
Abstract
The clinical diagnosis and treatment, including information such as age, history, clinical symptoms, signs, audiology, imaging examination, mode of operation, and postoperative follow-up, of a patient with suppurative temporomandibular arthritis caused by chronic suppurative otitis media were analyzed. As conservative drug treatment and drainage surgery were ineffective, the patient was treated with microscopic open radical mastoidectomy, tympanoplasty, the plasty of the cavity of auricular concha, facial nerve decompression, coarctation of the mastoid cavity combined with otoendoscpic resection of the lower temporomandibular lesions, and standard anti-inflammatory treatment after surgery. The patient appeared to be cured at the 3-month follow-up. The ear canal was dry, without any preauricular swelling, purulent ear discharge, otalgia, limitation of mouth opening, or other symptoms. A clear diagnosis by defining the scope of the lesions, analysis of the transmission route of the lesions, and standard conservative treatment, local drainage, and surgical resection, if necessary, are recommended for patients with suppurative temporomandibular arthritis.
Keywords
Introduction
Suppurative temporomandibular arthritis is a serious infectious disease of the joints that can cause systemic sepsis or septicemia. Local joint infection can lead to osteoarthropathy and is also a cause of ankylosis. Suppurative temporomandibular arthritis has a low clinical incidence, approximately 1 in 10,000 individuals. 1 Its symptoms include preauricular pain, swelling, masticatory pain, and occlusal limitation. 2 A common cause is adjacent or distant tissue infection and trauma. Few studies have reported its clinical treatment and follow-up findings. Herein, we report a rare case of suppurative temporomandibular arthritis caused by chronic suppurative otitis media, its diagnosis, and etiology, followed by surgical resection of the temporomandibular joint after open mastoidectomy under a microscope, resection of temporomandibular joint lesions under ear endoscopy, and the 3-month follow-up findings.
Patient and Methods
History of Present Illness
A 69-year-old man presented with pain and purulent flow in the right auditory canal along with hearing loss for 3 months. As he had not received any standard treatment, he started experiencing gradual ear discharge and preauricular pain. He received radiation therapy at the right temporomandibular joint, teeth, parotid area, and right neck. There was no limitation of mouth opening, dizziness, nausea, or vomiting. Treatment with anti-inflammatory drugs showed no effect. The patient had undergone resection and drainage of granulation tissue in his external auditory canal under general anesthesia at an external hospital. However, his symptoms had failed to improve after the procedure, and the pain in the preauricular canal and temporomandibular joint had worsened, accompanied by a mouth opening limitation of 1°. The patient experienced no improvement in his right ear pain and right facial pain for >6 months, leading to his presentation to our department. Subsequently, he was diagnosed as having suppurative temporomandibular arthritis caused by chronic suppurative otitis media of the right ear, and was admitted to our hospital.
Previous History
The patient had a history of diabetes mellitus for >10 years, with unstable pharmacological control of blood sugar levels in recent years, and chronic suppurative otitis media for >20 years, with no other diseases.
Physical Examination
Specialist examination revealed swelling of the right maxillofacial region, purulent secretion from the right external auditory canal, pus in the external auditory canal, granulation tissue in the anterior and inferior wall of the external auditory canal, and a fistula at the attachment of the granulation tissue. When the probe was extended into the temporomandibular joint cavity, a small amount of pus flowed out in the direction of the tense part of the tympanic membrane. The purulent secretion from the external auditory canal was sent for bacterial culture and drug sensitivity testing. Staphylococcus aureus was detected after 3 days of culturing. Ceftriaxone injection was selected based on the drug sensitivity results. The inflammatory granulation tissue in the external auditory canal was accompanied by calcification.
Auxiliary Examination
An audiogram revealed that the right ear had mixed deafness (Figure 1A). Preoperative ear endoscopy suggested a defective anterior superior wall of the external auditory canal, with protruded granulation tissue. A large amount of purulent secretion was observed after resection of the granulation tissue, and the tympanic membrane was intact (Figure 1B). Computed tomography (CT) of the temporal bone (Figure 1C) revealed that the temporomandibular joint was destroyed and the scope of the lesion was more extensive than before. Maxillofacial enhanced CT (Figure 1D) showed that the right temporomandibular space was blurred and had partially disappeared, and the tissue around the right temporomandibular joint was thickened and swollen with a blurred edge; an enhanced scan showed obvious enhancement. The right pharyngeal recess had become shallow and had slightly swollen near the occipital eustachian tube, medial pterygoid muscle, and lateral pterygoid muscle. Maxillofacial enhanced magnetic resonance imaging (MRI) (Figure 1E) revealed widening of the right temporomandibular joint space and abnormal signal in the right medial pterygoid muscle, lateral pterygoid muscle, and temporal muscle, suggestive of infection and right mastoiditis.
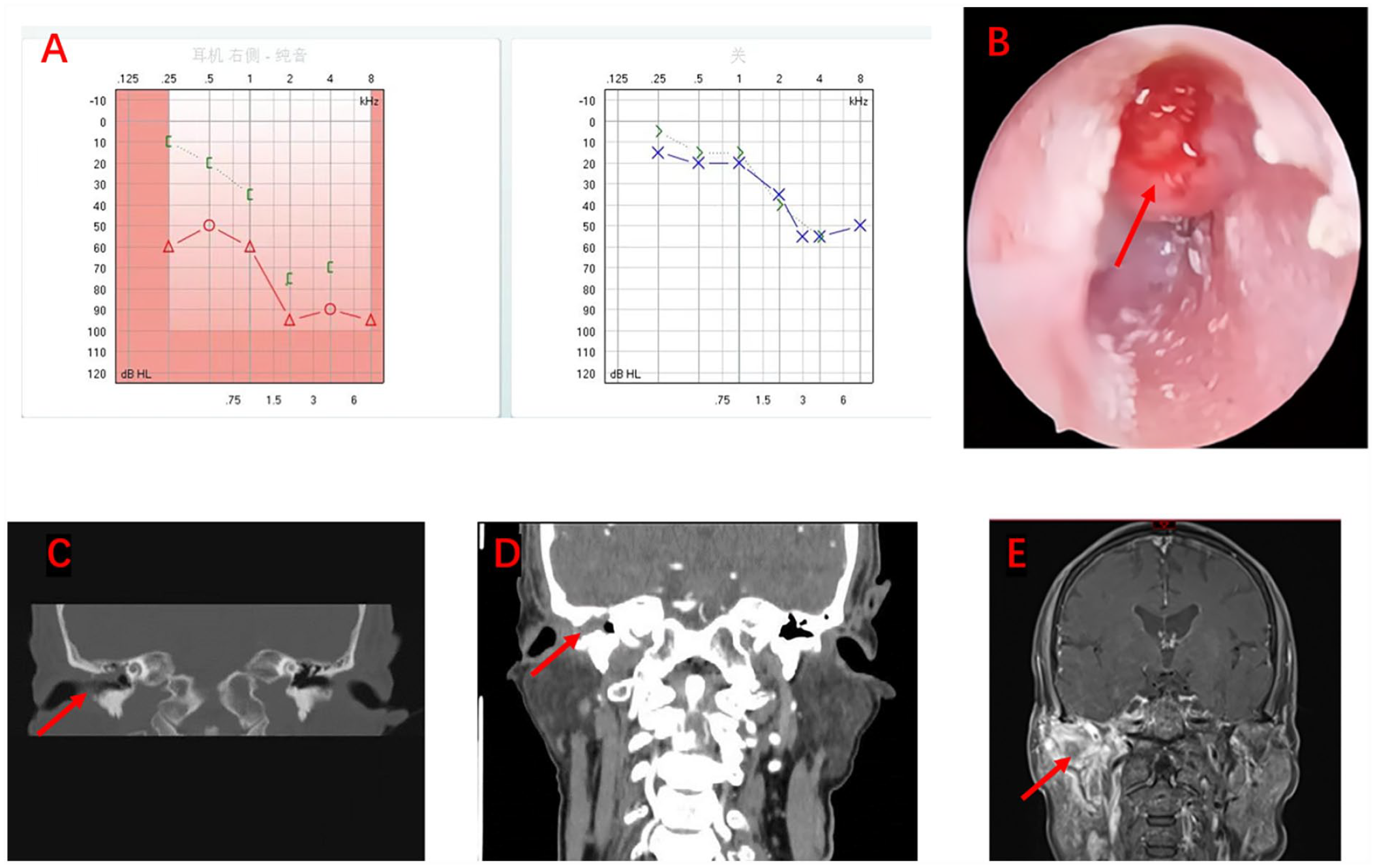
(A) Graphs of preoperative audiogram; (B) Photograph of preoperative ear endoscopy; (C & D) Preoperative temporal bone computed tomography shows the auditory ossicular chain surrounded by a soft-tissue-density shadow and a bone fissure in the lateral wall of the superior tympanum (red arrow); (E) Preoperative magnetic resonance imaging shows the right temporomandibular joint disc with thickening; the articular fossa shows an abnormal arc signal. The right parotid gland, medial pterygoid muscle, lateral pterygoid muscle, and temporal muscle are swollen. The adjacent masseter space and parapharyngeal space are blurred. The right pharyngeal recess appears shallow.
Results
On the basis of the examination results, the treatment plan for the patient on admission consisted of the following steps:
Adjustment of medication to control blood sugar levels.
Local cleaning with 3% hydrogen peroxide, normal saline, gentamicin 80,000 U, and dexamethasone 5 mg, and rinsing of the external auditory canal twice a day.
Culturing of local secretions.
Intravenous administration of third-generation cephalosporin.
Symptomatic treatment with temporary intravenous medication for pain.
However, the ear pain and ear discharge of the patient failed to improve even after treatment for 7 days.
The patient underwent open mastoidectomy of the right ear, tympanoplasty, otoplasty, facial nerve decompression, and coarctation of the mastoid cavity following Schaumburg incision of the right ear plus extended incision in the direction of the tragus temporomandibular joint, and full exposure of the external auditory canal and mastoid cortex. Granulation in the anterior wall of the external auditory canal was cleaned, and perforation of the tense part (pretense) of the tympanic membrane and a small purulent mass were detected. Open radical mastoidectomy was performed to clean the lesions in the mastoid process, tympanic sinus, and tympanic cavity, partially destroying the auditory ossicles and preserving the stapes. The sinus was ground along the bone destruction site in the anterior wall of the external auditory canal. Endoscopic partial resection of the temporomandibular joint was performed to explore the temporomandibular joint fossa under an endoscope, followed by extensive cleaning of purulent secretions and granulation, along with reduction of the tissue in the joint fossa. The mastoid cavity was narrowed using normal bone powder, the surface was covered with fascia tissue, the tympanic membrane perforation was repaired, the spare fascia was used to cover the tympanic cavity and mastoid surface, and the plasty of cavity of auricular concha. Postoperative pathology revealed that the tissues of the upper tympanum and temporomandibular joint showed acute and chronic inflammation, accompanied by vascular and fibrous tissue hyperplasia.
After the patient’s wound was dressed with an antimicrobial gauze, followed by suturing of the incision, he was administered 2 g of ceftriaxone and 100 mL of 0.9% normal saline via an intravenous drip for 7 days, which significantly improved his symptoms, and he was discharged.
After postoperative follow-up (Figures 2A–D), the patient was discharged following 7 days of anti-inflammatory therapy. Pathological examination showed no signs of infection, and antibiotics were discontinued. Eighteen days after the operation, the gauze at the external auditory canal was removed for the first time; no signs of infection, pus, ear pain, or mouth opening disorder were observed, and the patient needed oral analgesics once every 2–3 days. Twenty-eight days after the operation, the patient still reported experiencing occasional tingling in the now dry ear; however, local tenderness at the front of the ear had subsided and local swelling had disappeared, and analgesic drugs were subsequently discontinued.
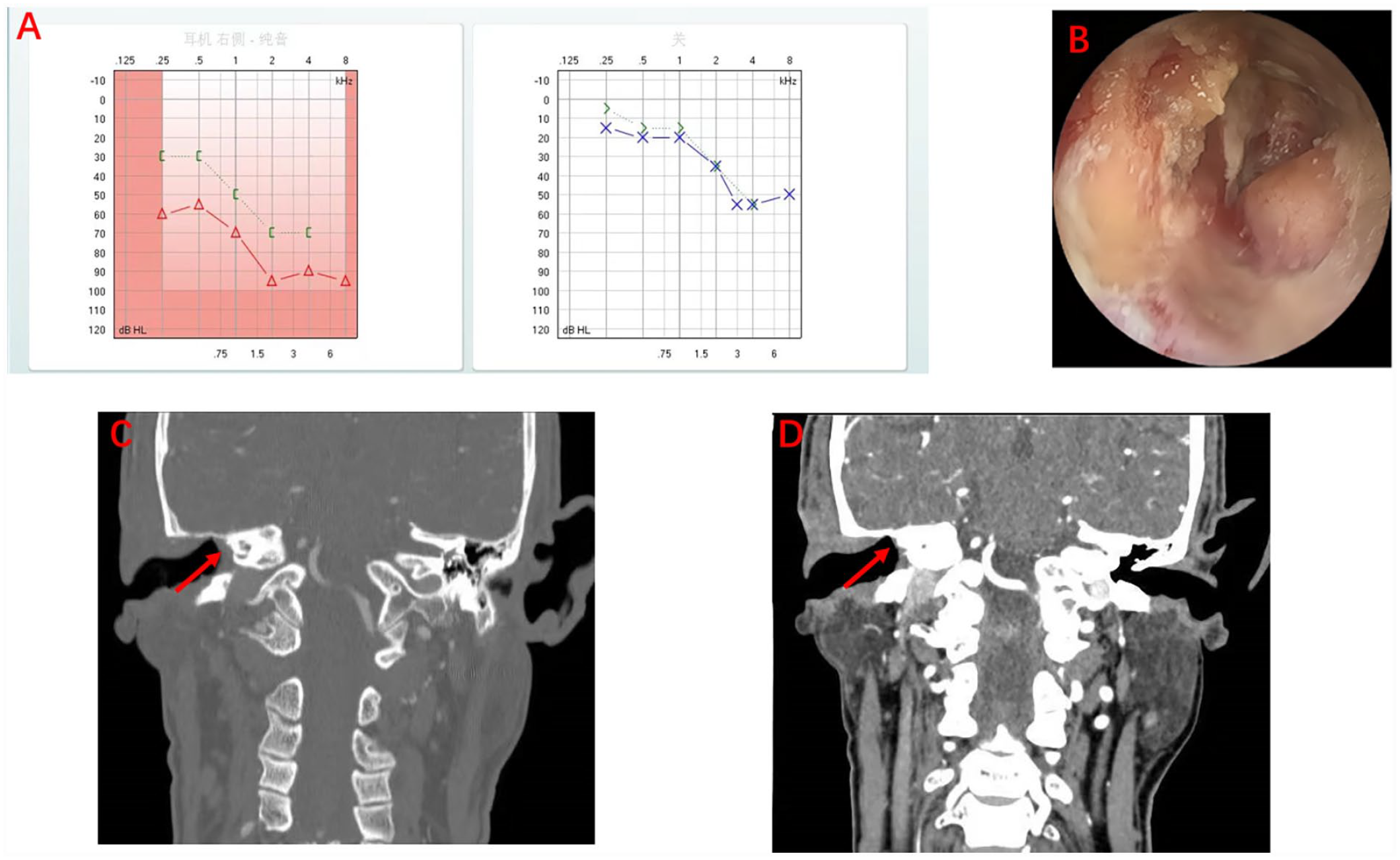
(A) Graphs of postoperative audiogram; (B) Photograph of postoperative ear endoscopy; and (C & D) Preoperative computed tomography shows that the drainage was unobstructed in the direction of the superior tympanum postoperatively (red arrow).
Discussion
Suppurative temporomandibular arthritis is common in children; the most common causative pathogen is S. aureus, followed by Streptococcus spp. and Neisseria gonorrhoeae. 3 In cases of poor control of local infection, the infection spreads to adjacent tissues, such as in cases of acute mumps and masseter space infection. 4 Clinically, suppurative temporomandibular arthritis is occasionally misdiagnosed as lymphadenitis, pharyngitis, retropharyngeal abscess, gingivitis, mastoiditis, mumps, mandibular inflammation, or otitis media. 5 Timely diagnosis and accurate treatment are important to prevent serious complications such as infectious osteomyelitis and ankylosis. Suppurative temporomandibular arthritis caused by chronic suppurative otitis media has rarely been reported.6 -8 Luc et al proposed two possible mechanisms underlying otitis media complicated by temporomandibular arthritis. The first is local spread, because the periosteum of the temporomandibular joint is adjacent to the periosteum of the temporal bone, and the infection spreads through the gap between the bones. The second mechanism is related to the deep auricular artery; as the branches of the deep auricular artery supply the tympanic membrane, external auditory canal, and temporomandibular joint, the infection may originate from blood diffusing through it. 9 Both routes of infection were considered in this patient.
Our patient was 69 years old and had a history of chronic suppurative otitis media for >20 years, diabetes mellitus for >10 years, and unstable blood glucose control for the last few years. Since the onset of disease, only resection of the granulation tissue in the external auditory canal was performed (in an external hospital). The condition of the tympanic membrane was explored and the pus was drained; however, there was no significant change in the postoperative symptoms of the patient. He had a long history of chronic suppurative otitis media, and the infection had spread from the tympanic membrane and external auditory canal along the deep auricular artery to the temporomandibular joint. His blood glucose levels were poorly controlled in recent years and chronic suppurative otitis media was not treated conservatively in time; hence, the inflammation had spread to the temporomandibular joint and the area around the parotid gland after bone breakthrough along the anterior wall of the external auditory canal. The patient was provided with anti-inflammatory treatment at the external hospital. However, his symptoms worsened after the operation, as the mastoid lesions were not cleared and drainage was not performed. The temporomandibular joint was not treated, which resulted in unresolved lesions, purulent ear discharge, and preauricular pain. Preoperative CT of the jaw at our hospital showed a broader lesion range than before, and the temporomandibular joint was damaged.
The first key point in the diagnosis of suppurative temporomandibular arthritis is the medical history of the patient, such as a history of tissue aggravation around the temporomandibular joint and systemic diseases such as diabetes mellitus and hypertension. The second point of diagnosis is symptoms such as persistent pain in the front of the ear and limitation of mouth opening. The third point is imaging examinations such as CT and MRI, which are also important for the diagnosis of temporal suppurative temporomandibular arthritis. 10 CT of the jaw is effective to examine the bone structure and any changes such as bone erosion and subchondral cysts. Enhanced CT of the jaw is recommended for the evaluation of infectious temporomandibular joint arthritis, because it can reveal the presence of inflamed soft tissue and fluid and evaluate adjacent clinically related structures, to determine the presence of concurrent myositis and osteomyelitis. 11 Although the radiological criteria for temporomandibular arthritis are not clearly defined, studies on temporomandibular arthritis have described temporomandibular joint effusion, mandibular bone erosion, significantly widened joint space, and masticatory muscle effusion. 8
Owing to a history of surgery and a long-term history of anti-inflammatory treatment, our patient underwent MRI, which revealed good resolution of articular effusion, accumulation of purulent substances, articular surface, peri-articular soft tissue, and adjacent structures. After the patient was hospitalized, local secretions were sent for inspection and cultured, revealing the presence of S. aureus. Subsequently, the patient was prescribed suitable antibiotics.
Few cases of suppurative temporomandibular arthritis with otitis media have been reported in the literature, and there is no clear consensus on its treatment, which involves surgical drainage and surgery. Surgical drainage includes needle aspiration, low-pressure joint puncture, and arthrotomy. Surgical treatment should be considered when drainage and anti-infection treatments are ineffective. For patients with suppurative temporomandibular arthritis with otitis media, temporomandibular joint surgery can be performed simultaneously with mastoid surgery. This surgery can be planned with the cooperation of otolaryngologists and maxillofacial surgeons. The purpose of temporomandibular joint drainage is to reduce pain and remove inflammatory mediators, avoiding conglutination and bone destruction caused by pus. 12
In the present case, ear endoscopy revealed bone destruction in the anterior wall of the ear canal, protruding granulation, and outflow of purulent secretions after cleaning the granulation tissue; the secretions were sampled for biopsy, and targeted anti-inflammatory treatment was provided.
Careful attention should also be paid to the use of antibiotics in the treatment of suppurative temporomandibular arthritis. 13
Conclusion
Suppurative temporomandibular arthritis caused by chronic suppurative otitis media is a rare disease that can easily be misdiagnosed. When a patient has a history of otitis media, water and pus in the ear canal, pain and swelling of the temporomandibular joint, and limitation of mouth opening, enhanced CT and MRI of the temporomandibular region should be considered first. Destruction of the middle ear and mastoid, widening of the temporomandibular joint space, blurred edge, obvious enhancement of enhanced scan, and abnormal signal shadow of surrounding tissues should prompt consideration of suppurative temporomandibular arthritis. Surgical treatment can be considered when local medication and targeted anti-inflammatory treatment are ineffective. Joint participation of multiple departments, including radiology and stomatology, can help achieve good clinical results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Grant Number and Data Availability statements
The data that support the findings of this study are available from the corresponding author upon reasonable request.