
Abstract
Paragangliomas are rare, slow-growing, hypervascular, catecholamine-secreting neuroendocrine tumors arising from the paraganglia. Paragangliomas are rarely found in the head and neck and are typically benign, presenting as a painless, slow-growing mass. Surgical extirpation in combination with long-term surveillance has been long regarded as the standard of care; however, the advances in imaging, radiation therapy, and embolization techniques have improved diagnostic and therapeutic modalities. We present a case of an 87-year-old female who had previously undergone resection of a paraganglioma in 1998, with no evidence of disease in 2002. Eighteen years later, the patient presented to the clinic with otogenic complaints. Imaging showed an expansive mass from the jugular foramen with bone destruction and opacification within the ear canal. The patient opted for observation. The patient eventually presented to the emergency room with neurologic manifestations. Imaging showed a cerebellar abscess prompting emergency drainage. Intraoperative cultures grew Prevotella loescheii and S. intermedius, and the patient was started on 6 weeks of IV antibiotic therapy. Debulking of the paraganglioma was performed followed several months by mastoid and ear canal obliteration; however, the patient experienced complications, including dehiscence of the external auditory canal and Clostridium difficile infection. The patient was eventually treated successfully, marked by a reduction in complaints, a return to baseline activities, and imaging showing no increase in tumor size.
Introduction
Paragangliomas are rare, usually benign, slow-growing, hypervascular, catecholamine-secreting neuroendocrine tumors arising from the paraganglia. Paragangliomas are extra-adrenal, typically occurring in the abdomen (85%), thorax (12%), and even less commonly in the head and neck (3%). 1 The annual incidence of head and neck paragangliomas is estimated to be 1 in 300,000, accounting for approximately 0.6% of all head and neck tumors. 2 The most common head and neck paragangliomas are found in the carotid body, followed by the jugular foramen, along the vagus nerve, and rarely in the larynx.3-5 Head and neck paragangliomas can present a diagnostic challenge for several reasons since they typically do not produce catecholamines. This is due to the fact that they arise from the parasympathetic ganglia and present as painless, slow-growing masses, which can eventually cause deficits in cranial nerves VII, VIII, IX, X, XI, and XII. These deficits notably lead to a decrease in the patients’ quality of life marked by dysphagia, hoarseness, Horner syndrome, and hearing loss resulting in a marked reduction in the patients’ quality of life.6-13
Traditionally, surgical extirpation has been the standard of care for managing paragangliomas. However, due to the remarkable vascularity of these tumors and proximity to neurovascular structures, surgical extirpation carries significant risks such as blood loss, speech and swallowing dysfunction, and increased risk of stroke, all of which negatively impact a patient’s quality of life.3,14-16 Over the past few decades, the evaluation and treatment approach has evolved significantly with various advancements. These include diagnostic imaging, stereotactic radiation therapy, and preoperative embolization techniques, which have contributed to improving patient outcomes and increasing an emphasis on observation and non-surgical treatment for the appropriate patient. 15
Case Presentation
An 87-year-old female was referred to the clinic in November 2020, initially presenting with otalgia, purulent otorrhea, imbalance, and a previous history of right-ear hearing loss that improved with antibiotics. The patient also reported having had a resection of a paraganglioma in the right ear in 1998. Post-resection, magnetic resonance imaging (MRI) in 2002 showed no evidence of disease.
On otoscopic examination, a nonpulsatile purple mass was visualized in the external auditory canal (EAC) with purulent debris. Audiometric testing revealed profound sensorineural hearing loss on the right and moderate high-frequency sensorineural hearing loss in the contralateral ear. On MRI, enhancement in the right jugular foramen extending into the right-ear canal with mastoid opacification was observed. On computed topography in the coronal view (Figure 1), an expansile mass was seen arising from the jugular foramen with bone destruction and opacification within the ear canal. Given the patient’s age and extent of ear disease, the head and neck tumor board was consulted and recommended either observation or subtotal resection and debulking. The patient opted for observation.
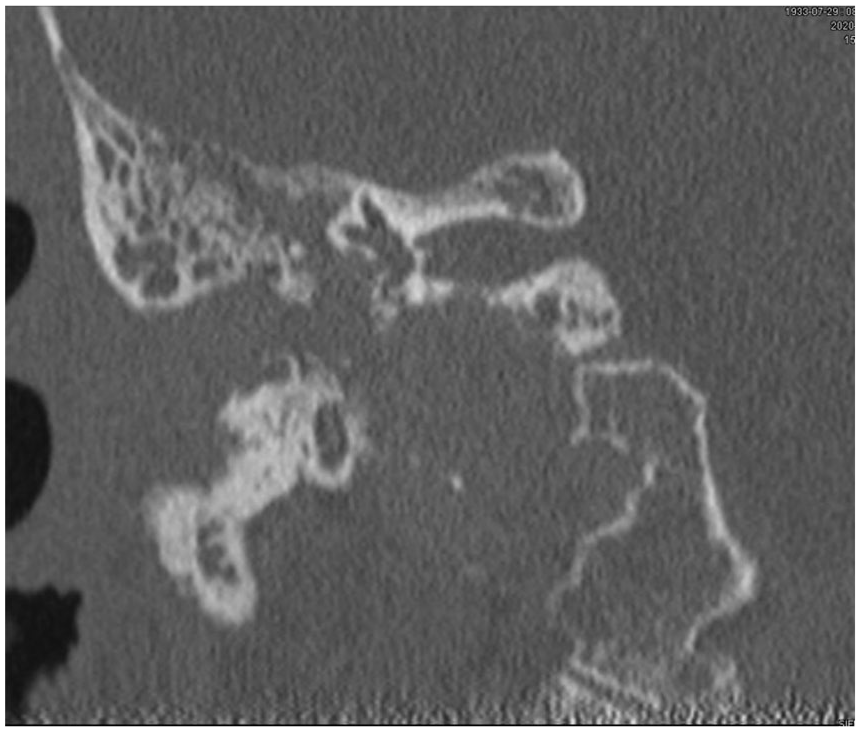
On computed topography (CT) in the coronal view, an expansile mass was seen from the jugular foramen with bone destruction and opacification within the ear canal.
Seven months after the patient’s initial visit, she returned to the clinic complaining of new-onset rust-colored otorrhea, particularly in the mornings. The patient reported no new pain or imbalance. The option to debulk the tumor was discussed, and the patient opted to continue observation.
Fifteen months after the initial visit, the patient returned with a 2-day history of otalgia, purulent otorrhea, and progressive dysphagia with solid foods but without complaints of dysphonia. The patient was started on antibiotics, and additional imaging was ordered; however, due to the COVID-19 pandemic, the patient was unable to schedule an imaging.
Her pain worsened over the next few days, and she developed an imbalance and headache without fever. Three weeks following her previous office visit, the patient was urgently admitted to the emergency room (ER) for confusion and headache. Imaging obtained in the ER demonstrated expansion of the jugular foramen mass, now with enhancing lesions within the cerebellum (Figure 2). A neurosurgeon was consulted, and the patient was taken to the OR for drainage of the cerebellar abscess. Intraoperative cultures grew Prevotella loescheii and Staphylococcus intermedius, and the patient completed 6 weeks of IV antibiotic therapy with ceftriaxone and oral metronidazole.
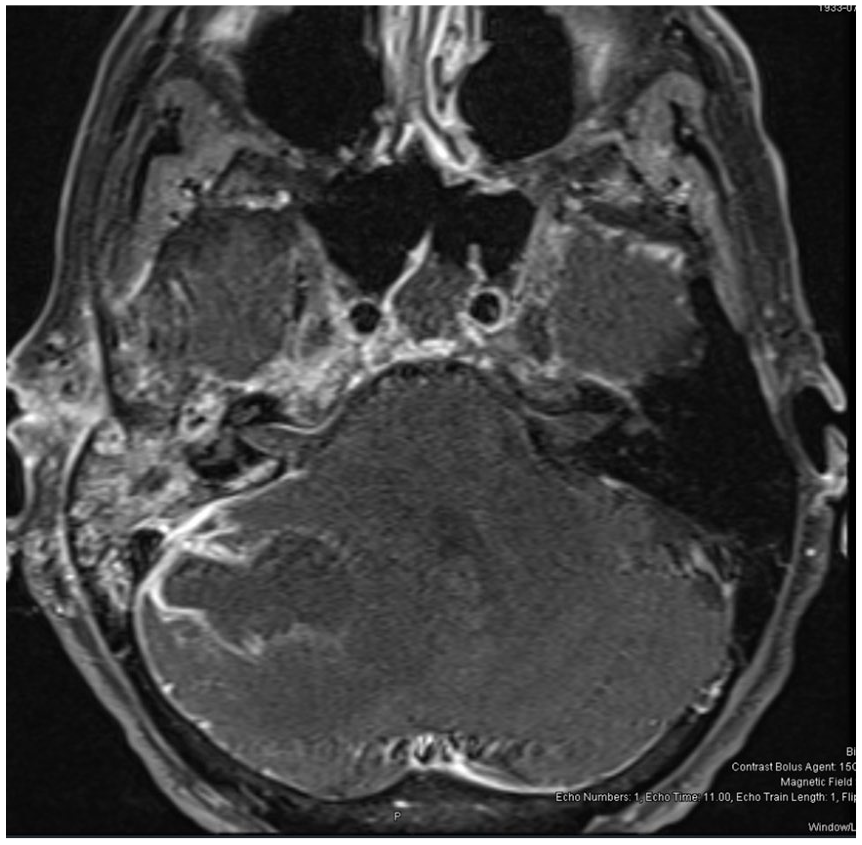
T1 fast spin magnetic resonance imaging (MRI) axial with contrast demonstrates rim-enhancing cerebellar abscess attached to dura at the mastoid.
Three months later, the patient underwent a preoperative embolization followed by a sub-total resection of the paraganglioma with oversewing of the EAC. Post-operatively, the patient developed a dehiscence of the EAC overclosure with some purulence. Wound exploration with irrigation and debridement was performed, and the wound was left open to granulate. Shortly after surgery, the patient developed Clostridium difficile and was treated successfully.
Over the next several months, the patient’s wound was managed with wet and dry packing. On follow-up in April 2023, the patient had no complaints or significant imbalance, EAC was granulating, and she returned to her usual active lifestyle. Most recent imaging showed no increase in the tumor size.
Discussion
Cerebellar abscesses are not common and can be primarily due to otogenic disease. A review published by Shaw et al 17 reported that cerebellar abscesses have a 41% mortality rate that is mainly determined by 3 factors: immunocompetence, reduction of posterior fossa mass effect by abscess excision and antibiotic coverage, and in the case of an otogenic abscess, an adequate radical mastoidectomy with bone removal to the site of attachment of the abscess to the dura mater. 17
The tumor that filled the auditory canal and extended down to the jugular foramen was resected; however, the disease within the jugular foramen was not removed, considering the patient’s advanced age and the possibility of a swallowing and voice disability as a consequence. A review of a 30-year experience with head and neck paragangliomas conducted by Valero et al 18 has demonstrated that while surgery is an effective treatment, non-surgical observation should be considered, particularly in the case of non-carotid body tumors.
Furthermore, the EAC was oversewn, given that at the time of surgery, there was a substantial amount of scar tissue visualized without the presence of pus or significant granulation. The intent was to eliminate the need for future office mastoid debridements. However, in retrospect, the residual tumor may have harbored bacteria, ultimately leading to the EAC overclosure dehiscence. The preoperative embolization served a dual purpose in this case since it could also aid in preventing further tumor growth by directly limiting the blood supply to the tumor, causing involution. Given the patient’s health at the time, radiation therapy will be considered if there are signs of significant growth on follow-up.
Conclusion
Paragangliomas, particularly those found in the head and neck region, are slow-growing and can present a diagnostic challenge before progressing. These tumors lead to a multitude of symptoms impacting a patient’s quality of life. This case illustrates a rare cerebellar abscess complication from a jugular foramen paraganglioma. Consideration should be given to whether this risk extends to other tumors within the temporal bone within non-sterile, mucosal-lined spaces, regardless of the histopathology. Various treatment approaches include diagnostic imaging, radiation therapy, and preoperative embolization techniques. These techniques provide pathways to improved quality of life, patient outcomes, and non-surgical treatment.
Footnotes
Consent
Informed consent was waived and not sought in our case study due to the lack of any identifying patient information.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Submission Statement
This article is original and has not been submitted elsewhere in part or in whole.