
Abstract
Keywords
Introduction
Radiation therapy (RT) and concurrent chemoradiation therapy (CCRT) are one of the primary modalities in the treatment of advanced head and neck cancer, and the mainstay of treatment for oropharyngeal cancer. 1 However, RT can cause complications that affect the quality of life (QOL), including xerostomia, dental caries, osteoradionecrosis, and skin necrosis. 2 Xerostomia, a subjective sensation of dry mouth associated with decreased salivation, is an important complication leading to dental caries, need for tooth extraction, and osteoradionecrosis of the mandibular and maxillary bone. 3 Hyposalivation caused by RT can also lead to mucositis, oral infection, difficulty of speaking, and dysphagia. 4 Therefore, it is important for the patients undergoing RT in the head and neck area to maintain salivary gland function and improve the QOL related to salivation.
As 60% to 65% of all saliva is produced in the parotid gland, the volume of the gland can be a predictor of overall salivary gland function, as well as of hyposalivation or xerostomia.4,5 Many studies have investigated the relationship between salivary flow and radiation treatment-related xerostomia.3,6 However, as this method of evaluating salivary flow requires additional, uncomfortable tests, it has limitations for use as a primary indicator of salivary gland function. Since periodic head and neck computed tomography (HNCT) is performed routinely during follow-up of head and neck cancer patients, it occurred to us that evaluating salivary gland function by this method might be useful, and would not require any additional, uncomfortable, and invasive tests.
Serial changes in parotid gland volume have not been thoroughly evaluated, especially after RT to treat oropharyngeal cancer. Furthermore, the ability of the parotid gland to recover after a prolonged period of RT treatment is largely unknown. We have used HNCT to evaluate serial changes of parotid gland volume and to analyze the relationship between volume change and xerostomia.
Patient and Methods
Subjects
This study was approved by the Institutional Review Board of a tertiary hospital. We retrospectively analyzed the patients with oropharyngeal cancer treated in this hospital, from November 2013 to August 2018. All patients underwent RT or CCRT with a dose/fractionation schedule of 67.5 Gy in 30 fractions with a definitive aim and 63 Gy in 28 fractions with a postoperative aim, respectively. RT was applied 5 days per week.
Evaluation of Parotid Volume
Patients underwent HNCT scans before radiation therapy (pre-RT), and at 6 months, 1 year, and 2 years after RT. The volume of the parotid gland was measured by HNCT, using Eclipse System version 11 (Varian Medical Systems, Palo Alto, CA, USA). Volume was measured by manually identifying parotid borders in continuous serial CT images by an experienced radiation oncologist (H.J.P) and physician (H.W.J) independently, who were blinded to the clinical data of patients and RT. The volume of the parotid gland was measured on the ipsilateral side of the primary tumor, or in tumors without laterality, such as base of tongue cancers located in the midline, the average parotid volume of the 2 sides was measured.
Evalutaion of QOL
QOL was evaluated using the EORTC QLQ H&N35 (the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire). Patients filled out the questionnaire at the time of HNCT scans. The EORTC QLQ is a well-known, widely used and validated questionnaire used to measure the physical, psychological, and social functioning of cancer patients. It evaluates 35 items, including 3 questions related to salivation; dry mouth (“Have you had a dry mouth?”), sticky saliva (“Have you had sticky saliva?”), and taste disorder (“Have you had problems with your sense of taste?”). The patients answer questions on a scale of 1 to 4 (1 “not at all” to 4 “very much”).
Statistical Analysis
Parotid gland volumes and QOL questionnaire scores at 4 consecutive times were analyzed by repeated analysis of variance. The relationship between parotid volume and individual components of QOL was analyzed with the Spearman’s correlation test. SPSS 21.0 (IBM, Armonk, NY) was used for statistical analysis. A P value < 0.05 was considered statistically significant.
Results
In total, 33 patients were enrolled in this study. The mean radiation dosage was 62.7 Gy with a standard deviation of 1.9 Gy, with a mean fraction of 29.6 (standard deviation 1.7). The highest number of cases was tonsillar cancer (25, 75.8%), followed by base of tongue cancer (7, 21.2%), and soft palate cancer (1, 3%). Twenty-one patients (63.6%) had concurrent chemotherapy, and 30 (90.9%) were pathologically diagnosed with squamous cell carcinoma (Table 1). The mean volume of the parotid gland before RT differed significantly from the volumes at all 3 post-RT time points (all P < 0.001, Figure 1). Mean volumes decreased from 23.30 mL pre-RT to 15.80 mL at 6 months, 15.93 mL at 1 year, and 16.67 mL at 2 years (Table 2). However, there was no significant difference between the 3 post-RT periods: 6 months, 1 year, and 2 years. No factors such as gender, primary site, pathology, or chemotherapy were related to the change in parotid volume (Table 3).
Demographics of Patients With Oropharyngeal Cancer who Underwent Radiation Therapy.
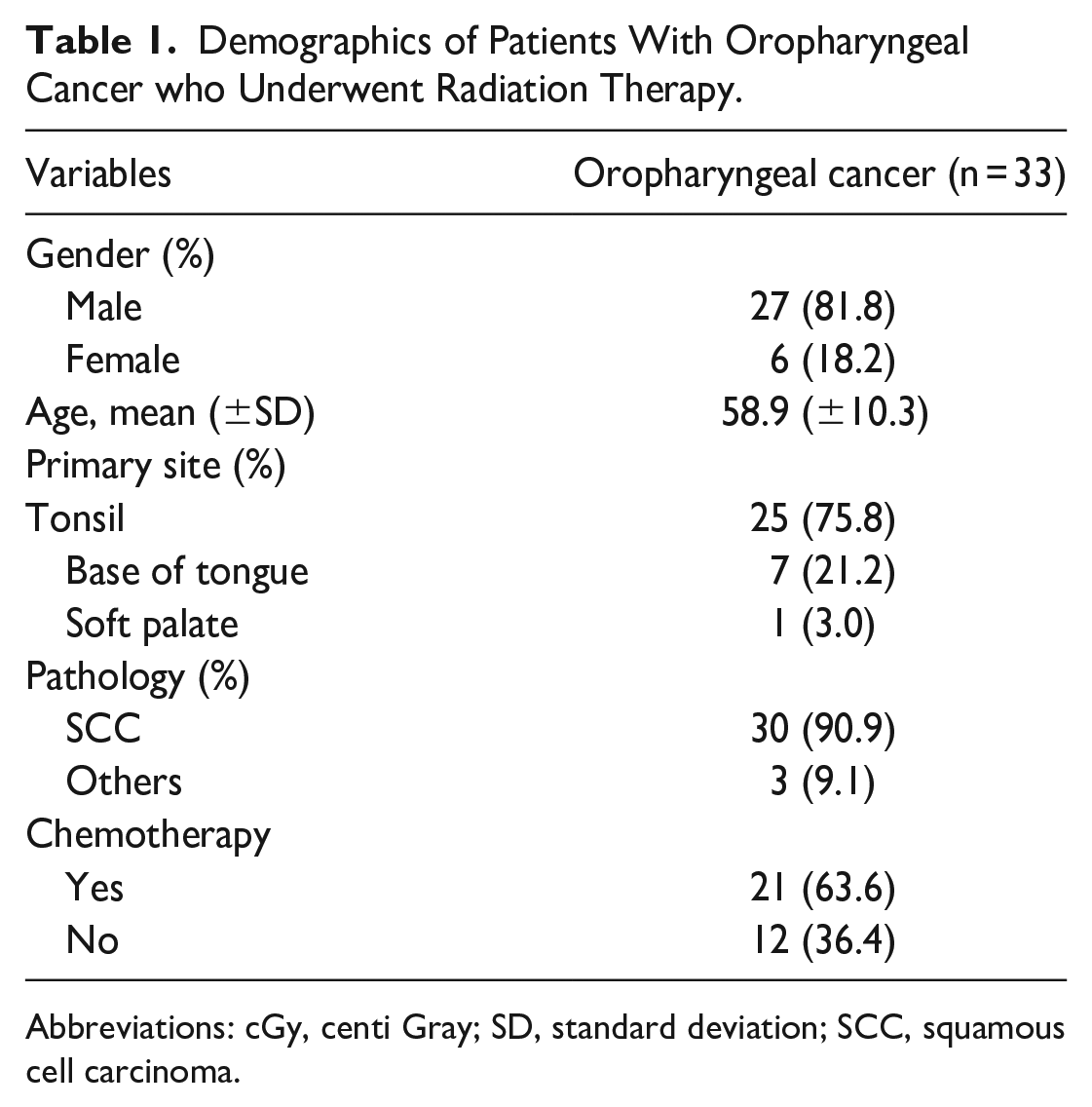
Abbreviations: cGy, centi Gray; SD, standard deviation; SCC, squamous cell carcinoma.
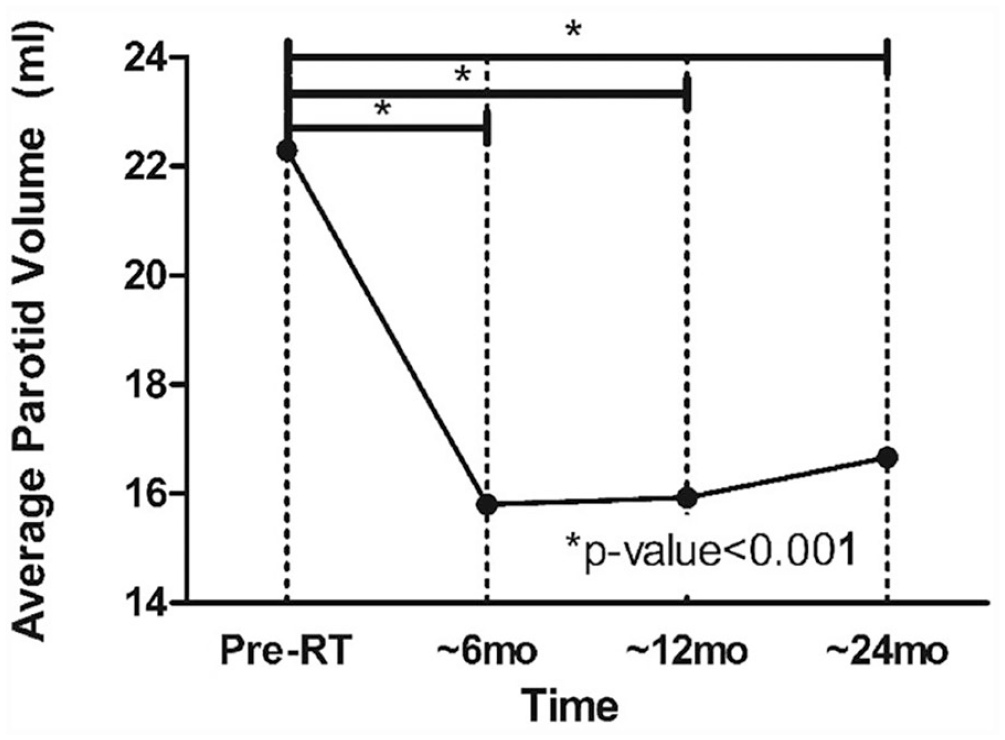
Average parotid gland volume changes after radiation therapy.
Mean Parotid Gland Volume and QOL Score at Each Time Point.
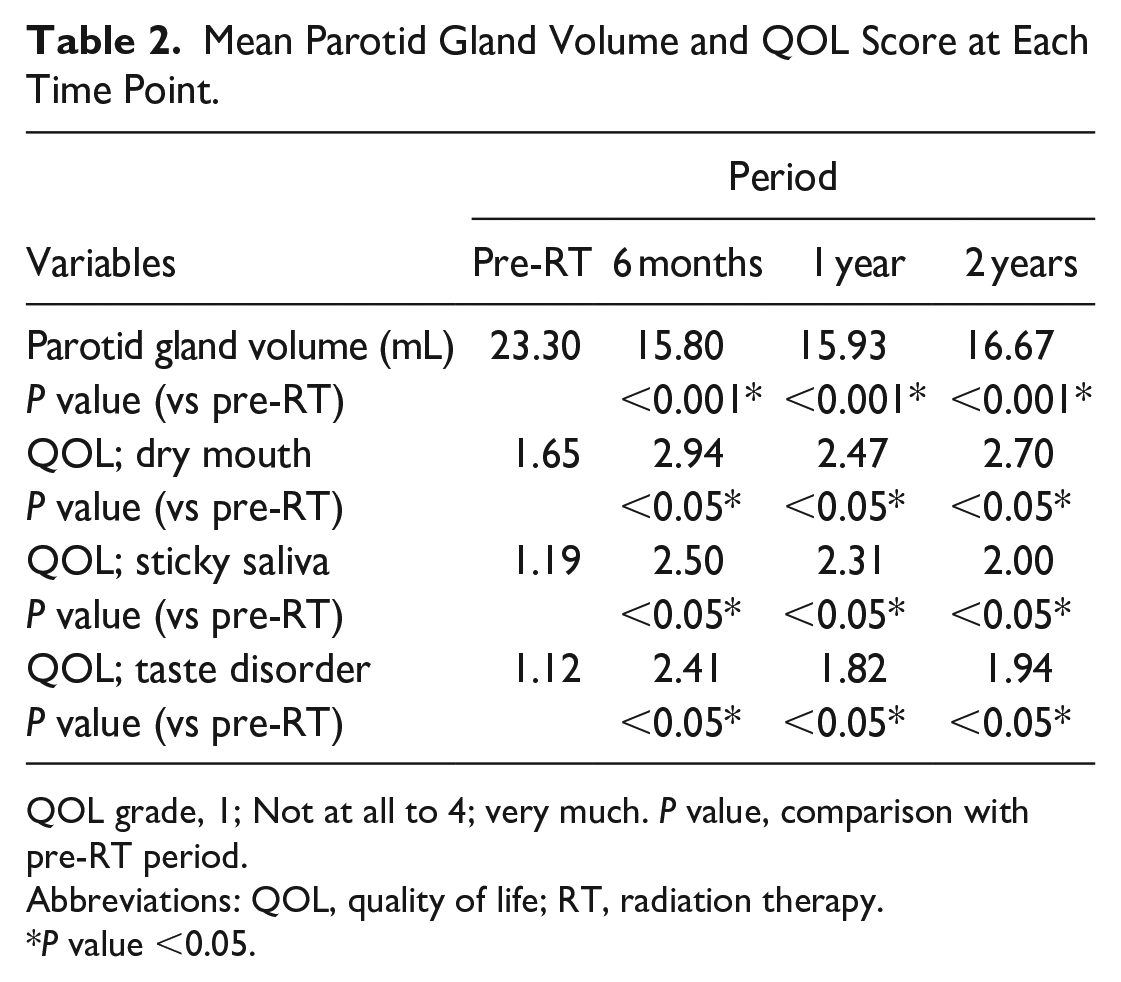
QOL grade, 1; Not at all to 4; very much. P value, comparison with pre-RT period.
Abbreviations: QOL, quality of life; RT, radiation therapy.
P value <0.05.
Average Parotid Gland Volume Change According to Clinical Factors.
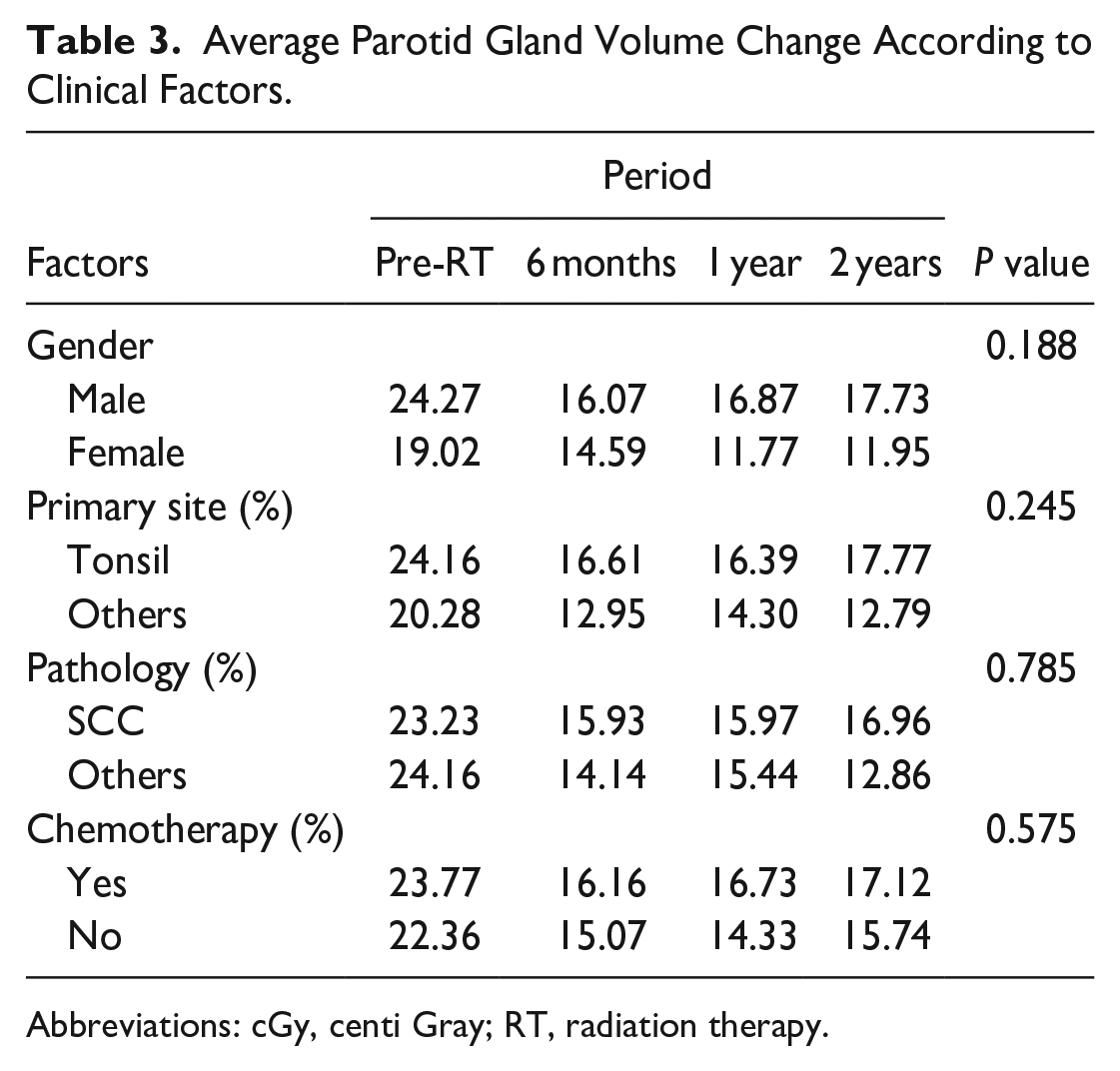
Abbreviations: cGy, centi Gray; RT, radiation therapy.
The mean QOL score increased (worsened QOL) straight after the RT (Figure 2) and 6 months, 1 year, and 2 years after RT (P < 0.05 for all 3 periods). The average score of saliva-related QOL was higher at 6 months, 1 year, and 2 years after radiation than pre-RT; “dry mouth” rose from 1.65 (pre-RT) to 2.94 (6 months), 2.47 (1 year), and 2.70 (2 years), “sticky saliva” from 1.19 (pre-RT) to 2.50 (6 months), 2.31 (1 year), and 2.00 (2 years), “taste disorder” from 1.12 (pre-RT) to 2.41 (6 months), 1.82 (1 year), and 1.94 (2 years). All 3 parameters of the questionnaire showed a significant negative correlation with parotid gland volume (P < 0.05 for each).
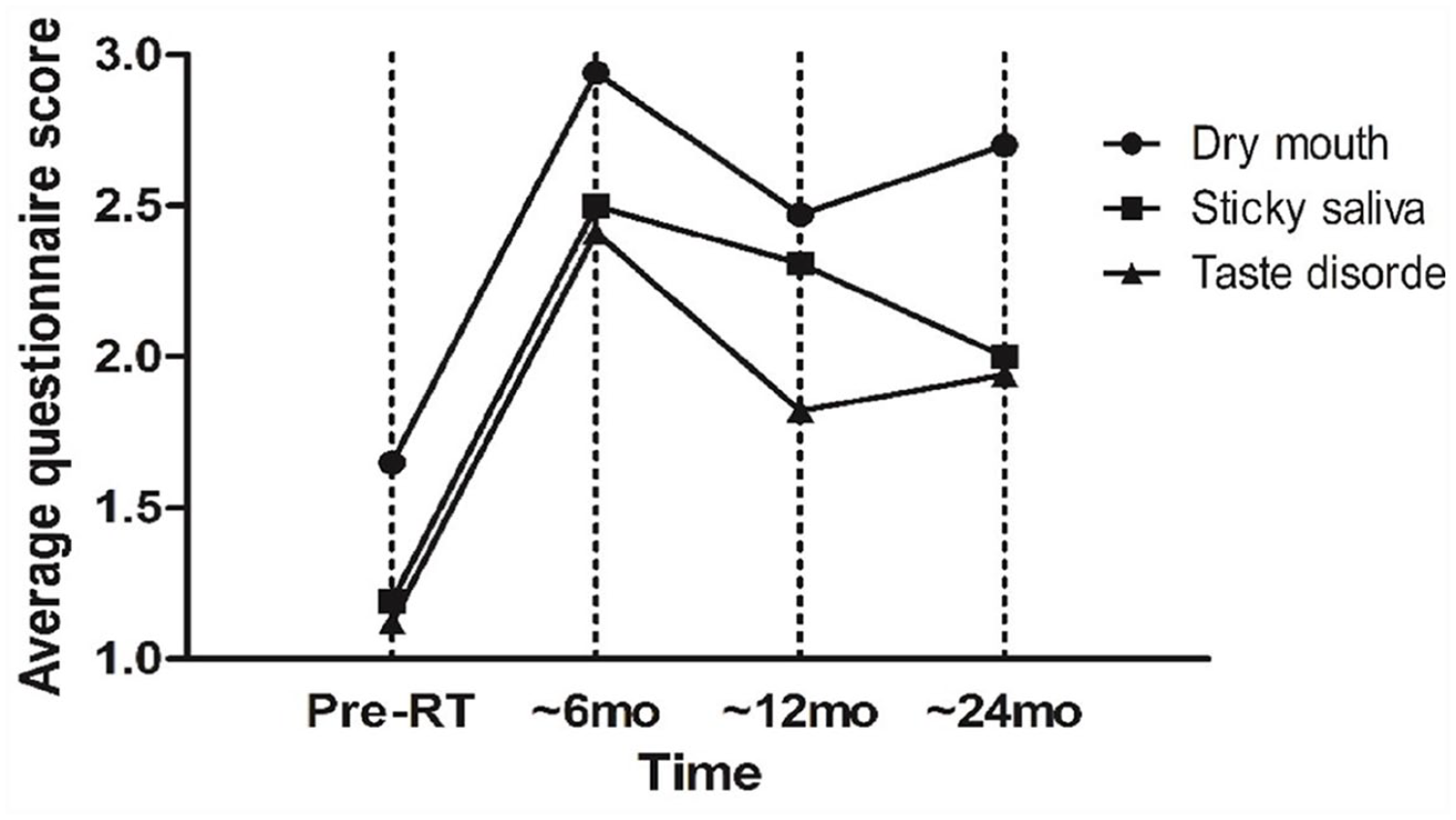
Average quality of life questionnaire score changes after radiation therapy.
Discussion
RT with or without concurrent chemotherapy is widely used to treat oropharyngeal cancer. 1 However, it causes damage to minor blood vessels and decreases blood flow in the head and neck region. 7 Moreover, this region contains many critical structures, including the salivary glands and thyroid glands, that can be damaged by RT. This damage has a negative impact on the QOL, associated with cosmetic and functional deficits such as xerostomia, dental caries, trismus, and skin fibrosis.2,8 One of the most common and significant side effects of RT is xerostomia, which is caused by irreversible cell damage of the salivary gland, especially in the serous salivary glands.2,5,7 There is evidence of a reduction in the volume of the parotid gland after RT.9,10 RT for oropharyngeal cancer often includes the major salivary glands because of proximity of the primary tumor and the pathway of lymphatic spread.
Several mechanisms may be involved in salivary gland dysfunction after RT. The acute functional damage may be induced by damage to the plasma membranes of the secretory cells, or apoptosis of the serous acinar cells. The later damage is thought to be caused by radiation-induced loss of acinar cells, or impairment of parasympathetic innervation and injury to vascular structures. 11
Although the volume of the parotid gland itself cannot reveal the occurrence of xerostomia, studies suggest a relationship between the change in parotid gland volume and saliva production. Most studies evaluating salivary function or salivary gland volume changes have dealt with oral cavity cancer, nasopharyngeal cancer, or hypopharyngeal cancer, as opposed to our study, which examined oropharyngeal cancer.12–14 Tasaka et al evaluated the volume of the parotid glands in patients with nasopharyngeal cancer treated with intensity-modulated radiotherapy for 5 years. 13 The volume of the parotid gland decreased after radiotherapy up to 3 years after RT. In patients who received less than 40 Gy total dose, the volume recovered significantly at 4 and 5 years after RT. Nguyen et al detected hyposalivation 3 months after RT by measuring salivary flow rate and defined hyposalivation as measured saliva weight less than 3.5 g over 5 minutes. 3 The authors reported more hyposalivation in bilateral 3-dimensional RT than unilateral RT. Teshima et al described a relationship between salivary gland volume change and saliva production: mean parotid gland volume decreased from 68 to 48 cm3 after RT. After RT, saliva production amount was not significantly correlated with parotid volume itself. However, the parotid volume ratio (post-RT volume/pre-RT volume) was significantly correlated with the amount of saliva reduction. 4 Although most studies compare only pre-RT versus post-RT levels and not serial changes in parotid gland volume, some found similar volume changes to ours. Sim et al reported a parotid gland volume decrease of 30% 3 months after RT of nasopharyngeal cancer, and partial recovery after 2 years, which is similar to our findings. 12
Our results point to a reduction in parotid volume of an average of 7.5 mL, and 32.96% in ratio 6 months after RT, compared to the pre-RT period. Parotid volume decreased significantly at 6 months, 1 year, and 2 years after RT. However, there were no significant differences between the 3 post-RT periods: 6 months, 1 year, and 2 years, suggesting that there was neither significant recovery nor long-term aggravation of parotid gland damage.
As xerostomia is defined as subjective symptoms of dry mouth, symptoms related to salivation are crucial for its evaluation. 3 EORTC QLQ contains 3 items reflecting xerostomia (dry mouth, sticky saliva, taste disorder), so the questionnaire provides important information during the patient follow-up. The scores on all 3 items increased after RT, and were correlated with the change of parotid gland volume. We found no clinical factors that were significantly related to salivary gland volume change by repeated analysis of variance. Most studies suggest that radiation dose influences salivary gland volume change. Nomayr et al reported a reduction in parotid volume of 26% after radiation of 3000 cGy, and of 40% after radiation of 7000 cGy. 15 However, all of our study subjects received 6000 to 6700 cGy of radiation, with no effect of radiation dose. This result may vary for cancers in other primary sites, including oral cavity, larynx, or nasopharynx, due to variation in the total dosage of radiation.16,17
There are conflicting results on whether the injured salivary glands recover after RT. 18 Li et al report that salivary production in patients who underwent RT with a mean dose <2500 to 3000 cGy recovered to pretreatment level after 2 years. 19 Braam et al report partial recovery of symptoms 5 years after RT, but recovery did not reach baseline levels. 20 We did not observe recovery of parotid gland volume and xerostomia up to 2 years after RT. This may be due to the higher dose of radiation, as our study subjects received more than 60 Gy of radiation.
Our study has several limitations. First, although radiation dose is an important factor affecting xerostomia, the radiation dose in our study was greater than 60 Gy and in a similar range due to the standardized regimen since this study was performed in a single hospital. High-dose RT is the preferred main regimen for the treatment of oropharyngeal cancer in our institution, which is a limitation for evaluating changes at lower doses. Second, although QOL is affected by xerostomia, we did not explicitly study a reduction in salivary flow itself. However, estimates of salivary flow or saliva volume are not precise, since total saliva cannot be evaluated throughout the whole day in a clinical setting for the treatment of cancer patients. An additional study is needed to show a direct relationship between parotid volume, salivary flow, and the QOL. We evaluated parotid volume and symptoms for 2 years after RT. Longer follow-up is needed to evaluate long-term changes in parotid volume and of QOL. Finally, we did not evaluate the volume of the submandibular gland, as we focused on evaluating the parotid gland, which is directly affected by radiation treatment.
Conclusion
The volume of the parotid gland decreased significantly at 6 months after high-dose RT and did not recover up to 2 years after RT. Symptoms related to salivation also appeared after RT and did not recover for 2 years. There was a statistically significant correlation between parotid volume and salivation symptoms at 6 months, 1 year, and 2 years after RT. Effects on parotid gland volume and their correlation with salivary function disorder should be considered in the treatment of oropharyngeal cancer.
Footnotes
Data Availability
All data generated or analyzed during this study are included in this published article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was performed in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Hanyang University Hospital (#2019-03-013)