
Abstract
Introduction
Sudden sensorineural hearing loss (SSHL) is a prevalent condition within the field of audiology. It is typically characterized as an abrupt loss of hearing within 72 hours from the onset of symptoms, involving a 30 decibel (dB) reduction across three consecutive test frequencies. 1 The incidence of SSHL has been reported to range from 5 to 160 cases per 100,000 individuals.2,3 Given its high prevalence, swift onset, and rapid progression, this disorder often presents with accompanying symptoms such as tinnitus, nausea, and vertigo, which can severely impact patients’ quality of life. The pathogenesis of SSHL remains elusive, but many researchers postulate that the condition may be linked to factors such as vascular endothelial dysfunction, inadequate blood supply to the inner ear, dyslipidemia, inner ear labyrinth virus infections, and autoimmune diseases.4 -6 Consequently, various treatments have been proposed for SSHL, including corticosteroids, vasodilators, hyperbaric oxygen, and vegetative nerves; however, the efficacy of most SSHL treatments continues to be debated. 1
Although the clinical experience and prognosis of initial treatment for SSHL have been extensively documented, their effectiveness varies.7,8 Patients with SSHL who experience no improvement or only slight improvement after treatment are often advised to accept their hearing loss, with those suffering from severe or very severe condition encouraged to pursue hearing aid interventions. Reports on the value and significance of retreatment for such patients are scarce. Therefore, it is crucial to explore continued treatment for SSHL patients whose initial treatment outcomes are suboptimal, and to examine the therapeutic effect and influencing factors thereof.
Research has demonstrated that exogenous nerve growth factor (NGF) can mitigate the damage caused by noise and ototoxic drugs to cochlear hair cells.9 -11 Han’s study reveals that NGF plays a vital role in the differentiation of cochlear neural stem cells into functional neurons while reducing the ototoxicity of gentamicin. 12 These findings suggest the potential for NGF in the treatment of hearing loss. NGF is known to be a nerve cell growth regulator possessing dual biological functions, acting on vegetative neurons and promoting the growth of processes. It plays a significant role in the regulation of development, regeneration of central and peripheral neurons, and the expression of functional characteristics. NGF has been widely utilized in research investigating the treatment of neurological diseases.
A retrospective analysis was conducted on the data of 101 cases treated with exogenous NGF at Sun Yat-sen Memorial Hospital of Sun Yat-sen University between January 2019 and July 2020. This analysis aimed to assess the therapeutic effect of NGF on SSHL and to further analyze the clinical efficacy of SSHL treatment and the factors influencing prognosis.
Materials and Methods
Inclusion and Exclusion Criteria
A retrospective study was conducted in 101 patients diagnosed with SSHL who received treatment at the Sun Yat-sen Memorial Hospital of Sun Yat-sen University between January 2019 and July 2020. This single-center study included all patients who underwent Pure Tone Audiometry (PTA), auditory brainstem reaction, otoacoustic emission, temporal bone computed tomography (CT), or inner ear magnetic resonance imaging (MRI). Inclusion criteria were as follows: (1) adults over 18 years of age with complete medical records; (2) patients diagnosed with moderate or worser SSHL, characterized by an acute decrease in hearing thresholds ≥20 dB in at least two consecutive frequencies within 72 hours, and hearing loss of adjacent frequencies above 41 dB; (3) patients unresponsive to first-line routine treatment, including systemic use of steroid hormones, microcirculation improvement, and neurotrophic drugs; and (4) patients with type A tympanogram and no evidence of middle ear effusion on endoscopy. Exclusion criteria were: (1) patients with a history of otitis media affecting hearing and (2) sensorineural deafness attributed to other causes, such as Meniere’s disease, autoimmune hearing loss, or space-occupying lesions in the internal auditory canal confirmed by CT or MRI.
Treatment Protocol
The control group received conventional ear therapy 13 : 1 mg/kg of intravenous methylprednisolone for 3 days, followed by a gradual dose reduction based on the patient’s condition; Batroxobin 5-10 BU, administered once every other day, with an initial dose of 10 BU, then 5 BU each time for a total of four times, monitoring fibrinogen (use if fibrinogen is higher than 1 g/L); and daily Ginkgo biloba extract. Methylprednisolone 40 mg combined with 2% lidocaine was injected into the tympanic cavity once every 2 days (patients were placed in a supine position with their head tilted 45° to the opposite side, and the solution was slowly injected under microscopic guidance into the posterior-inferior portion of the tympanic membrane, entering the middle ear space; patients were instructed to remain in this position without swallowing for 30 minutes). Patients experiencing vertigo were given oral betahistine, 12 mg per dose, three times a day. The study group received an additional 9000 U(18ug) of mouse NGF daily for 5 days, based on the control group’s treatment regimen. 14
Classification of Level of Hearing Loss
Hearing loss levels are divided into five degrees according to the World Health Organization method: mild (26-40 dB HL), moderate (41-55 dB HL), moderately severe (56-70 dB HL), severe (71-90 dB HL), and profound (>90 dB HL).
Classification of Audiogram
Audiograms can be categorized into four types 13 : (1) low-frequency type, with hearing loss in low-tone frequencies at least 20 dB HL greater than other frequencies; (2) high-frequency type, with hearing loss in high frequencies at least 20 dB HL greater than other frequencies; (3) flat type, with hearing loss at all frequencies ≤81 dB; and (4) total deafness, with hearing loss of 81 dB HL or higher in all frequencies.
Treatment Outcomes
All patients underwent PTA evaluation, with assessments performed before treatment initiation and at 1 week, 2 weeks, and 1 month post-treatment. For the analysis of hearing improvement, PTA results were evaluated, and an increase in the arithmetic mean of pure tones (final PTA—initial PTA) at impaired frequency was considered: (1) cure: hearing at impaired frequency restored to normal, to the level of the healthy ear, or to the level prior to this disease; (2) obviously effective recovery: affected frequencies at threshold recovery greater than 30 dB HL on average; (3) effective recovery: affected frequencies at threshold recovery greater than 15 dB HL on average; and (4) not effective: affected frequencies at threshold recovery no more than 15 dB HL on average. The overall recovery rate was calculated as (cured number + obviously effective recovery number + effective recovery number)/total number of subjects × 100%. The inefficiency rate was calculated as no effective number/total number of subjects × 100%.
Statistical Analysis
Data were analyzed using SPSS 22.0 software (Chicago, IL, USA), and statistical significance was defined at P < .05. The t-test was used for measurement data, and the chi-square test was used for counting data. Prognostic factors of SSHL were analyzed through univariate and multivariate logistic analyses. Parameters with statistical significance in univariate logistic analysis were included in multivariate logistic analysis.
Results
Patient Characteristics
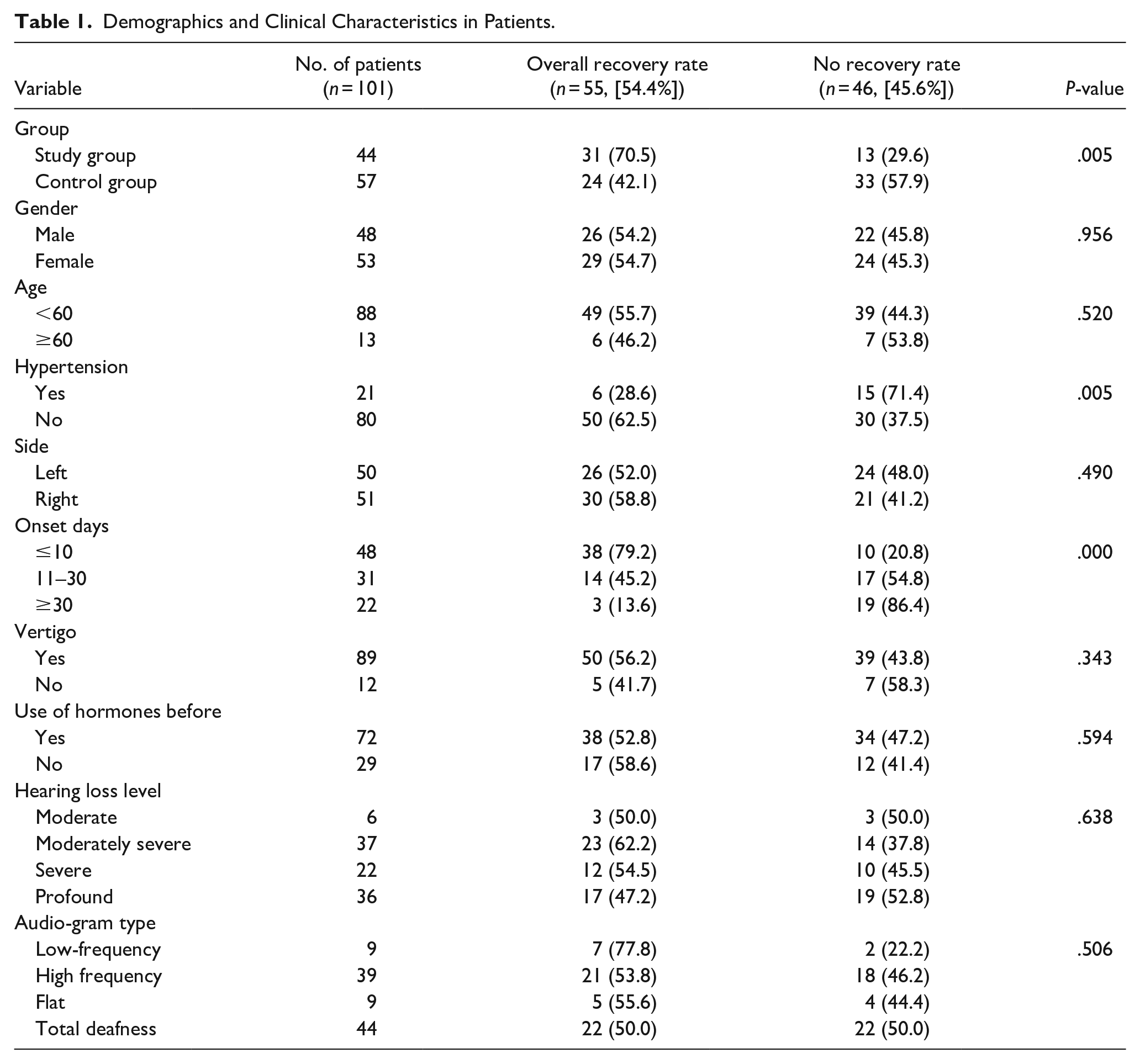
A retrospective study was conducted in 101 patients with SSHL treated at the Sun Yat-sen Memorial Hospital of Sun Yat-sen University between January 2019 and July 2020 (Table 1). Patients’ ages ranged from 19 to 81 years (mean 42.7 ± 1.3 years), with 48 males (47.5%) and 53 females (52.5%). Among these patients, 57 were included in the control group and 44 in the study group.
Demographics and Clinical Characteristics in Patients.
Evaluation of Efficacy
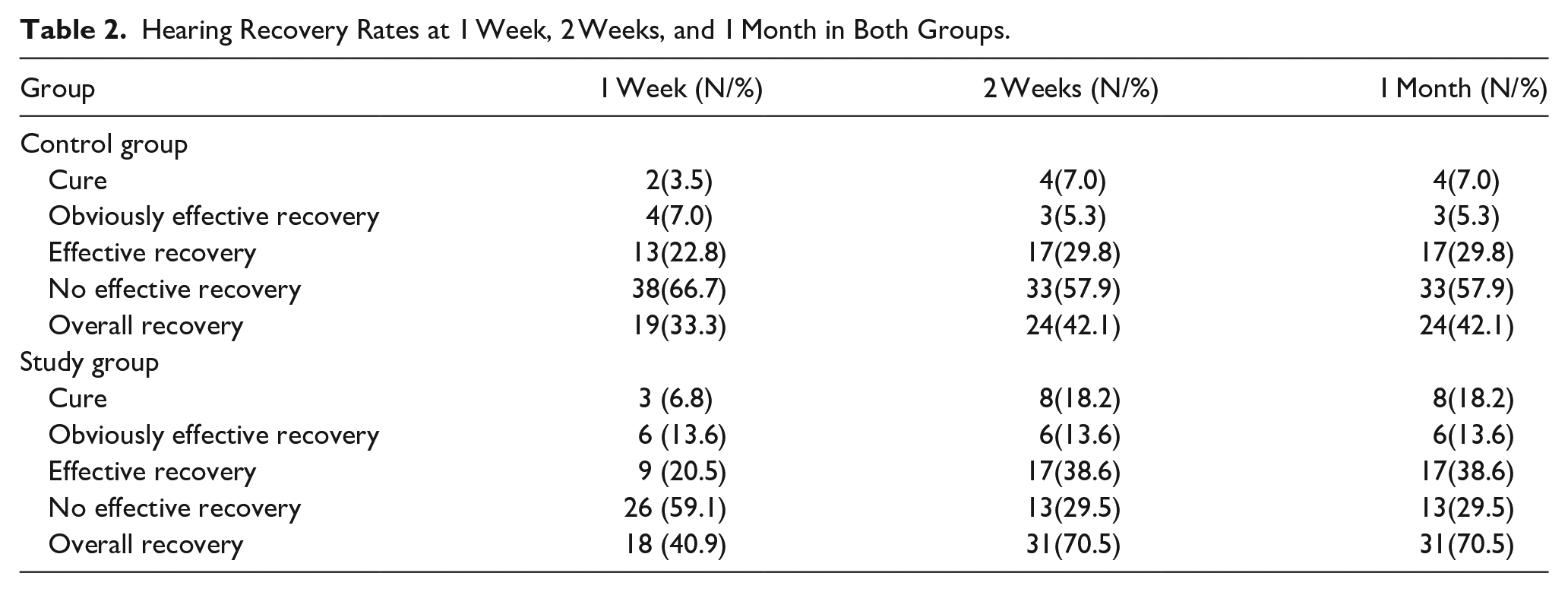
Post-treatment hearing thresholds were significantly reduced in both groups (Figure 1). Additionally, the change in PTA threshold was statistically significant between the two groups (Figure 2). In the study group, 8 (18.2%) of 44 patients exhibited cure, 6 (13.6%) exhibited obviously effective recovery, 17 (38.6%) exhibited effective recovery, and 13 (29.6%) exhibited no effective results (Table 2, Figure 3). (38.6%) exhibited effective recovery, and 13 (29.6%) exhibited no effective results (Table 2, Figure 3). The overall hearing recovery rate was significantly higher in the study group (31/44, 70.5%) than in the control study group (24/57, 42.1%; p < 0.05) (Table 1). Examining all patients, the results demonstrated that effective hearing recovery was most prominent within 1 week after treatment in both the study group (40.9%) and control group (33.3%), although some patients experienced good recovery within 2 weeks (42.1%, 70.5%) (Table 2, Figure 4).
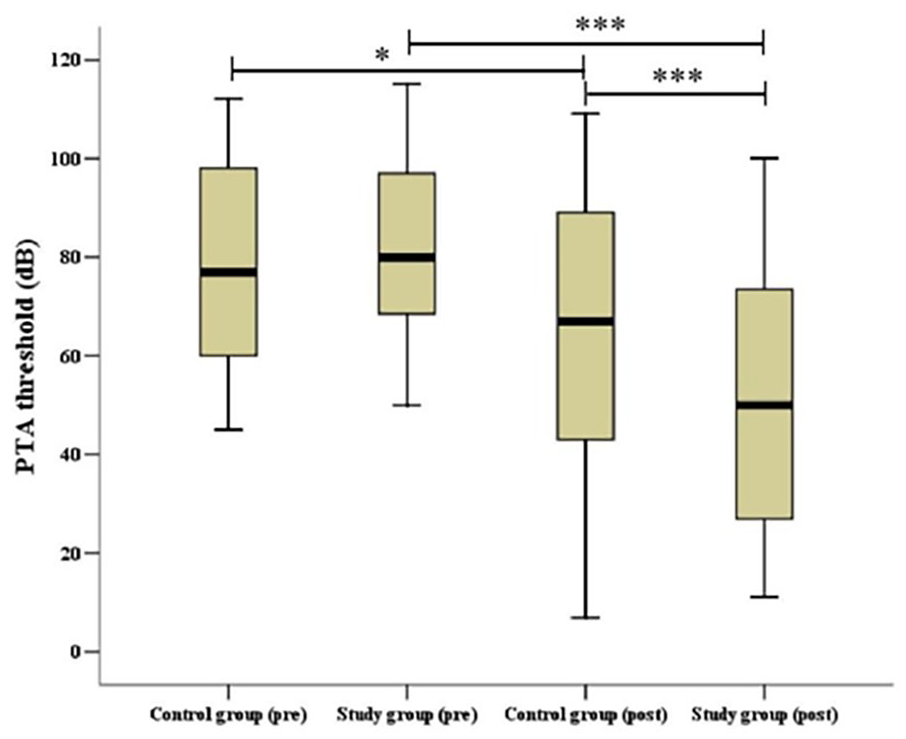
Pre- and post-treatment Pure Tone Audiometry threshold in the two groups.*P < .05, **P < .01, ***P < .001. pre, pretreatment; post, post-treatment.
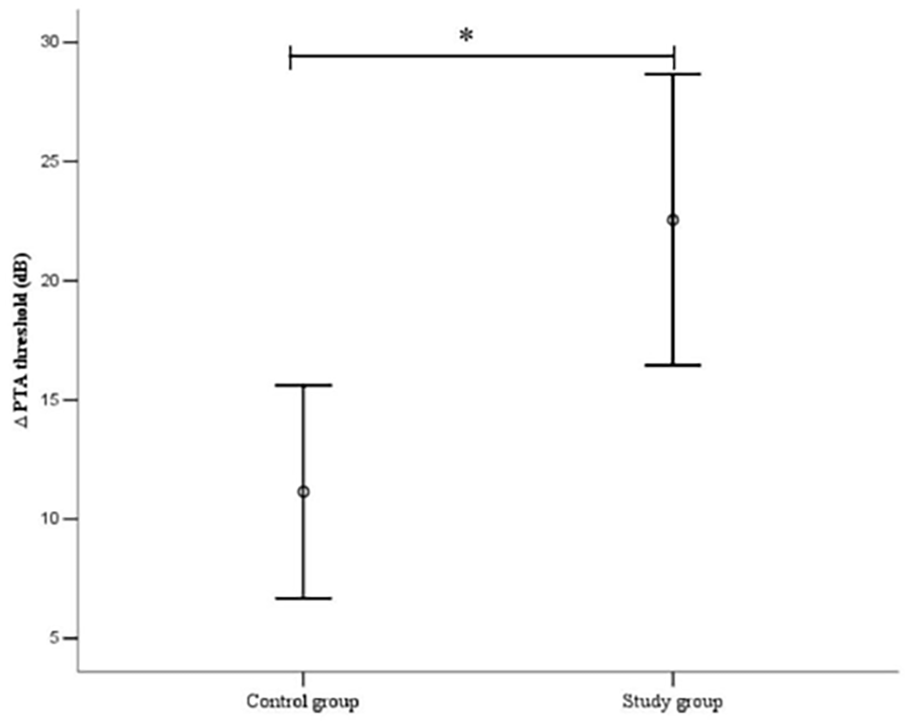
Comparison of change of the Pure Tone Audiometry threshold between the two groups,*P < .05.
Hearing Recovery Rates at 1 Week, 2 Weeks, and 1 Month in Both Groups.
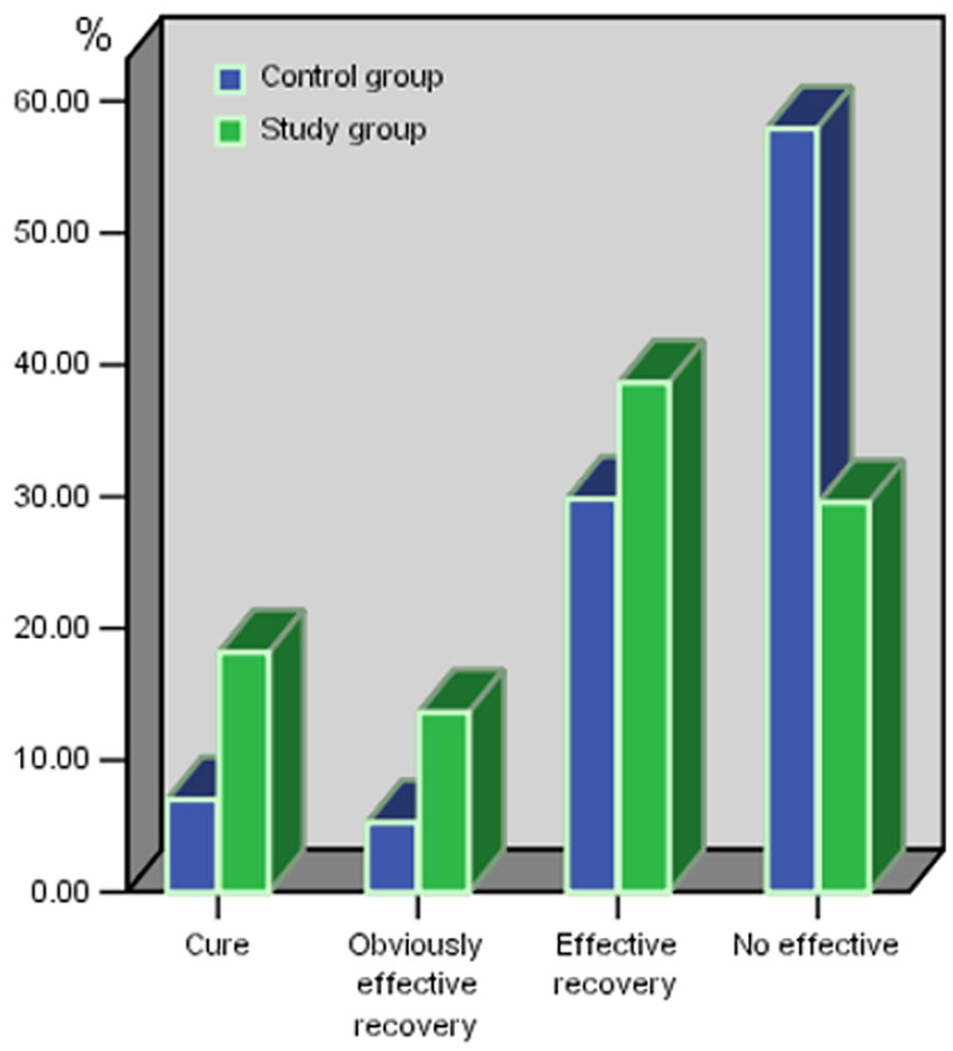
Overall therapeutic outcomes of patients with idiopathic sudden sensorineural hearing loss treated.
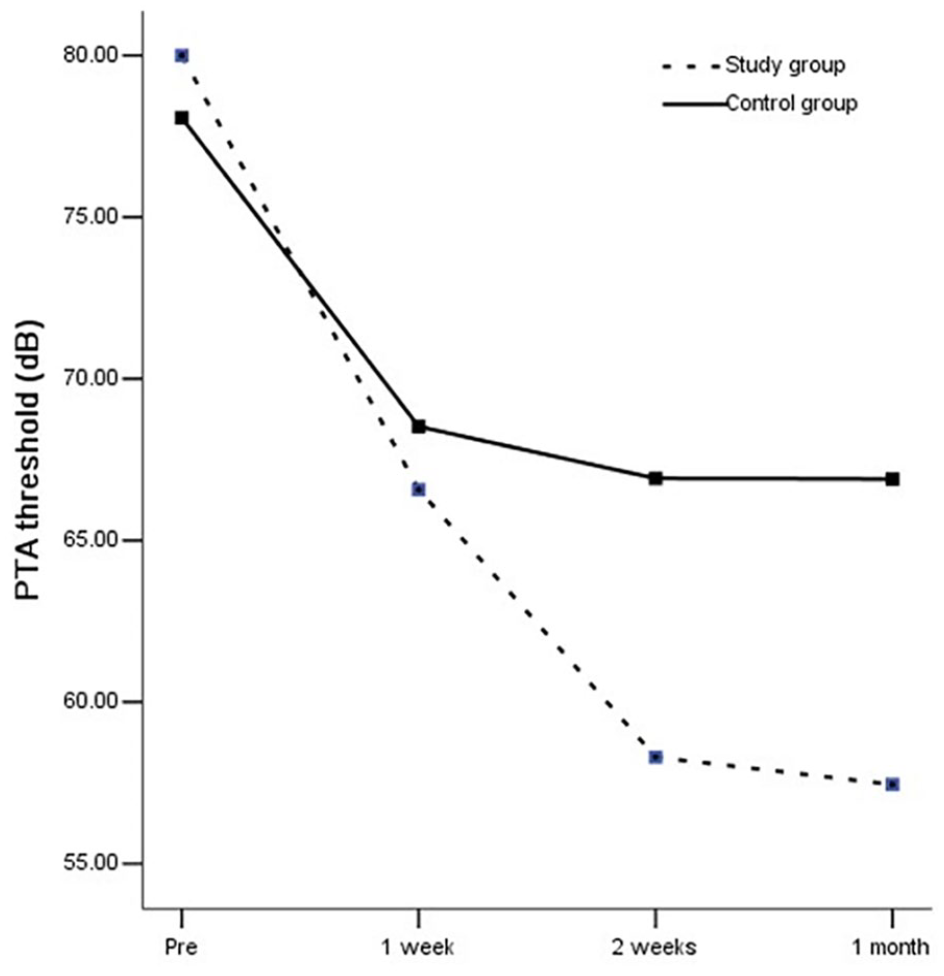
Comparison of change in pure-tone audiometry measurements before treatment and 1 week, 2 weeks and 1 month after the start of treatment by per-protocol analysis.
The Univariate Logistic Regression Analysis of Possible Prognostic Factors
Based on hearing recovery, patients were divided into the complete recovery group and the non-recovery group (Table 3). A univariate binomial logistic regression was performed to analyze 9 variables: NGF; gender; age; hypertension; side; onset days; prior use of hormones; hearing loss level; and audiogram type. According to the analysis, NGF, hypertension, and onset days were identified as independent risk factors for the treatment effect of SSHL (Table 3).
The Univariate Logistic Regression Analysis of Possible Prognostic Factors.
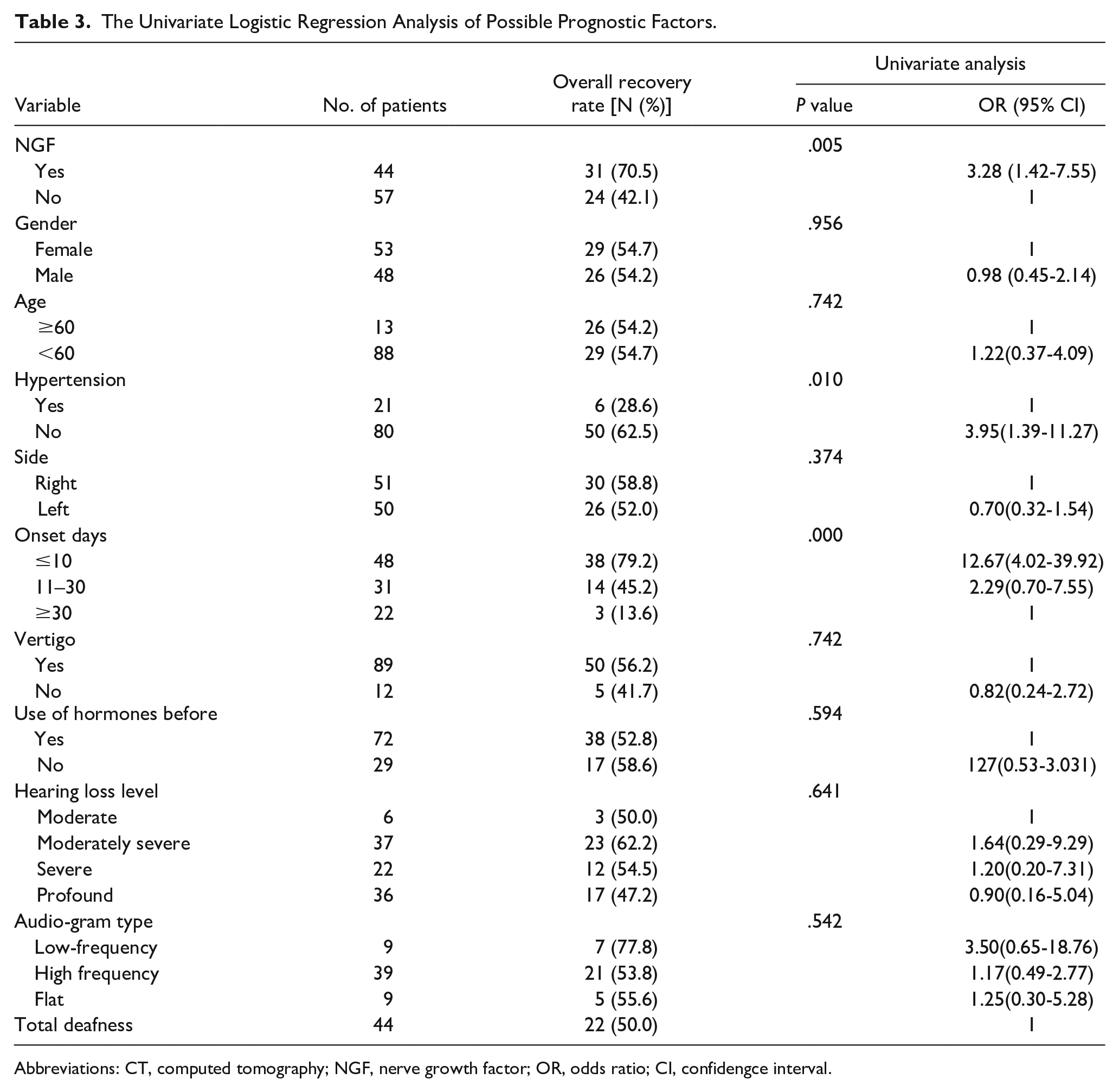
Abbreviations: CT, computed tomography; NGF, nerve growth factor; OR, odds ratio; CI, confidengce interval.
The Multivariate Logistic Regression Analysis of Possible Prognostic Factors
Parameters with a P value of <.05 in the univariate analysis were incorporated into the multivariate analysis. Consequently, NGF, hypertension, and onset days were selected for multivariate examination. The findings revealed that hypertension and onset days were associated with the efficacy of therapies for SSHL (Table 4).
The Multivariate Logistic Analysis of Possible Prognostic Factors.
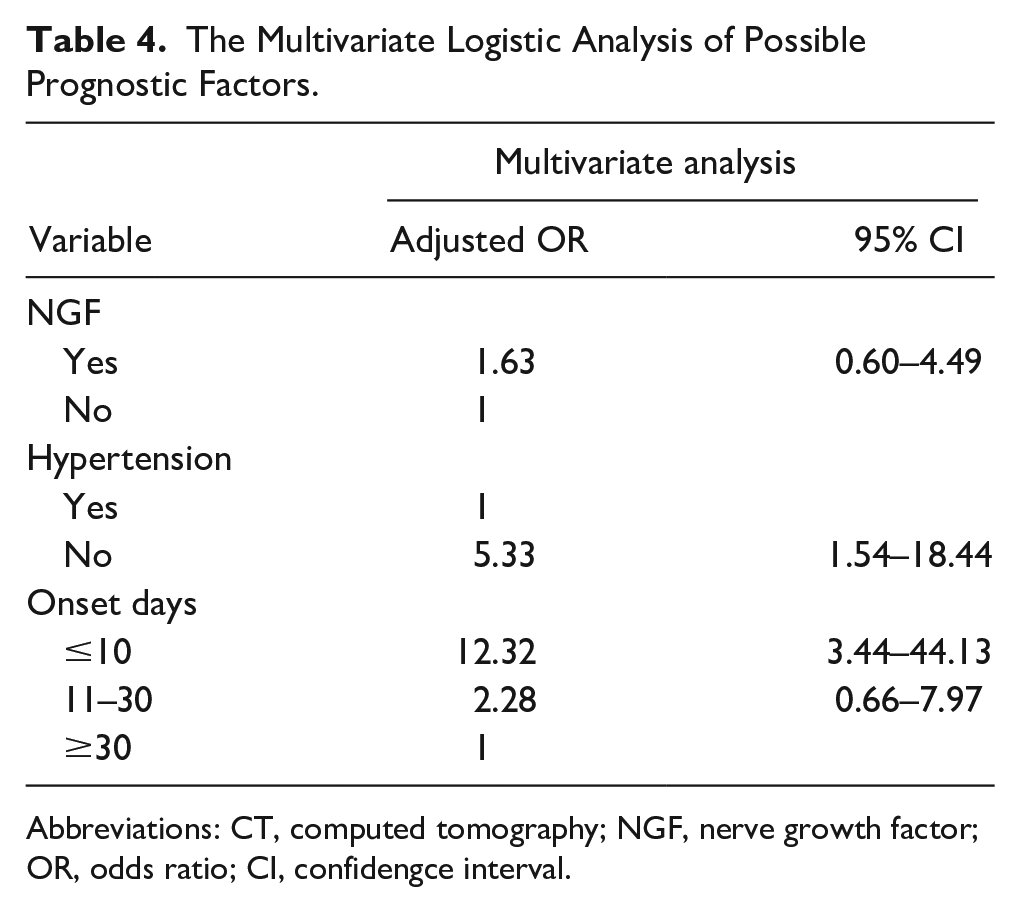
Abbreviations: CT, computed tomography; NGF, nerve growth factor; OR, odds ratio; CI, confidengce interval.
Discussion
The research demonstrates that PTA significantly improved after treatment in both groups, with a statistically significant difference (P < .05). The effective rate of hearing recovery in the control group was 42.1%, while it was 70.5% in the experimental group, exhibiting a statistically significant difference between the two groups (P < .05). Most patients experienced significant hearing improvement 1 week after treatment, and some patients still had improved hearing 2 weeks after treatment. Multi-factor analysis results indicated that hypertension and onset days were related to the curative effect.
It is known that SSHL is an ear disease that severely impacts health and causes distress to patients. Research has found that while some individuals with sudden deafness recover on their own, 60% or more still face hearing problems. 15 Lee et al suggest that persistent hearing impairment in these patients can lead to social isolation.16,17 Moreover, SSHL can result in tinnitus, and patients with tinnitus exhibit a higher prevalence of anxiety and depression than the general population.18,19 These findings highlight the harm that SSHL causes to patients and society. Currently, SSHL treatment requires further exploration, particularly regarding secondary treatment and the extended course of sudden deafness treatment, which remains at an exploratory stage. Very few people maintain a positive attitude toward secondary treatment. Thus, a retrospective analysis of the clinical data of 101 patients with moderate or above sudden deafness who received secondary treatment at Sun Yat-sen Memorial Hospital of Sun Yat-sen University from January 2019 to July 2020 was conducted to provide a reference for sudden deafness secondary treatment.
SSHL treatment is a comprehensive approach. Studies have confirmed that NGF and its receptors are expressed at varying degrees during each stage of inner ear development and maturation, 20 suggesting that NGF plays a crucial role in maintaining the normal development and maturation of the inner ear. Recent studies have also shown that NGF can enhance cochlear microcirculation by promoting cochlear microvascular damage repair and angiogenesis. 21 It can not only boost metabolism but also promote the elimination of harmful substances, such as oxygen free radicals, which can reduce hair cell damage and facilitate repair. 22 Based on this data, an analysis of clinical data of NGF in the treatment of sudden deafness was conducted. The findings showed that the total effective rate of the NGF group was higher than that of the conventional treatment group, indicating that NGF combined with conventional treatment is effective for secondary treatment of sudden deafness. However, in Dai’s study, 23 the success rate of salvage therapy for patients with sudden deafness was lower than in the present research. The influence of the number of days of illness included in the study cannot be ruled out. Additionally, an examination of all hearing for patients revealed that, in both the control and experimental groups, the vast majority of patients with hearing recovery had significant improvement within 1 week after treatment, and some patients had good hearing within 2 weeks. In contrast, instances of poor hearing improvement within 2 weeks rarely improved during 1 month of follow-up. This is consistent with the results of previous studies.24,25 Consequently, it is recommended that patients without significant hearing recovery after the first treatment should not give up.
Univariate and multivariate analyses were conducted to further investigate the factors influencing the efficacy of sudden deafness treatment. Univariate analysis revealed that statistically significant differences existed in NGF use, hypertension, morbidity days, and prognosis, while no statistically significant differences were observed in age, sex, ear position, accompanying symptoms, or first treatment with or without hormone use. Multivariate analysis indicated that the time of onset, hypertension, and prognosis were related. The results demonstrated that different types of hearing curves had varying prognoses, with low and intermediate frequency descending types being the best. This might be because the middle and low-frequency descending types could be due to labyrinthine fluid in the inner ear, which was easier to recover. Additionally, this study found no significant direct correlation between the use of hormones during the first treatment and the efficacy of the second treatment, primarily because the first treatment regimen differed from the second treatment regimen. The use of NGF in univariate analysis is a prognostic factor, and there is no statistical significance after multi-factor analysis. The analysis suggests that, since this study is a retrospective study, the inevitable defects, such as the non-randomization of the group and the non-placebo group as the control, may lead to the deviation of the results due to the number of cases in each factor group. In the future, the sample size should be expanded to further study the related factors affecting the prognosis of SSHL.
In conclusion, for the secondary treatment of sudden deafness, intravenous medication, simultaneous systemic and local hormone use, nerve nutrition, and other combined treatment approaches have a certain effect on improving hearing. Some patients even experience further hearing improvement 2 weeks after treatment. As a result, it is necessary to administer secondary treatment to patients with sudden deafness, and cases without hearing improvement 1 week after treatment should not be abandoned. Due to the small sample size included in this study, short follow-up time, and differences in gender, age, and other factors, this study has certain limitations. In the future, the sample size will be further expanded to conduct relevant studies to determine the therapeutic effect of sudden deafness under the influence of different factors, providing a basis for clinical treatment and prognosis assessment.
Conclusion
In general, secondary treatment for SSHL, although not highly effective overall, still has a certain impact on improving hearing. It indicates that the second treatment is of clinical significance for patients with SSHL who experienced failure or no significant effect after the first treatment. NGF may be effective in improving partial hearing.
Footnotes
Data Availability statements
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (number: 81970887)and the Guangzhou Science and Technology Foundation (number: 201903010088).
Ethical Approval
This study involves human participants and was approved by the ethics committee of Sun Yat-sen Memorial Hospital, China(approval number: SYSEC-KY-KS-2021-014).