
Abstract
Introduction
Illumination is a vital component of safe, high-quality surgery. 1 Surgical advancements have paralleled improvements in lighting, and surgery in the oral cavity is no exception. 2 Typically, illumination includes ambient light, overhead positional spotlights, headlight, and fiber optic light. 3 However, overhead lights have been shown to require frequent adjustments (eg, every 7.5 minutes), which can interrupt operating room staff activities. 4 Overhead lights may also not be best suited for visualization of deep wounds, 4 as the surgeon’s and assistant’s heads may interfere and cause shadows when relying on overhead lights. Headlights are often blocked primarily by surgeons’ hands, as well as instruments and cautery devices, potentially causing the wearer to repeatedly adjust their head and/or neck position. Use of headlights may result in discomfort and musculoskeletal issues over the long term. 5 Whether the headlight is sufficiently sanitary has also been examined. 6
Due to these issues, the ability to illuminate the surgical site from within a cavity is of particular interest. 4 Various other electric bulb technologies and fiber optic systems offer a way to illuminate at or within the oral cavity, but these have not previously received widespread use when incorporated into the surgical field due to excessive heat generation, 7 poor illumination quality, 4 construction from glass which poses a hazard if broken, and the necessity of managing bulky and potentially obstructing cables and additional light sources. 7 White light-emitting diode (LED) technology offers a solution to these problems 8,9 and has led to LED-based surgical instruments and tools. 10 Untethered LED surgical illumination has been previously described 8 and is commercially available. 10,11 Until recently, LED lights were too large for intracavitary illumination; however, existing lights are now of a suitable size and brightness to be tested in this clinical situation.
The primary objective of this pilot project is to demonstrate the viability, quality, and safety advantages of utilizing sterile LED illumination technology during surgery in the oral cavity and pharynx. The senior author on this study has worked jointly with surgeons in other specialties to solve their illumination challenges, and as such was familiar with off-the-shelf generic lighting devices that may show usefulness in otolaryngology. We sought to determine whether the current embodiment of LED illumination, designed for an alternative surgical situation but lending itself to this circumstance, could illuminate the oropharynx and nasopharynx as well as or better than illumination coming from an external source—such as with a headlight—when performing tonsillectomy and adenoidectomy.
Methods
Participants and Procedures
We offered individuals involved with tonsillectomies at a children’s hospital and a community multispecialty hospital, including study investigators and any residents and surgical staff, the opportunity to participate. This study was reviewed and approved by the IRBs of both institutions (children’s hospital: University of Louisville, study #17.0475; community multispecialty hospital: Billings Hospital IRB, study #16.18) as one of minimal risk. As no protected health information was collected, consent preambles were utilized. Patients were eligible if they were undergoing tonsillectomy with or without adenoidectomy. Consecutive cases were included; in other words, to mitigate investigator bias, cases were not preselected based on factors that could impact results, such as patient age, oropharyngeal anatomy, or comorbidities. We targeted pediatric cases for patients of ages 3 to 18 years to allow for the full range of mouth gag sizes for use with the LED light device. Data were collected over a period of 18 months on days when study personnel were available to coordinate survey data collection. Immediately following each procedure, surgeons, residents, and scrub nurses completed the questionnaires to assess their experiences on the need to use supplemental lighting during the case, mouth gag and LED light placement and insertion, whether any barriers or advantages were identified, and their general impressions on the use of LED lighting in addition to their general impressions on the use of headlights. We asked surgeons to provide their general observations regarding the use of the LED light for each case or in the context of prior cases, and asked scrub techs for general observations about each case. Questionnaires were completed in the presence of study staff who were overseeing data collection, but not in the presence of the principal investigator.
Materials
We piloted the use of an FDA-approved, commercially available LED light. This specific device is marketed for utilization in neuro-spine cases and is pre-bent to fit into a specific retractor. These and similarly derived lights are used in orthopedic, urogynecological, and general surgery cases. Lights were sourced from eMedsco (Phillipsburg, NJ, USA) using their standard Scintillant production run which is designed to provide light of consistent intensity for up to 4 hours. The LED light was held in position with a standard stainless-steel Crowe–Davis mouth gag with minimal modification (Figure 1). The gag was professionally modified by adding two 5 mm metal guides to accommodate and direct the LED light heads. The decision to mount the LED light attachment guides so that they are in a fixed position was made to ensure the simplicity of use. The validity of this assumption was pretested in a mock oral cavity positioning and inspection of the coverage of the surgical field for the extremes of mouth gag sizes. The final positioning of the LED light attachment guides was made based on this preliminary exercise. Gags were insulated using standard powder coating for tonsil gag by Olsen Medical (Louisville, KY, USA).
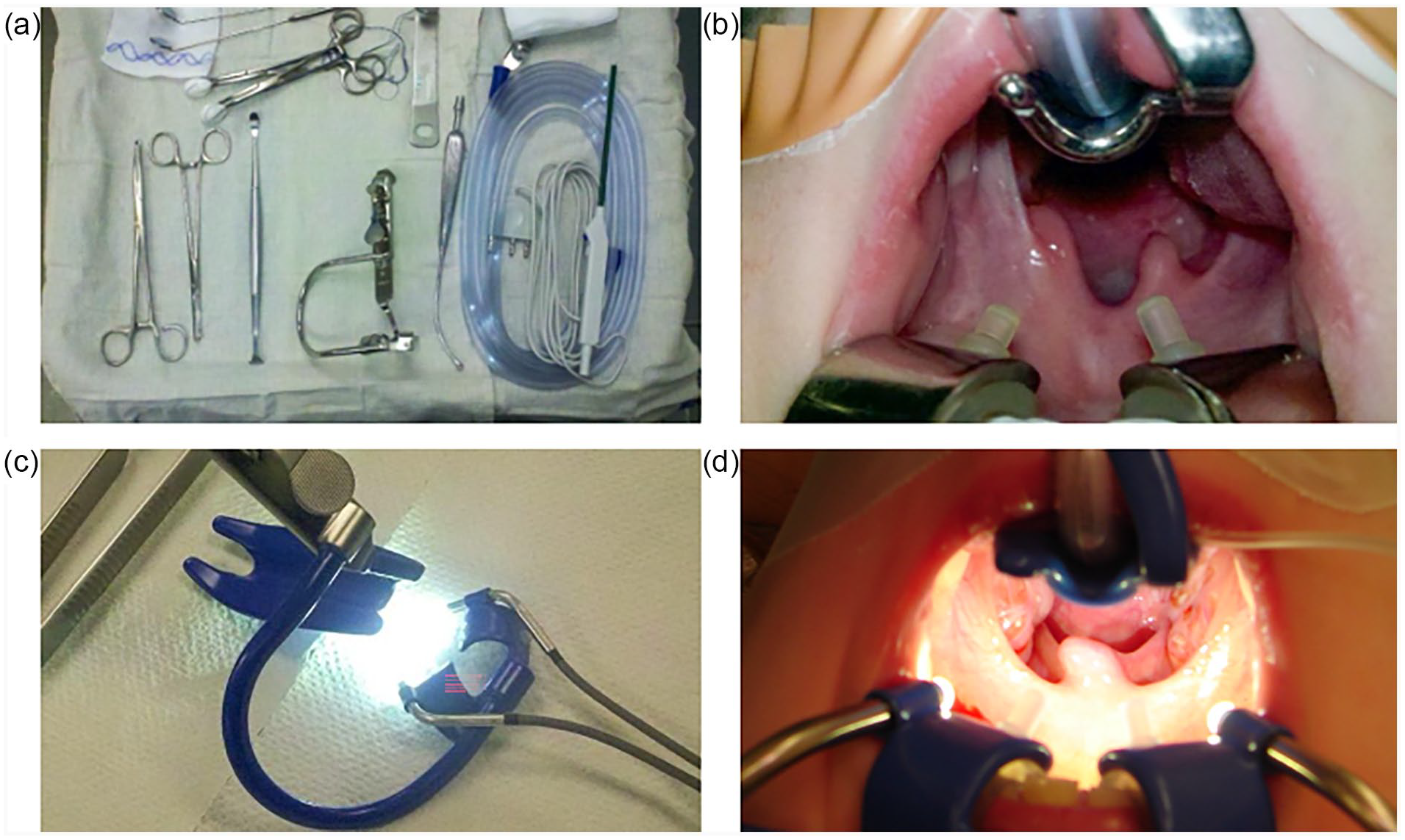
Comparison of standard setup (a, b) to Crowe–Davis gag with LED light guides and illumination in place (c, d) for tonsillectomy/adenoidectomy.
Results
A total of 48 surveys were completed evaluating the use of the LED light for 30 surgical cases: 17 surveys were completed at the children’s hospital and 31 at the community multispecialty hospital. A survey was completed by either an attending surgeon or resident for all 30 cases. Scrub nurses provided survey responses for 18 of the 30 cases performed.
Among attending surgeons or residents, all reported normally wearing a headlight, and 93.3% endorsed that not wearing a headlight would be a favorable option for them. Some (31.6%) endorsed concerns about the cleanliness of headlights used in the OR in general. Prior to the start of the procedure, about half of 53.3% reported using supplemental lighting as the initial source of illumination for the case (ie, while the LED light and mouth gag were prepared and inserted); 60.7% of the time this was via overhead or room lights versus the use of a headlight. The preferred order of application was to attach the LED light to the modified mouth gag, turn on the LED light, insert the mouth gag, and then expand the gag.
During 53.3% of cases, a headlight was eventually utilized, due to a small oral cavity or large tonsillar pillars creating a shadow. However, it was observed by chance that these shadows were almost entirely alleviated by turning down room or overhead lights to enhance visualization of the nasopharynx, and so this suggestion was made during subsequent cases when shadows were created (20.7% of cases performed). Most of the time (79.3%), room or overhead lights did not need to be dimmed to enhance view. In 2 cases, after the LED light device was placed, the headlight was removed and not replaced for the duration of the case.
Many (66.7%) of respondents identified some barrier or disadvantage to use. Primarily, this was the inability to adjust either brightness or exact direction of the light. On the other hand, due to mounting the LED light just back from the immediate working field, spatters were not an issue, and there was no need to clean the light during the procedure. No harms or adverse events were experienced with the use of the light. Some (28.6%) respondents also noted advantages when using the LED light, including superior brightness, stability and consistency of illumination during the tonsillectomy portion of the procedures, and the ability to assist (both attending as an observer and scrub nurses) more quickly without needing the surgeon to specifically adjust their headlight.
Scrub nurses identified no barriers to use of the LED light. Most of the time (66.7%) the LED light was rated as easy to place. Most scrub nurses (88.9%) reported no desire to wear a headlight, and 25% endorsed at least some concerns about the cleanliness of headlights.
Discussion
LEDs are increasingly being deployed in a variety of situations, though research on their use in the operating room has been investigated relatively infrequently. 7 Here we demonstrate the utility of existing LED lighting technology applied in a novel manner to routine pharyngeal procedures. The LED lighting technology was perceived as safe, though some issues with visualization were experienced in a subset of cases.
A major perceived advantage to use of the LED light devices during tonsillectomy was that the device allowed supervising attending physicians to continuously view the surgical wound whether the resident was gazing there or not. Having the lighting fixed on the surgical field enhances safety, allowing for supervision and even intervention—quick or otherwise—should it be required. There may be considerable potential for this technology to change how surgeons work, and how well they are able to interact with their surgical team when illumination comes from the opening or within the wound. 12 This alternative complementary illumination technology would free the surgeon, assistant(s), and surgical scrub team from the myriad limitations encountered when relying on overhead, headlight, and fiber optic light sources.
The LED light device and minimally modified Crowe–Davis mouth gag were found to be suitable for use with patients of a variety of ages and sizes. The current configuration holds the lights in a fixed angle but prevents minor adjustments to give the best reflection angle for some patient anatomy via a mirror into the nasopharynx. Mounting the light on the gag frame back from the immediate working field prevents impairment of the light from spatters and the need to be cleaned during the procedure. Due to the ability to quickly intervene when needed, safety may potentially be increased by having fixed lighting near the surgical field. We observed no mechanical interference in procedures performed with the lights in place.
Illumination is often an issue for assistants and surgical scrub technicians. This is most apparent when the surgeon wears a headlight. When the surgeon gazes away from the surgical wound the light follows their gaze, removing it from the wound. During this time the assistant cannot adequately visualize the surgical wound unless the assistant or scrub technician is also wearing a headlight. Though a common practice, when pointed out to assistants they will immediately acknowledge that this is a limitation of headlight use in many situations, specifically in this research situation. Scrub nurses and surgical techs overwhelmingly commented that the LED light device offered an advantage for their ability to see when the surgeon was looking away.
LED lighting technology offers several additional advantages over the use of headlights. Foremost, headlights often do not supply light at the optimum angle for visualization.
The closer the light is emitted to the visual target, that is, the immediate visual target of the surgeon, the easier it is to have the light come from an angle. This angle off the line of sight helps delineate tissue texture and its subtle features. 12 It also prevents direct reflection back into the surgeon’s eyes. Placing a very small, high-intensity light source into or on the edge of the surgical cavity or wound allows manipulation of the above-mentioned parameters and creates a new opportunity to achieve improved and, perhaps, optimal visualization. 13
The ability to direct light to the desired area with a headlight is not as simple as it might seem. Often the best angle to direct the light may change, necessitating the surgeon to manipulate the angle of the light. The simplest models require the surgeon to “crane” or bend their neck. 5 For some surgeons, among them otolaryngologists, who may wear a headlight in every case and who may do in excess of 10 such cases in a day, totaling many hours, this has an adverse effect. 14 This ranges from causing a headache, creating “distractibility,” and inducing neck, shoulder, and back pain. 15 Surgeons had to be treated for musculoskeletal strain and cervical spine issues due to neck craning from headlight use. 16 Over time this can lead to missed work due to physical symptoms. 14 The full extent of this issue is likely under-recognized.
In other situations, surgeons or their proxies may be required to manipulate the non-sterile light leading to a variety of potential sources for contamination. Headlights are a fomite and often hard to completely clean. 17 They have a variety of mechanical knobs and surfaces, and their cords often come into contact with many non-sterile surfaces including the ground. 3 Headlights are often shared, leading dirt and skin oils to accumulate in the fine cracks and grooves of the device.
Finally, headlights are also relatively expensive, large, and somewhat cumbersome, making purchase and storage secondary factors. Searching for headlights, and light boxes also consumes a measurable amount of time by those who organize them for the surgeon, and sometimes the surgeon themselves. There is a cost for this time, although it is not generally accounted for as a specific line item for a given surgery. Our data suggest that the use of near-field lighting has the potential to at least partially mitigate some of these problems.
There were some limitations observed with the use of the LED lighting technology. We employed a single-use, off-the-shelf commercial solution to conduct this pilot study. A reusable device was not engineered as it would have been cost prohibitive for the purposes of this study, but this approach could be considered in future research. In some cases, shadowing at the top of the superior tonsillar pole was noted. However, light in the nasopharynx was improved by turning the room lights down, providing excellent contrast and improving visualization. This issue may have been more difficult to correct with the specific modified mouth gag used in this research. Solutions include mounting additional lights to improve aim into this area. Additional specifications may make the LED light applicable to a wider variety of cases, though no specific patient biometric specifications can be offered due to the relatively small sample size of this study. Additionally, the LED lights are disposable, single-use devices. While this may pose as a limitation to accessibility of the device for some, its usefulness lies in its ability to reduce or potentially eliminate the need for a headlight in ideal cases and could be advantageous in locations where headlights are not available or unable to be used. Of note, other mouth gags—including McIvor and Dingman—can easily be configured to hold the lights. These configurations could be tested in future, larger trials that employ a control group. A new, as yet undefined mouth gag configuration may be the optimum way to take advantage of near-field LED illumination.
This project offers a potential strategy that may serve as a viable supplemental approach to existing illumination which may fill certain niche needs. Individual surgeons may be willing to adopt or reject this technology based on the quality of the illumination and their feelings about headlights. Nursing staff are likely to appreciate the ability to see in the wound so they may safely assist without interruptions in visibility due to fluctuations in gaze by the surgeon. This project may open the possibility of fundable research related to providing illumination during surgical procedures performed in rural or underserved areas of the globe where outreach and medical missions are done, as these low-resource settings have been observed to struggle with safety issues due to poor lighting of the surgical field and inaccessibility of headlights. 18
Conclusions
In this pilot feasibility study, near-field LED lighting technology demonstrated utility to teaching surgeons, residents, and scrub nurses, and was perceived as safe when applied to pediatric tonsillectomy and adenoidectomy procedures. Minor issues experienced were quickly resolved with the brief use of supplemental lighting. Additional specifications may make the LED light applicable to a wider variety of cases and could mitigate the need for fiber optic headlight during procedures of the oral cavity and oropharynx.
Footnotes
Authors’ Note
Meeting information: Poster presentation at AAO-HNSF virtual annual meeting, 13 to 16 September 2020; specialty area: pediatric otolaryngology.
Author Contributions
EC: Design, data acquisition and analysis, drafting the work, review and revision, reviewed final article prior to submission, and accountability of the work. CA: Data acquisition, review and revision, reviewed final article prior to submission, and accountability of the work. KP: Conception, review and revision, reviewed final article prior to submission, and accountability of the work. SC: Conception, data acquisition, review and revision, reviewed final article prior to submission, and accountability of the work. RH: Conception, design, data acquisition, interpretation of data, drafting review and revision, reviewed final article prior to submission, and accountability of the work.
Data Availability
All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. The data are available to anyone for review upon request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RH is a surgeon inventor and jointly owns intellectual property for temperature control in surgical illumination. The off-the-shelf commercial light devices used in this study were purchased from the manufacturer at full price by RH. The manufacturer was not involved at any point in study design, data collection, analysis, interpretation, or dissemination, nor were any restrictions placed regarding publication. RH is also the Chief Medical Officer for LumeNXT where he focuses on strategies to improve surgical visualization. All other authors declare that they have no conflict of interest, financially or otherwise.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.