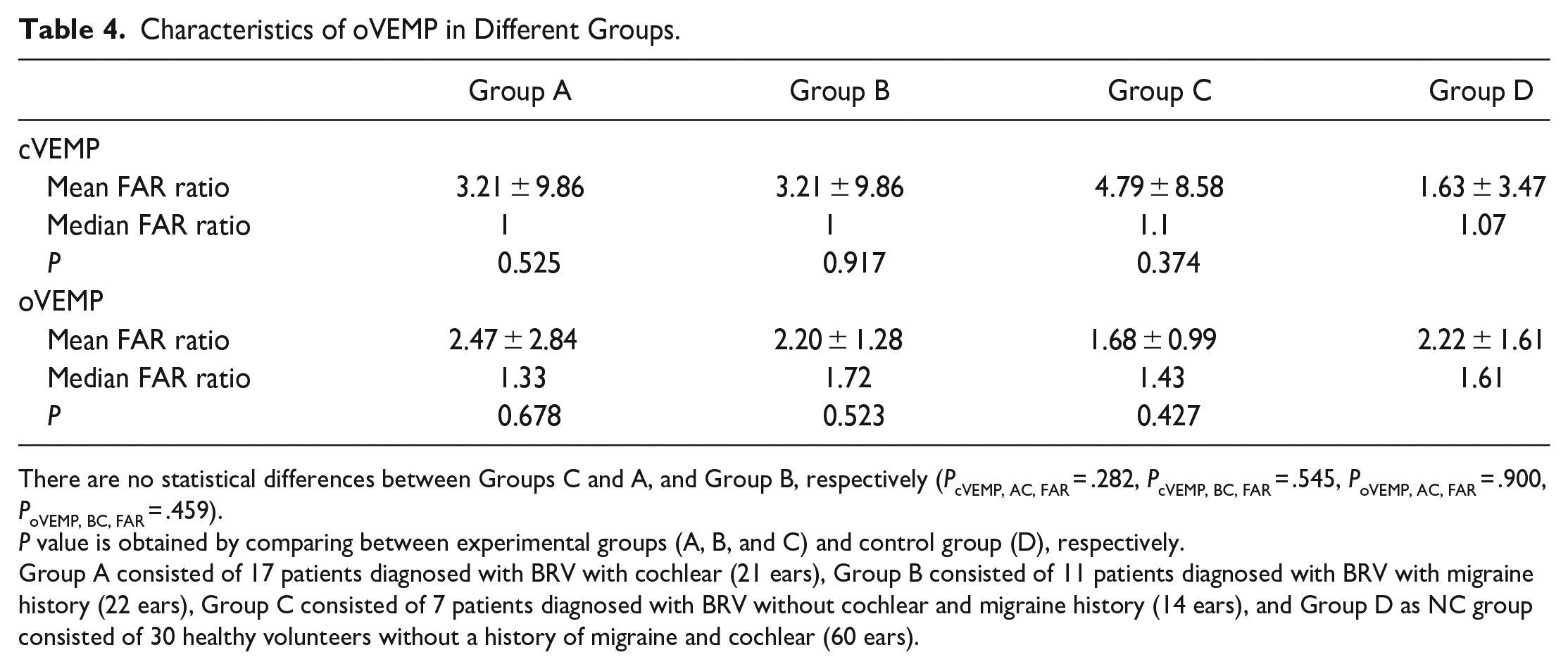
There are no statistical differences between Groups C and A, and Group B, respectively (PcVEMP, AC, FAR = .282, PcVEMP, BC, FAR = .545, PoVEMP, AC, FAR = .900, PoVEMP, BC, FAR = .459).
P value is obtained by comparing between experimental groups (A, B, and C) and control group (D), respectively.
Group A consisted of 17 patients diagnosed with BRV with cochlear (21 ears), Group B consisted of 11 patients diagnosed with BRV with migraine history (22 ears), Group C consisted of 7 patients diagnosed with BRV without cochlear and migraine history (14 ears), and Group D as NC group consisted of 30 healthy volunteers without a history of migraine and cochlear (60 ears).
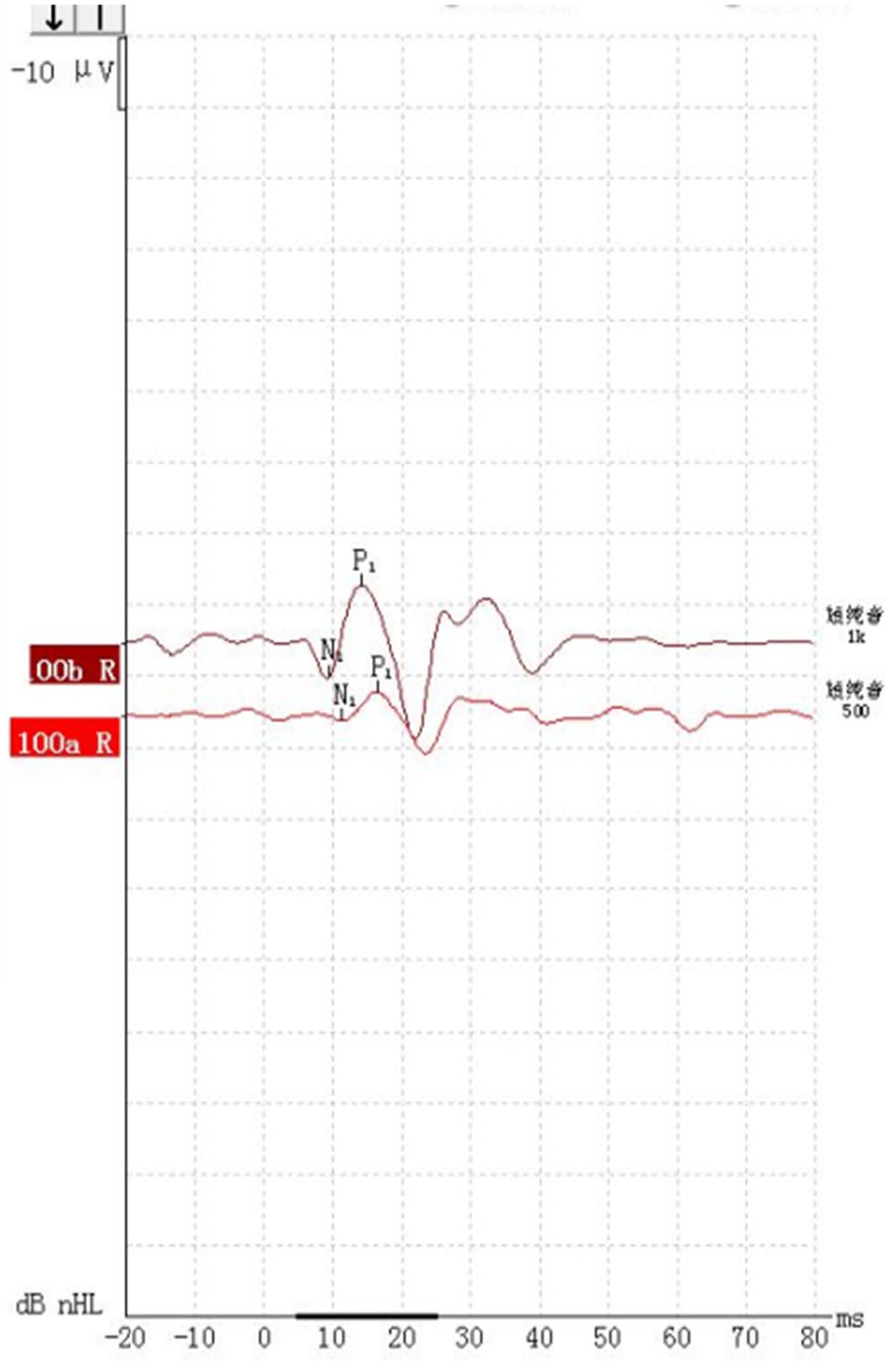
oVEMP under 500Hz and 1,000Hz tracing from a 28-year-old male BRV patient with cochlear symptoms (P15/N10).
Discussion
This study recruited 30 healthy participants as a control group (Group D) and 34 BRV patients as experimental groups. Based on whether they had a migraine history and cochlear symptoms, the BRV patients were split into 3 groups: Group A (BRV patients with cochlear symptoms), Group B (BRV patients with migraine history), and Group C (BRV patients without cochlear symptoms and migraine history). All participants were requested to proceed with both oVEMP and cVEMP tests. This study evaluates the VEMP parameter changes caused by cochlear symptoms and migraine history at 500 and 1000 Hz. According to this study, the cVEMP amplitude under 500 Hz of BRV patients with cochlear symptoms and BRV patients without cochlear symptoms and migraine history were significantly lower than the healthy people. The cVEMP amplitude under 1000 Hz of BRV patients with migraine history and BRV patients without cochlear symptoms and migraine history were significantly lower than the healthy people. Besides, the oVEMPs amplitude of BRV patients with cochlear symptoms and BRV patients with migraine history are significantly lower than the healthy people under 500 Hz. In comparison, the oVEMPs amplitude of only BRV patients with cochlear symptoms is significantly lower than that of healthy people under 1000 Hz. Furthermore, the significant differences in VEMPs FAR between BRV patients and healthy people are absent. Finally, there are no differences among Groups A, B, and C separately in the VEMPs parameter. Therefore, we cannot rely on VEMP results to determine whether cochlear symptoms and migraine history accompany the BRV patients.
Based on the epidemiological characteristics research, this study found that BRV is common in middle-aged women, with a female-to-male ratio of 2.8:1 and a mean age of 46.56 ± 2.53 years. Compared with males, females could suffer from BRV with a higher risk, matching the result of the previous study. 8 About 91% of BRV patients had vertigo lasting less than 24 hours, and 3% of BRV patients had vertigo lasting more than 72 hours, similar to the duration of MD patients demonstrated in previous studies. 9 In BRV patients, vertigo could be accompanied by vocal photophobia and headache. Some scholars believe that those may be related to vestibular pain, while others believe MD can cause these manifestations.10,11 Cochlear symptoms such as tinnitus and ear swelling can be present in BRV patients. In addition, numerous patients have vertigo accompanied by nausea and vomiting. These clinical and epidemiological features of BRV are similar to the results of previous studies. 12
The primary etiology of BRV is otolith pathway disorders. The inner ear consists of a vestibular labyrinth, including 3 semicircular canals, otolith organs, the utricle, and the saccule. These structures are where the otolith which is sensitive to gravity is located. The BPPV could be caused by the otolith motion within the endolymph of semicircular canals leading to an unbalanced stimulus when the otolith dislodges from the utricle. 13 Based on the potential pathophysiology, there are 2 prevalent theories in medicine: Cupulolithiasis Theory and Canalithiasis Theory. Harold Schuknecht proposed that basophilic particles adhered to the cupula, making the posterior semicircular canal (PSC) susceptible to gravity in 1962. 14 Once the basophilic particle achieves a specific position, the increased particle weight would arouse the cupula motionless, leading to persistent nystagmus and dizziness in the patient in the leaned backward position. In contrast, Epley believed that the presence of BRV was associated with the free-moving densities in the PSC instead of fixed densities on the cupula. 15 He proposed that these particles would rotate upward about 90° along the length of the PSC, causing the glide of endolymph from the ampulla due to the inertia and gravity. Afterwards, the cupula deflects, generating nystagmus with dizziness in patients. In addition, a novel hypothesis related to the ion channel disorder was proposed. Owing to the similar phenotype between BRV and ictal ataxia type 2, presumed to be caused by ion channel disorder, BRV is probably associated with ion channel disorder.16,17 However, the underlying pathology of BRV is still unknown.
Apart from these hypotheses, since the length of vertigo attacks and concomitant symptoms in BRV patients are similar to those in MD, and some patients (4%-14%) in long-term follow-up of BRV eventually developed into MD, some scholars found that BRV and MD have a similar pathology, which is endolymphatic hydrops. 18 Currently, VEMP examination is the most reliable diagnostics for MDs with high sensitivity and specificity. 19 Therefore, this study focuses on describing VEMPs characteristics of BRV.
This study revealed that the mean amplitude of oVEMP in all groups of BRV patients was lower than that of the healthy individual group, with a statistically significant difference. Despite the absence of studies on VEMPs in BRV, there is a similar presentation of reduced amplitude in MD compared with normal VEMPs in MD. The pathology of BRV may be similar to that of MD. In addition, balloon and ellipsoidal sac function may remain intact in some MD patients with severe hearing loss, whereas endolymphatic hydrops would only happen in early MD patients. 3 The results of the VEMPs test are therefore not related to the degree of hearing loss but only to the degree of endolymphatic hydrops. This study also found that around 50% of BRV patients with vertigo were accompanied by tinnitus and increased ear congestion, and the duration of vertigo in BRV patients was mostly within 24 hours. These symptoms were similar to those of MD, which may be a manifestation of inner ear fluid accumulation. 20 However, patients with MD usually present with low-frequency hearing loss, and temperature tests often show mild paralysis of the affected semicircular canals. In contrast, patients with BRV usually have normal hearing and temperature tests.21,22 This may be related to the progression of BRV disease, suggesting that BRV is an early lesion of endolymphatic hydrops without the involvement of the semicircular canals and cochlea.
Previous studies have shown that the shift in optimal frequency from 500 to 1000 Hz manifests the specificity of MD and is called the VEMP frequency modulation phenomenon.5,6 It may be caused by the change in surface tension of the otolithic apparatus membrane due to the long-term accumulation of water in the endolymph, resulting in a greater resonance frequency at 1000 Hz. A study suggested that the VEMP frequency modulation originates from the electrical resonance of hair cells. 23 In contrast, Todd et al suggested that VEMPs modulation may be caused by changes in the surface tension and elasticity of ellipsoidal and balloon sacs after their water accumulation, thus changing the otolithic apparatus’ vibratory mechanical properties. 24 Moreover, the phenomenon of frequency modulation of VEMPs is also related to age. A study found that the optimal frequency could also shift to 1000 Hz in normal individuals in their 60s, which they considered could be related to the ageing of the ellipsoidal and balloon sacs. 25 In this study, the BRV patients with cochlear symptoms showed a significant decrease in both cVEMP and oVEMP amplitude at 1000 and 500 Hz. Nevertheless, the cVEMP amplitude at 500 Hz is higher than the cVEMP amplitude at 1000 Hz. The effect of otoliths on cVEMPs at 1000 Hz seems more remarkable. The difference between cVEMP amplitude at 1000 Hz and that of the healthy population is greater in otoliths than at 500 Hz. Furthermore, there is no significant difference between the FAR of BRV patients and healthy volunteers in this study, which means there is no significant modulation phenomenon. The potential reason is that the degree of inner ear fluid accumulation in BRV is mild, failing to reach the degree of pathological changes causing the otolithic membrane and cochlea, leading to the optimal frequency failing to shift. Furthermore, most BRV patients are middle-aged people whose otolithic apparatus are in a good state of compensatory function, which can explain the better prognosis of most BRV patients. Besides, a recent study indicated that the best frequency shift of MD prior occurs during acute episodes, while most of the BRV patients we studied were in the stable phase without vertigo episodes, potentially triggering no significant difference in FAR. 6 However, all experimental groups showed no significant difference to the control group. Due to the different causes and manifestations, FAR could be a diagnostic indicator of MD instead of BRV.
This study also investigated the elicitation rate of VEMPs in BRV patients at different frequencies. The elicitation rate of oVEMPs in Groups A and B was significantly lower than in normal subjects. The elicitation rate of oVEMPs at 1000 Hz was also significantly lower than in normal subjects, which indicates that the elliptical bursa sac function is more likely to be impaired in BRV patients with concomitant cochlear symptoms and migraine symptoms, suggesting that the BRV pathological mechanism may be related to elliptical bursa effusion.
Limitation
The findings of this study must be seen in light of some limitations. Firstly, this study was conducted in a single center with a relatively small sample size, making migraine’s effect on VEMP inconspicuous. Therefore, larger sample sizes are required in future studies to prove the findings of this study. Besides, the relationship between cochlear symptoms, migraine symptoms, and BRV is unclear. Considering BRV accompanied by cochlear symptoms or migraine has an overall incidence in the population, it is necessary to clarify the possible underlying relationship between cochlear symptoms, migraine, and BRV. Finally, the cochlear and migraine symptoms could be triggered by different features, but no research revealed whether these features impact the BRV on VEMPs. The influence factors of cochlear and migraine symptoms could be a potential direction for understanding BRV.
Conclusion
This study revealed that BRV occurs in middle-aged women (74%) and lasts mostly less than 24 hours (91%). Both cVEMP and oVEMP under 1000 and 500 Hz could not be the diagnostic indicator of BRV. Also, VEMP FAR could not determine if the patients suffer from BRV. It is impossible to depend on the VEMP parameter to explore the relationship among BRV, cochlear symptoms, and migraine. However, VEMP could be a diagnostic indicator to determine the BRV patients with cochlear symptoms that the amplitudes of VEMP are higher than the healthy people. When the elicitation rate is 1000 Hz, the test result could be more sensitive than 500 Hz. To sum up, BRV onset may be related to otoliths, but more clinical data and follow-up studies are still required to improve the reference index.
Footnotes
Data Availability Statements
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/Consent Statement
This study was approved by The Ethics Committee of First Medical Center of People’s Liberation Army General Hospital. Participants have provided their written informed consent to participate in this study.
Grant Number
None.