
Abstract
Spontaneous otogenic pneumocephalus (SOP) is a rare condition. We report a case of SOP that may be related to repeated Valsalva maneuvers. A young woman underwent repeated Valsalva maneuvers to restore Eustachian tube function and subsequently developed symptoms that included otalgia, headache, and nausea. A temporal bone computed tomography scan was performed and a diagnosis of SOP was made. Subsequent surgical treatment was performed and no recurrence was found during the 1-year follow-up period. The rarity of SOP and its potential for misdiagnosis pose significant challenges in clinical practice. The Valsalva maneuver is 1 of the contributing factors to this phenomenon. Otologists should be familiar with the potential complications of the Valsalva maneuver and use it with greater caution.
Case description
A 33-year-old woman was admitted to the hospital with a 1-month history of pain in the right ear, 6 days of headache, and 1 day of rhinorrhea. The patient underwent tympanocentesis for right secretory otitis media at a local hospital 8 months ago and made an uneventful recovery. To restore Eustachian tube function, the patient diligently performed Valsalva maneuvers more than 10 times a day for an extended period of time. One month earlier, the patient experienced sudden onset of pain in their right ear without an identifiable etiology. Six days ago, the otalgia intensified and was accompanied by persistent headaches and nausea. The local hospital initially misdiagnosed it as “acute otitis media” on the right side; however, 1 day ago, clear rhinorrhea developed from the right nostril of the patient. The initial otoscopic examination conducted after the patient’s admission to our medical facility revealed invagination of the tympanic membrane in the right ear and a positive effusion sign. The audiometric evaluation revealed mild conductive hearing loss in the right ear. The complete blood cell analysis determined a white blood cell count of 15.18 × 109/L and a CRP level of 15.01 mg/L. Computed tomography (CT) imaging of the skull and temporal bones (Figure 1) revealed a significant presence of gas within the right temporal region, as well as an irregular and disrupted right tympanic operculum. However, since there was no apparent inflammation in the tympanic compartments of the right middle ear, it is unlikely that pneumocephalus was caused by acute otitis media infection and is more likely to be considered spontaneous pneumocephalus. Magnetic resonance imaging (MRI) of the head (Figure 1) revealed pneumatosis in the right temporal lobe and ventricle, accompanied by localized inflammatory manifestations. After a thorough differential diagnosis, the patient was eventually diagnosed with spontaneous right otogenic pneumocephalus and cerebrospinal fluid rhinorrhea. Therefore, the patient received mannitol to reduce intracranial pressure and ceftriaxone (a third generation cephalosporin) for anti-infective treatment. Despite initial attempts at conservative therapy in the hope of spontaneous absorption of intracranial air lesions, it proved to be ineffective due to the prolonged course of the disease. She underwent surgical intervention to repair a cerebrospinal fluid leak via a right middle cranial fossa approach. A 2 × 2 mm bone defect was found medial to the posterior aspect of the spinous foramen. Bone wax, temporalis fascia, and biological protein adhesive were utilized for the repair of bone defects, the corresponding dura mater, and bone flap, respectively. The patient continued to receive mannitol for intracranial pressure reduction and ceftriaxone for infection treatment postoperatively. After 1 month, the patient achieved complete recovery with gradual resolution of symptoms such as headache and dizziness. After a 1-year follow-up period, no recurrence was observed and imaging revealed satisfactory recovery at the surgical site with complete resolution of the pneumatoid foci (Figure 2).
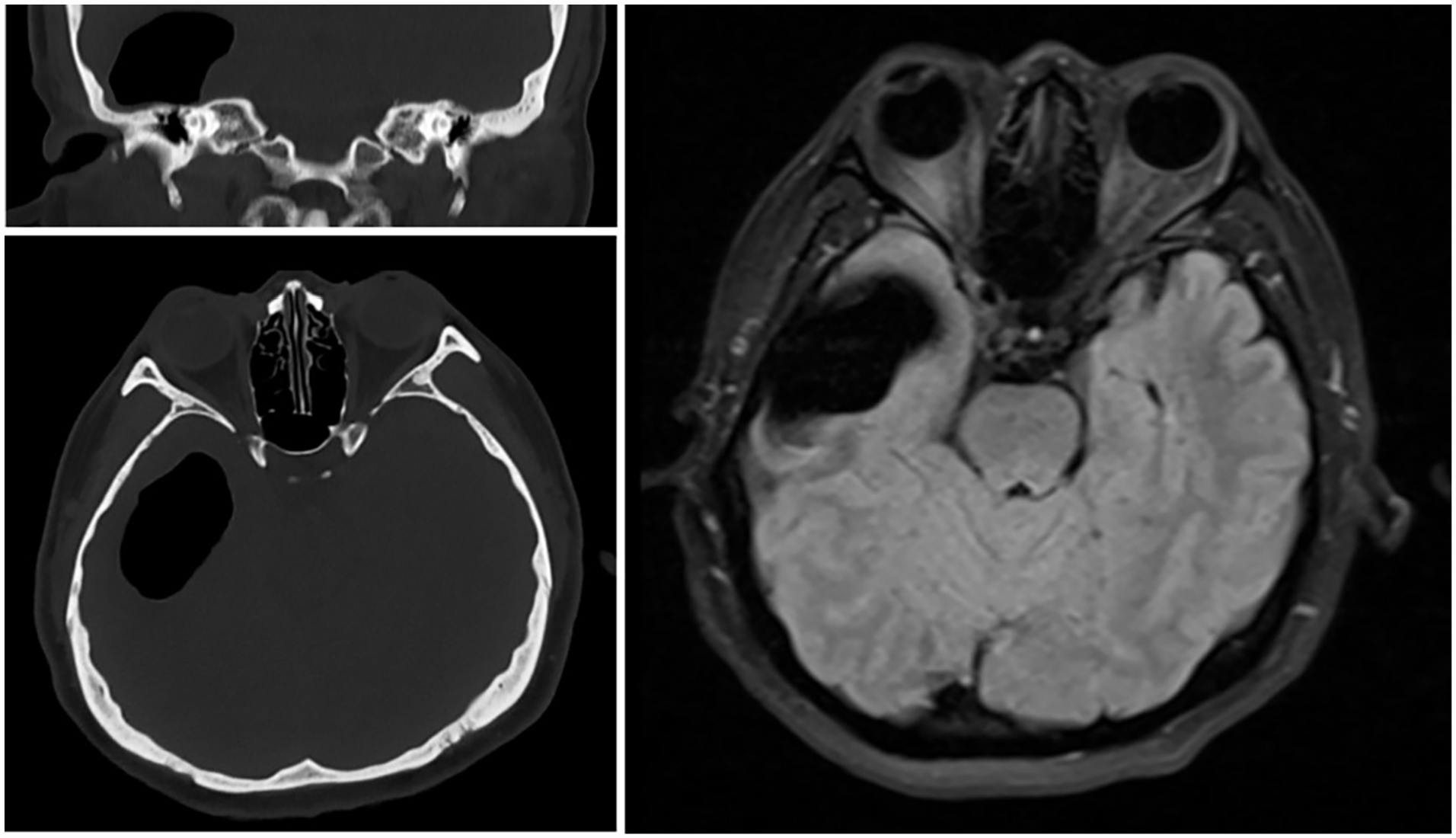
Preoperative imaging. CT scan of the temporal bone showing right tympanum preoperative defect and gas accumulation. CT scan of the brain showing air within the right temporal region, with a maximum diameter of 5.2 × 3.2 cm. Magnetic resonance imaging showing effusion and gas collection in the right temporal lobe. CT, computed tomography.
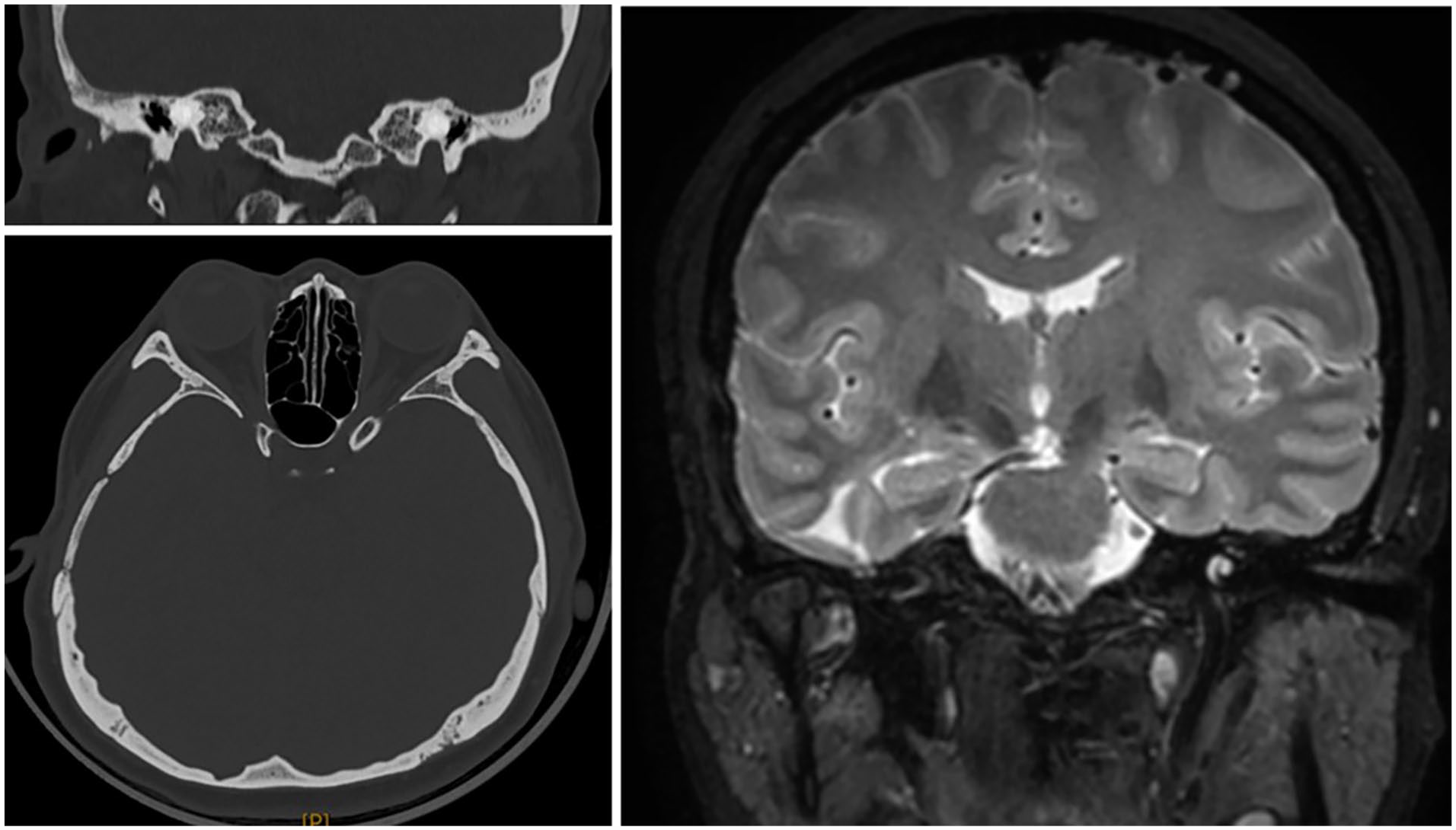
One-year postoperative imaging. CT scan of the temporal bone showing no right tympanum defect and no gas accumulation. CT scan of the brain showing no air in the skull. Magnetic resonance imaging showing no gas collection in the right temporal lobe and a few remaining old softening lesions. CT, computed tomography.
Discussion
As a complication of otitis media, spontaneous otogenic pneumocephalus (SOP) is an exceedingly rare intracranial occurrence. 1 Apart from the current case, only 44 cases have been reported to date, most attributed to barotrauma, exercise-induced, strenuous coughing or the Valsalva maneuver. 2 The precise mechanism of SOP remains elusive. However, based on the patient’s medical history, we postulate that the Valsalva maneuver may have contributed to 2 preconditions for this case: a pressure gradient between the temporal bone and skull, and a defect in the temporal bone that allows air entry through the mastoid process. 3
The Valsalva maneuver, initially proposed by Valsalva in 1704, is a technique that can enhance the Eustachian tube and optimize its function through glottic closure and air retention. However, despite its relative safety profile, this maneuver has been linked to complications such as epidural gas, orbital edema, and intracranial gas; these adverse events are frequently observed in patients who have undergone mastoidectomy or craniotomy or those with orbital tumors. 4 However, the current patient presented symptoms of intracranial pneumatosis, including headache and rhinorrhea of cerebrospinal fluid, after frequent Valsalva maneuvers in the absence of prior brain surgery. The ball valve effect is presumed to be the mechanism behind this condition, which arises from a congenital weakness in the temporal bone and dura, as well as an increase in the middle ear pressure resulting from frequent Valsalva maneuvers. Ultimately, this leads to the destruction of the bone wall and dura, allowing air to enter the intracranial cavity. The initial symptoms of SOP are atypical and involve mainly otologic manifestations, such as ear pressure and hearing loss. As the disease progresses, neurological symptoms may emerge, including headaches, altered mental status, and local neurological dysfunction. A diagnosis of SOP can be established when imaging studies (cranial CT and MRI) reveal pneumocephalus within the cranial cavity along with a temporal bone defect. 5 Due to the rare incidence of SOP, this patient was initially diagnosed with acute otitis media based on similar clinical symptoms at a local hospital. However, despite presenting with otalgia, persistent headache and hearing loss, the possibility of SOP was not considered during his visit and treatment was delayed until brain CT confirmed the correct diagnosis.
The radical treatment of SOP relies on surgery to release intracranial pressure and prevent brain infections. 6 Although conservative treatment and puncture suction can alleviate the symptoms of spontaneous pneumocephalus caused by bone defects, the defect remains, allowing gas to continue to enter the brain and causing disease progression. Therefore, it is crucial to repair the bone defect in the temporal bone and its underlying dural foramen. Myofascial flaps, cartilage, and bone wax are commonly used to effectively seal existing fistulas and prevent communication between the extracranial and intracranial compartments. Conservative treatment was ineffective, so radical surgery was necessary to prevent recurrence.
Conclusion
SOP is a rare clinical condition characterized by nonspecific symptoms, which poses challenges in diagnosis and increases the risk of misdiagnosis. The Valsalva maneuver is 1 known cause of SOP, and otologists should exercise caution when performing this maneuver in patients with recurrent otitis media, particularly during acute inflammation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Characteristics and mechanism of horizontal semicircular canal injury induced by gentamicin in guinea pigs [grant number 2020MSGY078]; Shandong Postdoctoral Innovation Program [grant number SDCX-ZG-202203076]; Natural Science Foundation of Shandong Province [grant number ZR2022QH073]; The Yantai Science and Technology Innovation Development Project [grant number 2022YD009].
Ethical/Consent Statement
Consent was obtained from the patient.