
Abstract
Introduction
Hearing loss in children is a serious condition that can significantly delay language learning, speech, and cognitive development. 1 Thus, managing hearing loss-induced speech and language delays is achievable and requires early identification and management.2,3 A major burden falls on adults as well, since hearing loss can greatly impact their quality of life and lead to serious morbidities.4,5 Cochlear implantation has been proposed for hearing rehabilitation as the method of choice for managing sensorineural hearing loss owing to different conditions in different age groups.6,7 The procedure significantly enhances hearing and speech perception, reducing morbidities and improving the quality of life and health of Cochlear Implant (CI) users.8-11 Nonetheless, such an approach requires and mandates the integration of a quality-controlled concept and an interdisciplinary team that can provide the best quality from the indications to patient selection and long-term application. 12
The duration of CI surgery is relatively short, taking an average of 2 to 4 hours. However, it requires additional steps and care to optimize the outcomes. The patient then undergoes various reprogramming and follow-up sessions to improve their speech perception and examine the implant, as well as adjust the fitting settings. 12 This process of early activation after CI has evolved considerably over the past few years. For instance, we witnessed the transition of device activation from weeks to only 1 day after CI or immediately after the surgery in some studies.13-16 This notable shift necessitates more light to be shed on this subject. There are some review articles that discussed the early activation of cochlear implants from different views.17,18 However, there is a need for further discussion of the early activation of cochlear implants from a chronological and historical view. In addition, no studies discussed the benefits of globally standardizing the early activation process. The present literature review discusses the chronological evolution of early activation and its definition among the relevant studies, in addition to the benefits of standardizing the early activation process in implantation centers worldwide.
Methods
A comprehensive literature search was conducted in major databases such as PubMed, Scopus, and Embase to retrieve all the relevant articles that reported early activation approaches following CI. Furthermore, a search in the citations of Google Scholar and regular Google websites was carried out to find any potentially relevant information.
Discussion
Conventional Activation
The CI activation process might differs between adults and children. In adults, a behavioral approach is used for fitting in addition to evaluating single electrode channels for their thresholds and stimulation levels. After this, clinicians can easily balance the loudness between channels, define the dynamic range, and choose the speech processing strategy. The process of activation typically takes place 4 to 6 weeks post-surgery. However, this decision is based mainly on practice and general evidence, as clear or precise guidelines for the timing of fitting are lacking in the literature. 19 This delay in activation is pursued as its thought to give time for the healing process to complete and for surgical swelling to subside.6,7,14,20-24 Hearing and speech training is usually conducted even during the first fitting session.
In addition to the behavioral approach, fitting in children could take place by objectively assessing different parameters, including electrically evoked compound action potential (ECAP), Electrically Evoked Auditory Brainstem Responses (eABRs), and electrically-evoked stapedial reflex threshold (ESRT). Following CI, activation sessions can be the children’s first experience with sound; it could be an exciting prospect, yet a source of anxiety to both children and their families.19,25 The first fitting session mainly aims to create a “first pass” at a speech processor program, introduce sound to the child, and fit the external audio proecessor. Following this, subsequent programming sessions are arranged to optimize the implant system and boost the child’s ability to perceive speech.
Minimally Invasive Technique
The field of CI has witnessed several advances in the past few years. These advances favor the use of this modality and enhance its outcomes to be more suitable for use by the patient. Performing minimally invasive or robotic surgery for CI has been proposed by experts in the field due to its outstanding outcomes.26-33 This technique shows that determining pre-operative ideal trajectories is feasible, allowing for safe and effective drilling from the mastoid surface to the cochlea. Some of the reported advantages of this technique include an accurate positioning of the electrodes, reduced insertion trauma, less hair removal, improved cosmesis, and a shorter duration of surgery. 34 Accordingly, it has been demonstrated that minimally invasive techniques can greatly overcome the disadvantages usually reported with the classical technique.35-37
This technique is mainly conducted by performing mastoidectomy with a small incision. Using a soft technique during the round window/cochleostomy approach can remarkably overcome the adverse events that might affect the cochlea secondary to drilling-induced trauma. This has been achieved by covering the round window/cochleostomy with Healon, which significantly lowered the amount of loss and perilymph contamination by bone dust/blood clots and air bubbles during the electrode insertion. 38 Applying these approaches can significantly enhance the healing process by reducing the disturbances of the cochlear microenvironment.
Reducing the Time of CI Activation From Weeks to Hours
Within the last decade, some studies have been published to report the outcomes and feasibility of CI early activation. However, the timing of activation in this context is inconsistent among studies as it can range from weeks to only 1-day post-surgery,10,13-16,20,21,23,24,39-43 although most relevant articles referred to it as early activation. In this section, we will give a chronological discussion about the evolution of activation time after CI.
Marsella et al 21 reported the approach of early activation after CI, which was presented at the 11th European Symposium on Paediatric Cochlear Implantation in Istanbul, Turkey, May 23 to 26, 2013. The paper was then published in 2014 in Otology and Neurotology. 21 The authors defined conducting early activation as CI activation 1 week after surgery. For comparison, they included a control group, where activation/switch-on was performed 1 month after surgery. It was concluded that early activation is feasible and safe, and conventional activation is not rational. However, the authors recommended considering some factors that might contraindicate early activation. For instance, it should be avoided in children that develop early postoperative complications, including receiver-stimulator instability, edema/serum collection around the receiver-stimulator, and wound infections. The authors also suggested drilling a tight pocket for the receiver-stimulator, together with applying firmly fixated implants, to further ensure the safety and feasibility of early activation, concluding that early activation may be planned as early as possible to proceed with activation and relevant follow-up procedures as the patient is hospitalized.21,44
In 2013, another paper by Chen et al 38 reported approaching early activation in their CI population. However, it should be noted that Chen et al 38 demonstrated that approaching early activation was long and routinely practiced in their department, indicating that this approach might be older than 2013. However, no evidence beyond this date highlighting early activation exists in the literature. This might suggest that early activation might have been long practiced, especially as the authors stated the feasibility of activation within the first 24 hours from CI. They indicated the possibility and safety of the procedure and the excellent hearing and speech outcomes of their candidates.
In 2014, Alsabellha et al 20 reported that early activation was conducted 5 days post-implantation. Another report, published from Saudi Arabia in 2015 by Hagr et al, 14 demonstrated the feasibility of early activation 1 day post-implantation. In the same year in Austria, Wolf-Magele et al 23 published that early activation was practiced 2 weeks post-implantation. This shows that there was no agreement on the timing of early fitting in these studies. As in convergent years, different studies defined different timing for CI early activation, such as Alsabellha et al 20 and Wolf-Magele et al 23 defined the early activation as 5 days and 2 weeks post-implantation. Whereas, Chen et al 38 and Hagr et al 14 indicated the feasibility of early activation 1-day post-implantation. Keeping in mind, the 2 studies by Hagr et al 14 and Alsabellha et al 20 were conducted in the same center, one year apart, following the approach of early activation gradually, starting from day 5 to day 1-post-op. Thus, Signifying the lack of clear guidelines regarding the best practice of early activation, as well as the cohesion of evidence-based publications in this regard.
Following these studies, various investigators conducted early activation at 1-day post-implantation between 2015 and 2021.10,13,15,16,39-43 Moreover, in 2021, Saoji et al 16 practiced activation on day 0 (within 5 hours) and day 1 post-CI in their early activation group. The authors demonstrated that early activation, whether in the same day of the surgery or 1-day post-implantation, is feasible and does not have a long-term impact on electrode impedance. Interestingly, a study conducted by Batuk et al 39 2019 defined early activation as activation between 1 and 7 days post-implantation. They also included a control group with activation at ≥8 days post-implantation. Similarly, Günther et al 45 reported that early activation was conducted at <8 days from CI in 2018. Other authors also considered activation at 10 to 14 days post-implantation as conventional and not early.16,41,42 These contradictions raise questions about the definition of early activation among studies in the literature since early activation was previously defined as activation conducted 2 weeks after surgery. 23 This further highlights the inconsistency in defining early activation among the published studies. Table 1 shows summary of the studies that approached early activation.
Summary of the Studies That Approached Early Activation.
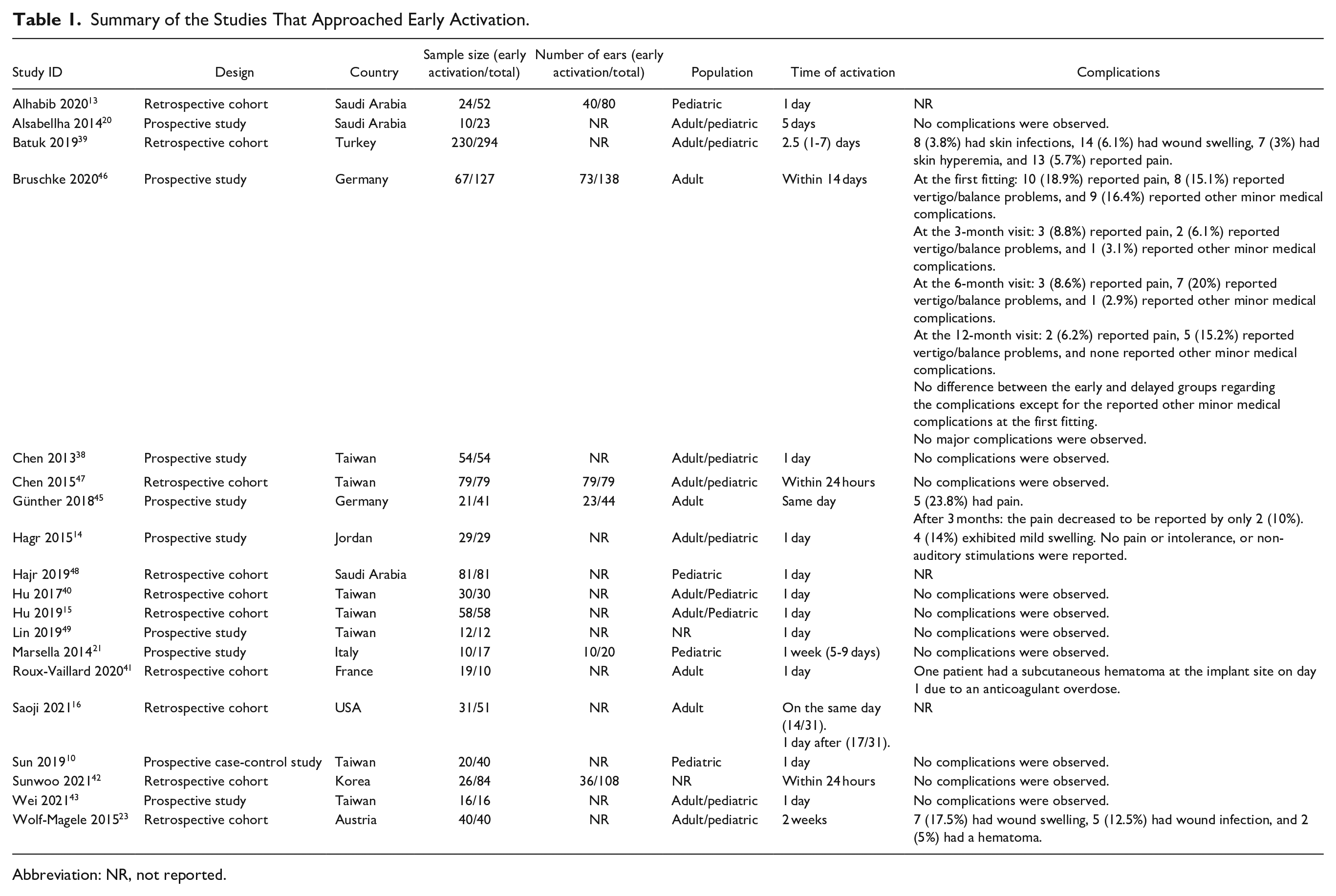
Abbreviation: NR, not reported.
The Importance of Early Activation
As it is traditionally practised, CI activation typically takes place within 4 to 6 weeks after implantation.6,7,14,20-24 Although, as stated, there are no guidelines or evidence to base this duration on. It has been advised by experts to allow enough time to ensure electrical stability or the need for alternations in impedance levels after implantation, magnet placement, and proper wound healing. Patient compliance might also be impacted secondary to developing postoperative pain.50,51 With that being said, this delay is mainly attributed to the surgical procedure, including the hard technique required for cochleostomy and the generally large-scale skin wound. However, experts have recently explored the possibility of early activation and addressed these concerns. For instance, overcoming concerns regarding wound healing, pain management, and other peri-operative complications was achieved by introducing a minimally invasive procedure for CI. This new surgical technique offers reduced operative time, smaller incisions, less inflammation, faster healing, and earlier device activation.14,38 Using a good flap design with sufficient venous drainage and arterial supply allows for closing the wound in layers with no tension secondary to an enhanced exposure of the surgical area. 52
Nonetheless, this might not be feasible for all CI users as flap thickness varies. For instance, erosion of too-thin flaps might occur due to magnetic pressure.53-56 Therefore, conducting early activation is not favorable in these patients. In such cases, it has been demonstrated that sound processors can be efficiently used shortly and safely.
Modifying the standard surgical procedure should be conducted in certain conditions, including malformations, hearing preservation, re-implantations, and obliterations of the cochlea. 12 Moreover, avoiding excessive trauma of hair cells was conducted by the skill of atraumatic insertion, including advanced Off-Stylet. 57 Some authors furtherly considered the restitution of electrical signals from the CI, inducing reciprocal interactions between peripheral and central auditory pathways. 38 Applying these approaches can significantly enhance the healing process by reducing the disturbances of the cochlear microenvironment.
Furthermore, following CI, fibrosis might develop, which can limit the function and outcomes of the procedure. It can encase the electrode array and intervene against a proper electrical stimulation delivery to the acoustic nerve.6,46,58-63 Therefore, conducting early activation before the development of fibrosis might enhance the outcomes of the procedure, leading to reduced impedance levels.10,13,16,20,21,38-42
Another benefit of conducting early activation might be gaining extra weeks of brain plasticity, thus, enhancing the implant adaptation due to reducing the interval between the time of surgery and activation. This process is referred to as “no mute interval” (ie, with no implantation or hearing aids). However, such evidence remains hypothetical, and further studies should investigate it.
Most importantly, the efficacy and safety of early activation are not inferior to the conventional activation approach. Most published studies showed that impedance levels and ECAP values after early activation are comparable with conventional activation.10,13,16,20,21,38-42 Furthermore, some papers demonstrated that impedance levels might even be lower after early activation, leading to better electrical stimulation effects than conventional activation.10,13,16,20,21,38-42 Furthermore, these studies showed that impedance levels were comparable to conventional activation groups at different time intervals from 1 to 12 months (last follow-up period). Although some complications, like pain, vertigo, infection, swelling, skin hyperemia, crusty ear canal or scar, and swollen device bed, were reported in some populations, the authors stated that they were negligible and did not impact the feasibility and efficacy of early activation.10,14,23,39,45,46 Most studies confirmed that no major complications were associated with early activation,13,15,16,20,21,38,40,42,43,47,49 Table 1. Moreover, studies showed that patients undergoing early activation showed significant improvement in hearing and speech perception outcomes using different assessment tools, including maximum comfortable levels, 20 the modified Mandarin speech perception, 10 the bisyllabic Fournier word recognition score, 41 the multisyllabic word test/the monosyllabic word test,45,46 the Meaningful Auditory Integration Scale questionnaire, the Ling Six-Sound test, and the Central Auditory Processing test. 21
Conducting early activation offers patients and their families both economic and psychological benefits 13 as it has been reported by Chen et al 38 that around half of the study participants were from outside the country where CI took place, indicating a significant relief in the economic burden that usually follows activation on these families. Hajr et al 48 also provided evidence regarding non-medical financial relief to families of patients undergoing early activation after CI. Having said that, early activation would even be more convenient for international patients and those who have traveled to an implantation center since CI might not be feasible in their countries due to limited resources.
Chen et al 38 also state that the participants and their caregivers are more satisfied with early activation of CI and it was associated with a significant reduction in worry and duration of uncertainty. For that reason, early activation allows patients and their families to pursue their daily activities within 2 days after CI, which is a major advantage over conventional activation. However, conducting early activation might not be optimal in certain situations where delaying the process of activation, to the conventional period, is recommended. For instance, conventional activation might be inevitable when the patient suffers from postoperative complications, like a hematoma. Accordingly, the best decision regarding the timing of activation should be based on the postoperative status of the patient and the anticipated outcomes. In another study, Günther et al 45 also showed that most of their patients (84.2%) were satisfied or highly satisfied with early activation, and more than two-thirds of the study participants (70%) were satisfied with the listening experience at 3 months post-activation. Other studies also reported similar findings, indicating high patient satisfaction with the procedure.23,41
Expert Opinion
All the mentioned factors above favor approaching early activation. Based on that, the question should be, why not approach early activation? Adopting the approach is feasible and safe and overcomes various burdens for patients and their families. Thus, we believe that approaching early activation should be standardized in the different implantation centers worldwide, especially in centers with global or remote patients that would require traveling and huge expenses. The exact timing of activation remains controversial since no adequate data is present in the literature regarding the definition of early activation and the feasibility of post-implantation timing over the other. However, early activation can be successfully conducted within the first few hours post-implantation, based on the current evidence. This might be a suitable option for many patients, although it might not be safe or convenient for others. Furthermore, since no apparent evidence contraindicates conventional activation, the timing should be based on a well-prepared pre-operative clinical and economic plan between patients, their families, and clinicians to decide what is more convenient. Future investigations should investigate the feasibility of self-fitting following the initial activation session, which might be more suitable to optimize the hearing device settings and attain the best hearing experience. 12
Conclusion
The field of CI witnessed significant advances within the past decades. A great evolution in the activation timing post-implantation has been noticed. It has been considerably reduced from 4 to 6 weeks in the conventional activation approaches to being conducted 0 day post-implantation and even hours following the surgery before the patient leaves the hospital. We found that early activation be further practiced since no adverse effects or contraindications could be found in the literature. It is essential to recognize the importance of conducting additional randomized controlled studies with larger sample sizes in order to strengthen the existing body of evidence. While existing research has provided valuable insights, expanding the scope of investigations through larger-scale studies can enhance the reliability and generalizability of the findings.
Footnotes
Acknowledgements
This research did not receive any specific grant.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/Consent Statement
Unrequired in reviews as per journal guidelines.
Data Availability
The data used to support the findings of this study are included within the article.