
Abstract
Introduction
A tracheocutaneous fistula (TCF) occurs when the squamous epithelium forms an epithelialized tract that fails to close. 1 It is a common complication of long-term tracheostomy, which is required in some cardiopulmonary diseases, neuromuscular disorders, malignancy, and congenital anomalies, as well as for patients in the intensive care unit. 2 -5 Moreover, it is more common in younger patients and patients who undergo tracheostomy for long durations. 6,7 However, it was reported that children, who undergo tracheostomy for more than 1 year, have persistent TCF formation after decannulation in more than 43% of cases. 8 Furthermore, persistent TCF is associated with multiple complications, including persistent secretions, skin irritation, breathing difficulties, pulmonary complications, and social and cosmetic problems. 9,10 Therefore, TCF closure is required. Interestingly, different techniques are adopted for TCF closure. First, excision with primary closure includes TCF removal, re-approximation, and layer closure with or without a small drain. 11 -14 This procedure makes the primary closure technique more cosmetically appealing than the secondary closure. 15 Second, excision with healing by secondary intention closure comprises TCF excision, temporary tube placement, or small drain removal early in the postoperative period, thereby facilitating secondary intention closure, or followed by cervical tracheoplasty. 10,12,14 -16 Therefore, both techniques are considered major treatment options for TCF. Some systematic reviews and meta-analyses have compared the efficacy of primary closure with that of secondary closure. Both are associated with a high success rate and low complication rate, whether major or minor, and there are no significant differences between the 2 techniques. 16,17 The major complications of primary or secondary closures in children include subcutaneous emphysema, pneumothorax, acute airway obstruction, and necessity for revision surgery. In contrast, minor complications include superficial wound infection, airway granuloma, minor bleeding, air leak, and supplemental oxygen requirements. 16,17
Our literature search revealed recent increase in the application of other approaches for TCF closure, such as suture ligation, and grafting with cartilage and local or regional flaps. 11,18 -21 Some of these techniques have shown high efficacy, including short operating times with low complication rates, demonstrating avoidance of depression scars, recurrence, subcutaneous emphysema, pneumothorax, and infection. 21 -24 However, most of these studies were either case reports or conducted on a small population. Furthermore, we could not clarify the safety and efficacy of these approaches alone or compare them with primary closure, and, to the best of our knowledge, no systematic review or meta-analysis has compared them. Therefore, our systematic review and meta-analysis aimed to compare the susceptibilities and complication rates of these surgical procedures.
Methods
Reporting Guidelines
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 25
Literature Search
We searched 4 online databases (Web of Science, the Cochrane Library, PubMed, and Scopus) for relevant articles published from study inception to August 2022 using the following search strategy: “Tracheocutaneous Fistula” OR “Tracheocutaneous Defect” OR “Trachea Cutaneous Fistula” OR “Trachea Cutaneous Defect” OR “Trachea Skin fistula” OR “Trachea Skin Defect.”
Inclusion and Exclusion Criteria
The inclusion criteria comprised studies with at least 5 adult or child patients with persistent TCFs who underwent closure surgery by primary or flap repairs. All single- or double-arm interventional and observational studies were eligible for inclusion, whether prospective or retrospective. Studies had to report the outcomes of surgical repairs, such as successful closure rates and complications, to be eligible for inclusion.
In addition, we excluded the following: studies that investigated other surgical procedures, such as healing with secondary intention or closure with cauterization; studies with <5 patients; studies published in languages other than English, descriptive studies reporting the mechanism of surgery without clarifying the outcomes, reviews, animal studies, and conference abstracts.
Study Selection
The authors independently screened the database search results in 2 phases. First, titles and abstracts were screened, followed by screening of full texts using EndNote X8.0.1. Furthermore, any conflict regarding the eligibility of any study was resolved by discussion among the authors.
Data Extraction and Quality Assessment
We extracted general and baseline data for each study, which included the country, study design, population description, study duration, follow-up period, sex, age at closure, tracheostomy, and decannulation, and time from decannulation to closure and from tracheostomy to decannulation. The primary outcomes, such as the successful closure rate, were extracted and defined since further surgical closure was not required. The secondary outcomes were minor and major complications. The major complications included death, need for reintubation, subcutaneous emphysema, respiratory distress requiring tracheostomy tube replacement, and any complications that required surgical intervention. However, the minor complications included surgical wound infection, hematoma, granuloma, any mild respiratory compromise that required minimal management with oxygen or medical treatment such as stridor and tachypnea, and any conservatively managed wound complications. Furthermore, we assessed the quality of the included studies following the National Heart, Lung, and Blood Institute criteria since they provide many tools for different study designs, such as cohort, case series, and controlled interventional studies. 26
Statistical Analysis
We used the Open Meta-Analyst software to perform single-arm meta-analyses for each surgical method by calculating the pooled event rate with 95% confidence interval (CI) and classifying the patients according to their age groups into adults and children. In addition, we compared the 2 surgical procedures using the Review Manager software in the double-arm studies. We used the risk ratio (RR) with 95% CI for all categorical outcomes. Significant differences between the 2 procedures were defined by P values of <.05. Heterogeneity was assessed using the I 2 test, where the outcomes were considered to have an acceptable heterogeneity level when I 2 was <50%. Since the outcomes were homogeneous, we used a fixed-effects model. 27,28 Furthermore, meta-regression analyses were performed only in the primary closure group to investigate the effects of covariates (age group and age at closure, tracheostomy, and decannulation and time from decannulation to closure and tracheostomy to decannulation) on all outcomes. However, we could not perform meta-regression analyses for the flap repair group because of the limited studies that reported these covariates.
Results
Literature Search and Study Selection Results
Overall, 856 records were identified from literature search after screening for duplicates during the title and abstract process. Among the 65 studies eligible for full-text screening, only 27 were eligible for inclusion in our systematic review and meta-analysis. 7,12,13,15,21 -24,29 -46 Figure 1 presents the comprehensive details of the literature search and study selection process.
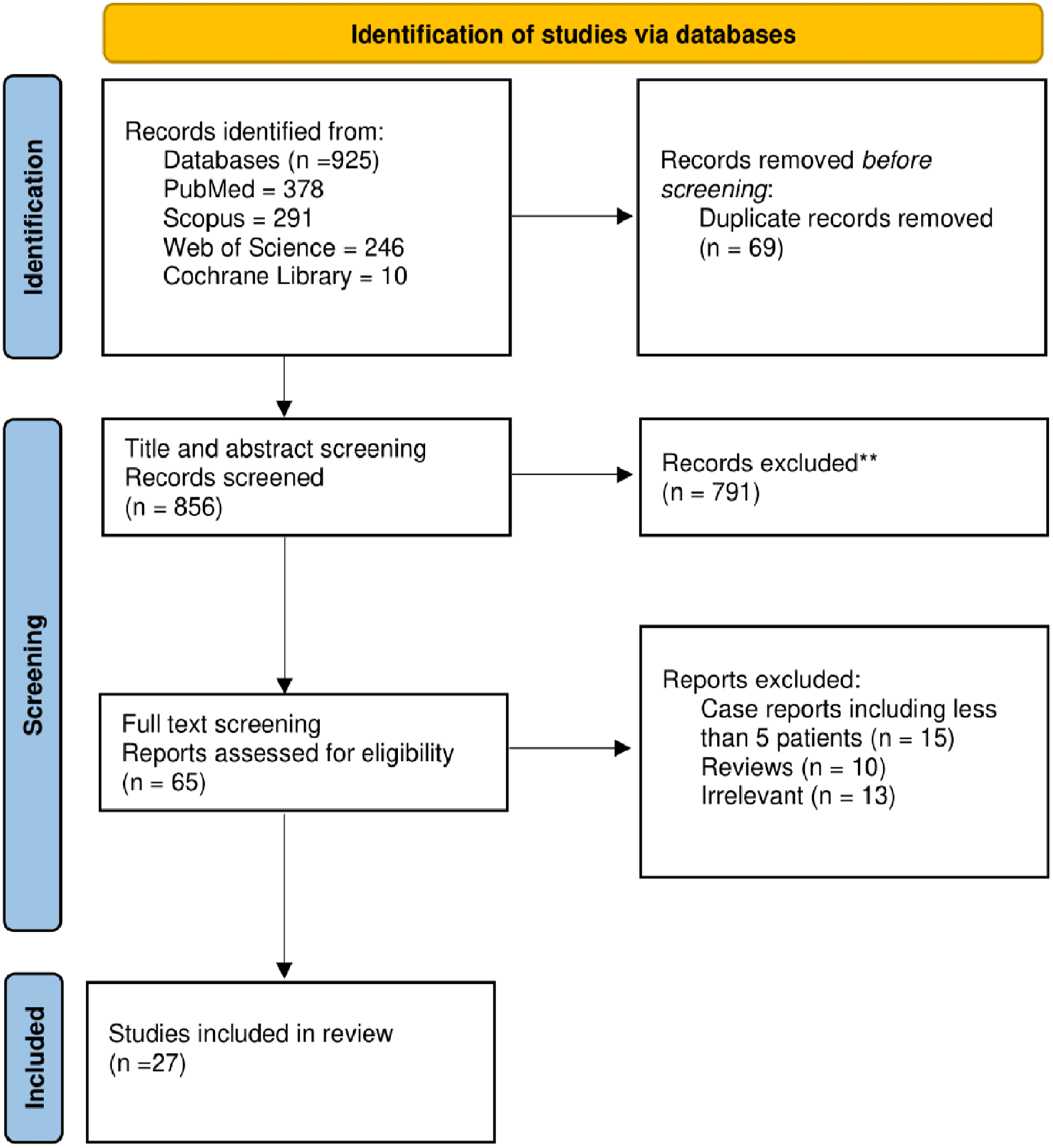
Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram.
General and Baseline Characteristics of the Studies
Among the 27 studies, 19 and 7 included only children 7,12,13,15,24,29,30,32,36 -45 and only adults, 21 -23,33 -35,46 respectively, and a single study included both children and adults. 31 In total, 20 studies investigated TCF closure by primary repair. 7,13,15,21,29,30,32,35 -45 In contrast, only 6 and 2 studies investigated flap closure 22 -24,31,33,46 and compared the 2 procedures, 12,34 respectively. Table 1 and Supplemental Table 1 present the full details of the included studies.
General Characteristics of the Included Studies.
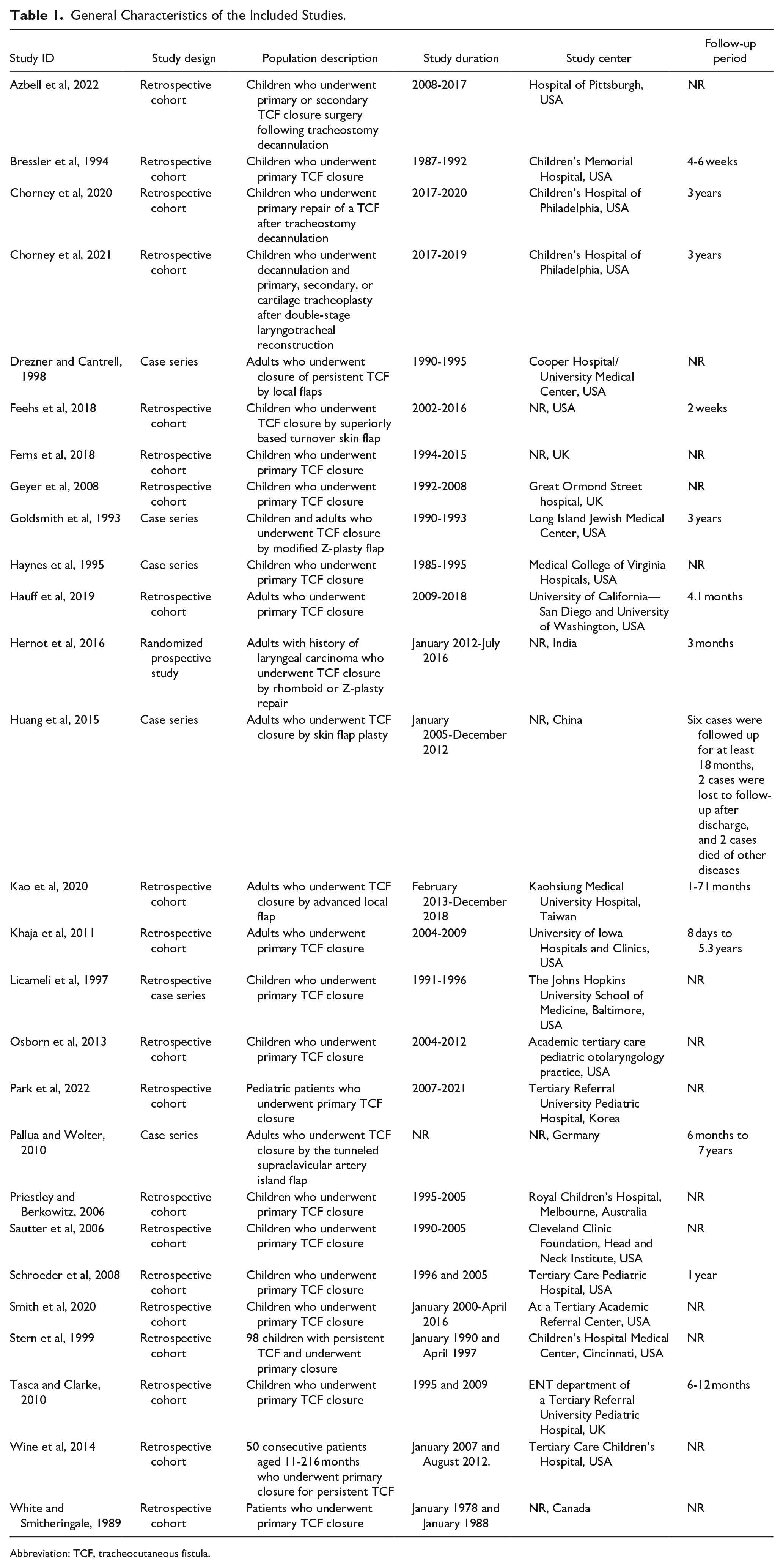
Abbreviation: TCF, tracheocutaneous fistula.
Quality Assessment
The observational cohort studies had acceptable quality assessment scores of 8 to 10 out of 14 points (Supplemental Table 2), 7,12,13,15,21,24,29,30,34 -42,44,45 while the case series studies had acceptable scores of 5 to 7 out of 9 points (Supplemental Table 3). 23,31 -33,43,46 Finally, the last interventional controlled study scored 9 out of 14 points, which was also acceptable (Supplemental Table 4). 22
Successful Closure Rate
Two studies compared both surgical procedures and found no significant difference (RR = 1, 95% CI = 0.82, 1.22, P = 1) (Supplemental Figure 1). 12,34
In the single-arm analysis of 19 studies that investigated primary closure (Figure 2), the overall success rate was 0.979 (95% CI = 0.968, 0.991). 7,12,13,21,32,34 -45 In addition, the overall success rates were 0.98 (95% CI = 0.969, 0.992) 7,12,13,32,36 -45 and 0.966 (95% CI = 0.911, 1.020) 21,34,35 in children and adults, respectively.
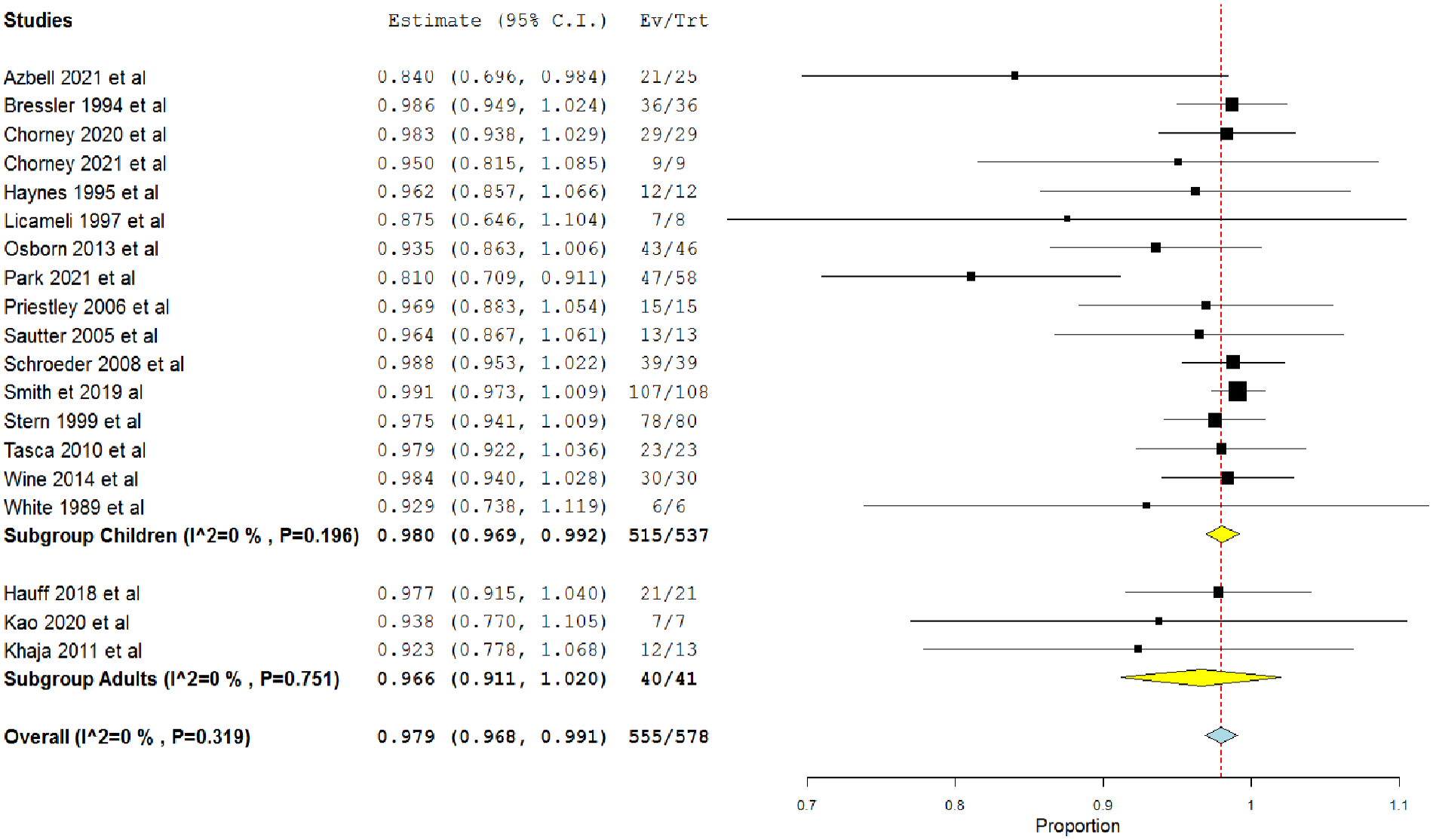
Single-arm meta-analysis of the success rate of the primary closure procedure in both adults and children.
However, the overall success rate was 0.98 (95% CI = 0.956, 1.004) in 8 studies investigating the flap closure (Figure 3). 12,22 -24,31,33,34,46 The rates were 0.979 (95% CI = 0.936, 1.022) 12,24,31 and 0.98 (95% CI = 0.951, 1.009) 22,23,31,33,34,46 in children and adults, respectively.
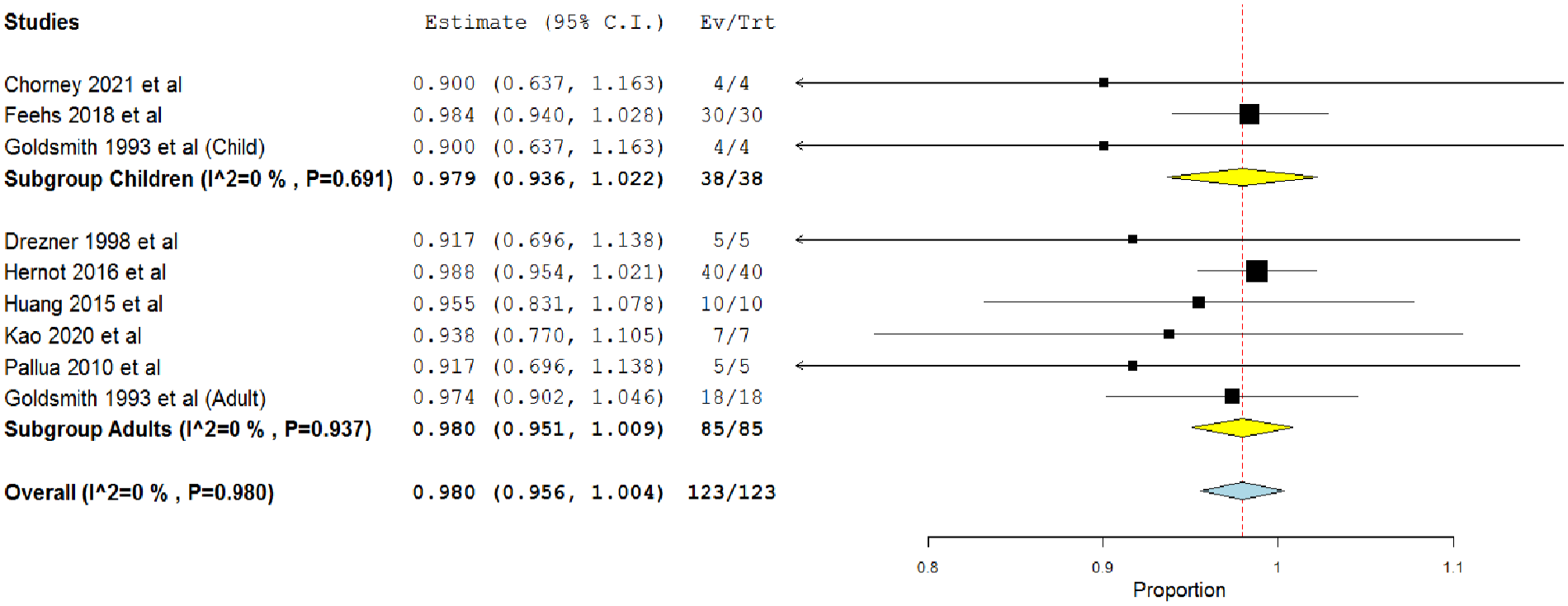
Single-arm meta-analysis of the success rate of the flap closure procedure in both adults and children.
Major Complications
The double-arm meta-analysis of 2 studies, which compared both procedures, showed no significant difference (RR = 0.69, 95% CI = 0.09, 5.12, P = .72) (Supplemental Figure 2). 12,34
The overall major complications rate in 21 studies that investigated primary closure was 0.034 (95% CI = 0.022, 0.047) (Figure 4). 7,12,13,15,21,29,30,32,34 -45 The rates were 0.033 (95% CI = 0.021, 0.046) and 0.059 (95% CI = −0.011, 0.129) in children 7,12,13,15,29,30,32,36 -45 and adults, 21,34,35 respectively.
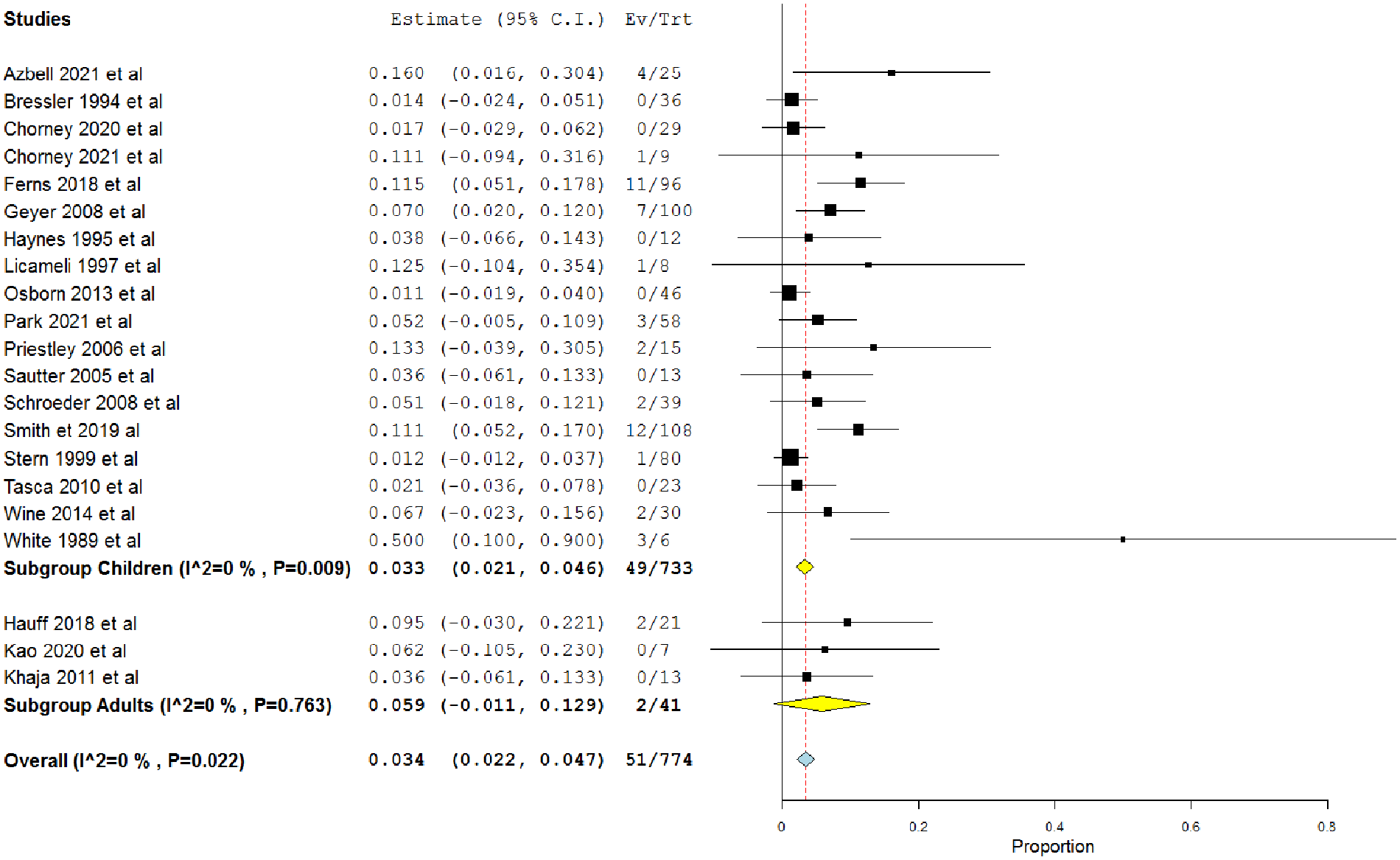
Single-arm meta-analysis of the major complications rate after the primary closure procedure in both adults and children.
Conversely, in 8 studies investigating the flap closure, the overall rate was 0.021 (95% CI = −0.003, 0.45) (Figure 5). 12,22 -24,31,33,34,46 The rates were 0.021 (95% CI = −0.022, 0.064) and 0.021 (95% CI = −0.008, 0.05) in children 12,24,31 and adults, 22,23,31,33,34,46 respectively.
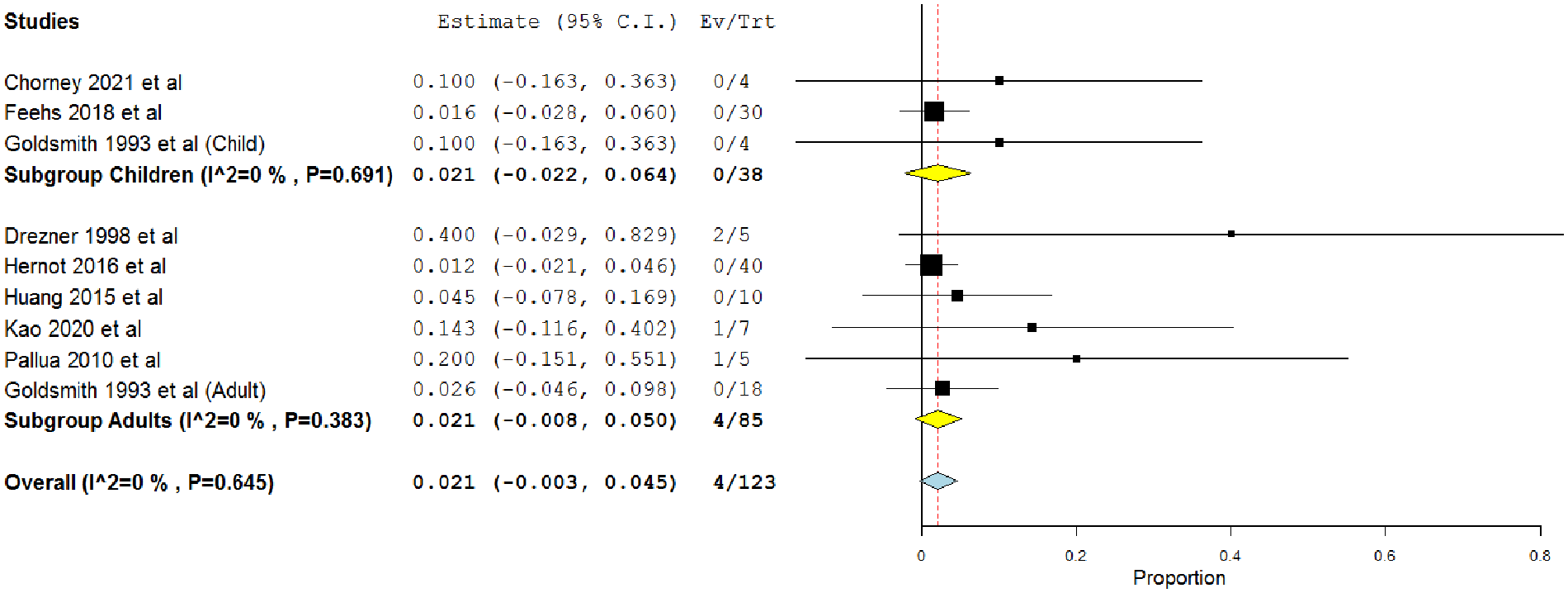
Single-arm meta-analysis of the major complications after the flap procedure in both adults and children.
Minor Complications
Although 2 studies compared both procedures, we could not perform a meta-analysis since Kao et al 34 did not find any minor complications in either group. However, Chorney et al 12 found that only 1 patient had minor complications in the primary closure procedure, but no patient had any minor complications in the other group.
The single-arm meta-analysis of 21 studies, which investigated the primary closure, revealed that the overall rate was 0.045 (95% CI = 0.031, 0.059) 7,12,13,15,21,29,30,32,34 -45 (Figure 6). In children, the overall rate was 0.047 (95% CI = 0.032, 0.61), 7,12,13,15,29,30,32,36 -45 whereas in adults, it was 0.03 (95% CI = −0.02, 0.08). 21,34,35
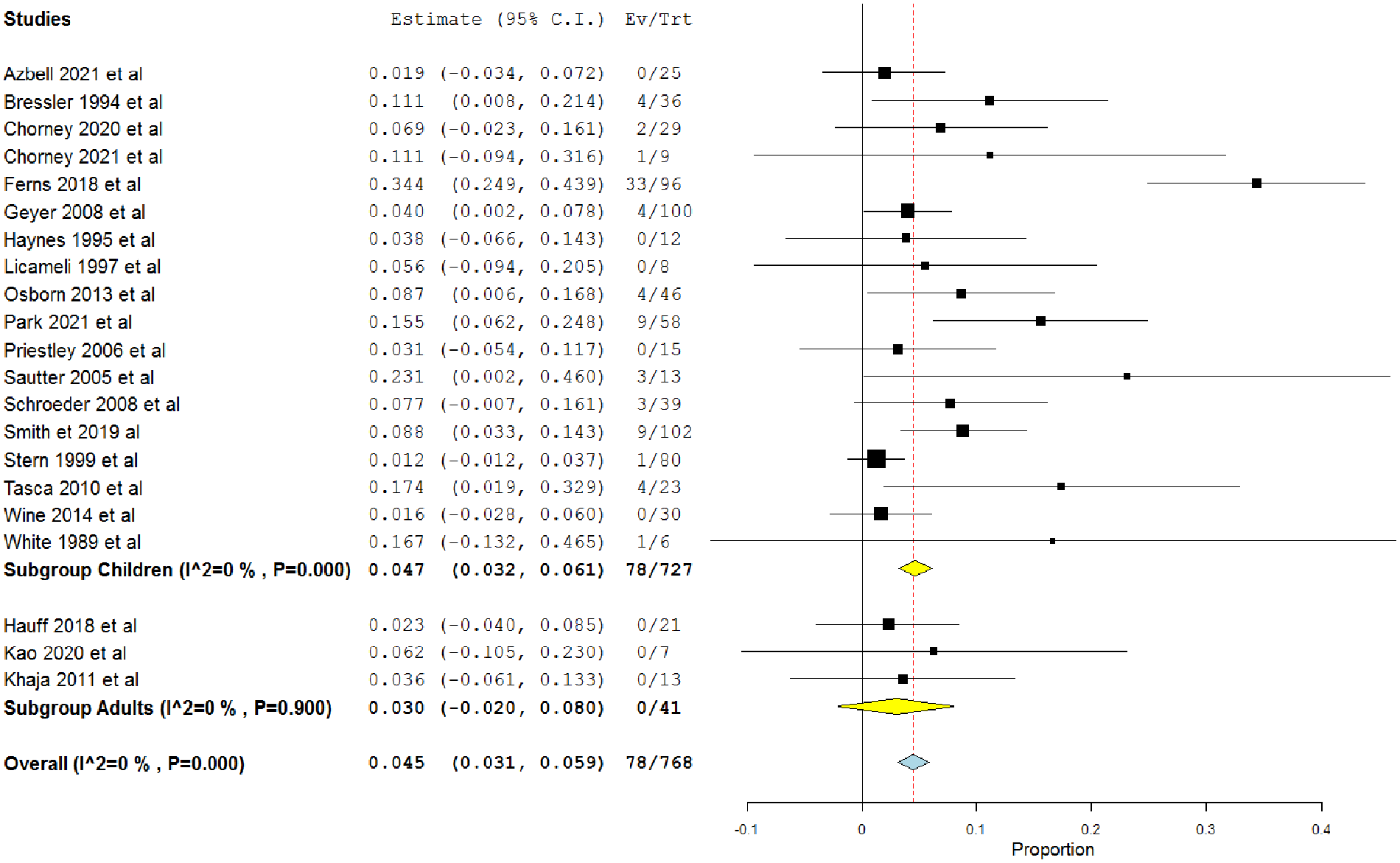
Single-arm meta-analysis of the minor complications rate after the primary closure procedure in both adults and children.
In the single-arm meta-analysis of 8 studies that used flap closure (Figure 7), the overall rate was 0.04 (95% CI = 0.008, 0.073). 12,22 -24,31,33,34,46 The overall rates were 0.021 (95% CI = −0.022, 0.064) and 0.067 (95% CI = 0.017, 0.117) in children 12,24,31 and adults, 22,23,31,33,34,46 respectively.
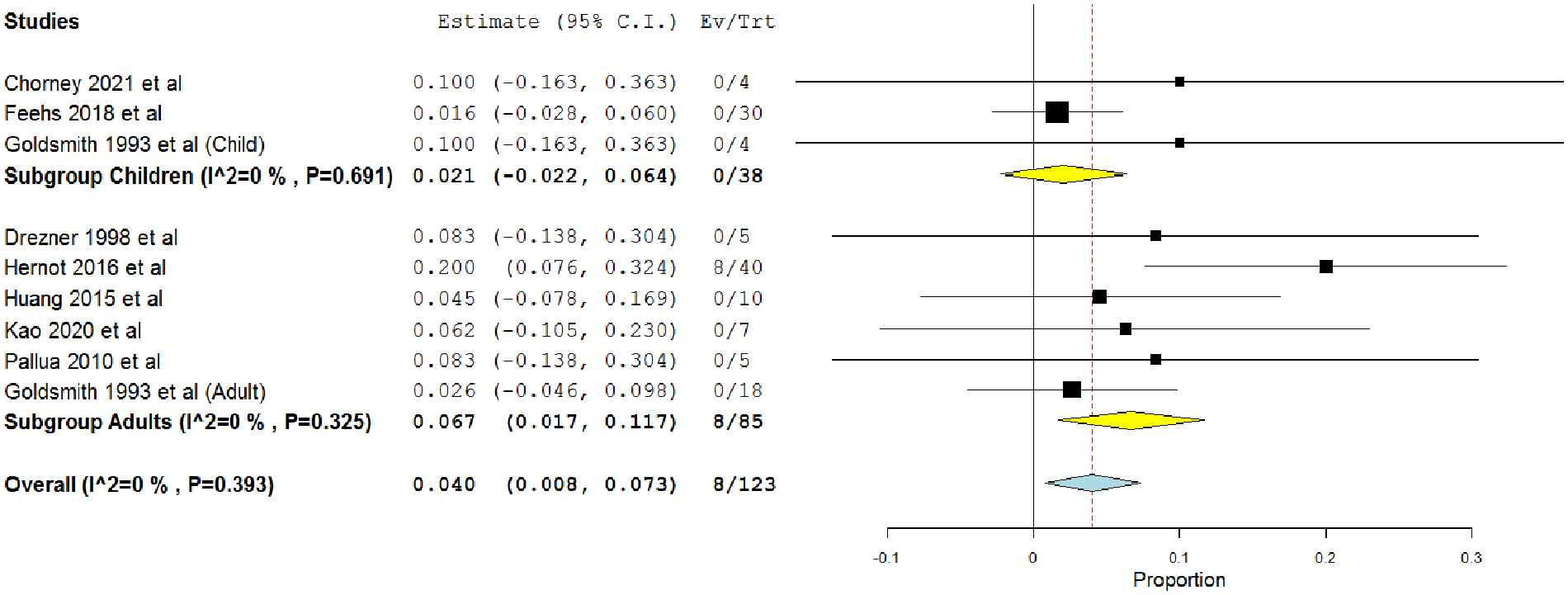
Single-arm meta-analysis of the minor complications after the flap procedure in both adults and children.
Meta-Regression
We assessed the baseline factors to determine if they could affect the outcomes of primary closure. We found that only age at decannulation negatively affected the success rate (regression coefficient = −.004, 95% CI = −0.007, −0.001, P = .002, Supplemental Figure 3A), whereas the time from decannulation to closure positively affected the major complication outcome (regression coefficient = .005, 95% CI = 0, 0.011, P = .04, Supplemental Figure 3B). However, we could not identify any factors that affected the outcome of minor complications.
Discussion
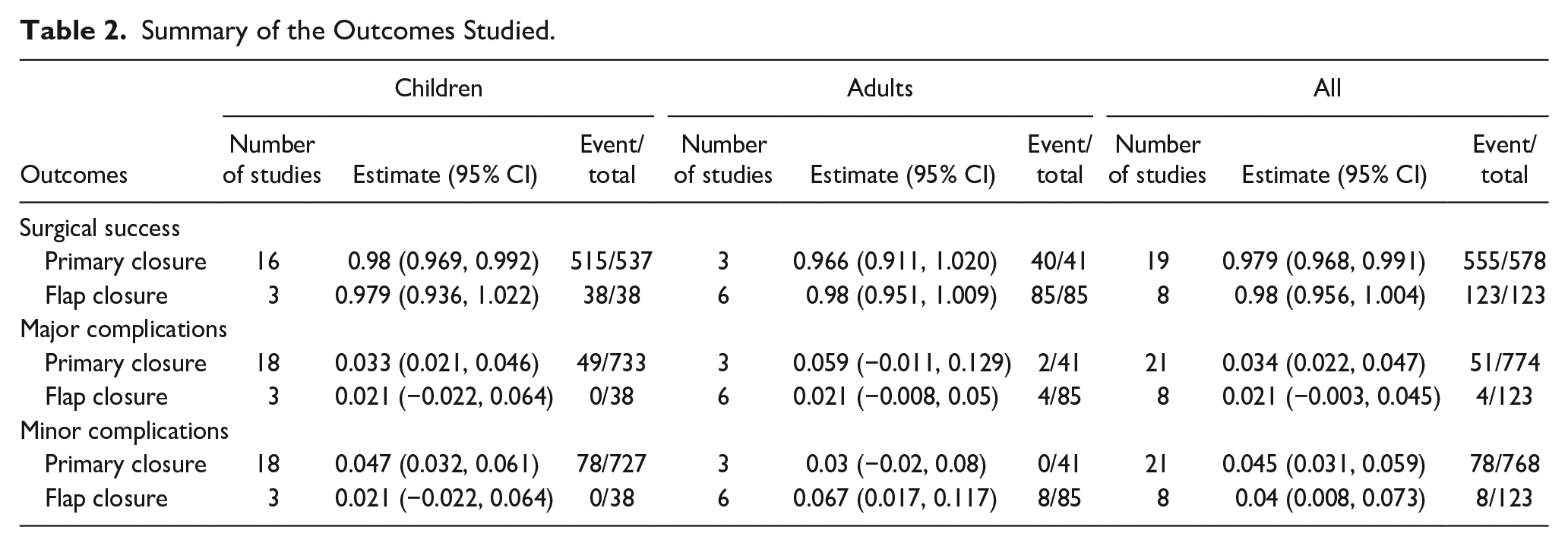
This systematic review and meta-analysis provide recent evidence comparing primary closure with flap closure of TCF in patients of various age groups. The double-arm analysis comparing both methods showed no significant difference between primary and flap repair regarding successful closure and major complication rates. Furthermore, in the single-arm analysis, we observed that the incidence of successful closure was 100% and 96% in the flap and primary closure groups, respectively. Moreover, flap closure showed lower incidences of major and minor complications (3.25% and 6.5%, respectively) than those of the primary closure (6.58% and 10.15%, respectively) (Table 2).
Summary of the Outcomes Studied.
TCF has become more common, particularly after prolonged tracheostomy cannulation. However, a long cannulation period and history of multiple tracheostomies have been linked to an increased incidence of persistent TCF. Overall, 50% of patients undergoing tracheostomy cannulated for >1 year have persistent TCFs because increasing the cannulation period enables epithelial tissue to create an epithelialized scar tissue and thick connective tissue within the stoma, resulting in persistent stoma. 47
Surgical repair remains the cornerstone of TCF management. Various surgical techniques for TCF closure have been established with promising results. However, they vary from simply using primary closure or fistula excision with secondary intention healing to applying a hinged closure to employ a harvested auricular or rib cartilage as a layer to close a large fistula defect. 20,48 -51
Cheng and Setabutr 16 conducted the first systematic review in children with persistent TCF that compared primary closure with simple excision and healing by secondary intention. They found no significant difference between the 2 techniques regarding safety and efficacy, which was supported by several cohort studies on children. 36,41 However, this study’s main limitation was inadequate randomization, which may cause allocation bias in cohort studies.
Another systematic review included 14 studies 16 investigating the safety and efficacy of surgical techniques used for TCF closure in children. However, they concluded that primary and secondary TCF surgical techniques are both effective regarding successful closure and complication rates and are both acceptable therapeutic alternatives. In this situation, surgical decision-making considerations may depend on social considerations, family, and cost differentials.
Comparison of the complications in primary and flap closures showed that some major complications, such as subcutaneous emphysema, respiratory distress requiring reintubation, and pneumothorax, were more strongly associated with primary closure. 12,29,30,37,38,43,45 In contrast, 1 patient had pneumothorax, 46 1 had subcutaneous emphysema, 23 and 2 had respiratory complications requiring reintubation 34,46 with flap closure. In addition, only Hernot et al 22 reported infections and blackish discoloration of the scar as minor complications with flap closure, particularly with the Z-plasty procedure, 22 while minor complications reported with primary closure included wound infection, granuloma, mild respiratory distress without requiring reintubation, stridor, and hematoma. 12 -14,29,30,36,37,39,40,42 However, direct comparisons between the 2 procedures regarding the incidence and type of complications were limited in the literature, which made conducting randomized controlled trials essential in determining the actual incidence.
Kao et al 34 performed the first study to address TCF management using a decision algorithm and modified risk score methodology. In this retrospective review, 7 patients had simple primary closures with fistulectomies, 6 had hinged turnover flaps with fistulectomies, and 1 had perforator flap reconstruction customized to the fistula size and peri-fistula soft tissue condition. Notably, all patients recovered without complications, and no surgery-related problems or incomplete TCF closures were observed during the first to 71-month follow-up period. Specifically, they used the following algorithms for treatment. Patients with TCF were examined after at least 3 months of follow-up and further split into 4 groups as follows: group A (TCF size 5 mm with spontaneous closure); group B (TCF size 5 mm without spontaneous closure); group C (TCF size 5-10 mm); and group D (TCF size >10 mm). All patients in group A eventually healed spontaneously during the follow-up period. In addition, patients in group B required primary repair; while those in group C required the local flap technique. Furthermore, ptaints with a TCF size >10 mm required the reinforcement technique. 9,51
This review was limited by its small sample size, retrospective design, and selection bias when a special surgical technique was selected for individual patients. Therefore, more prospective trials with larger sample sizes are required to validate this algorithm.
Although many flap closure methods have been described in the literature, only a few studies have compared them. A case series of 40 patients that compared rhomboid flap repair with Z-plasty was published by Hernot et al. 22 They reported that patients in the rhomboid flap group were associated with overall good results compared with those in the Z-plasty group who experienced complications in 8 cases. Therefore, this study revealed that TCF repair using a rhomboid flap was superior to Z-plasty repair and the main drawback of Z-plasty was tip skin necrosis. In addition, they concluded that flap closures are less likely to develop postoperative tracheal stenosis, recurrence of TCF, or wound dehiscence because the skin’s suture line cannot overlap with that of the subcutaneous tissue. In addition, repair with flap covering does not result in the creation of a depressed scar later in life, as seen in individuals with TCF who are left for secondary intention healing.
To the best of our knowledge, this is the first meta-analysis to compare the safety and efficacy of primary and flap closures of TCF with a relatively large sample size of 997 cases. One of our strengths was the study of different age groups. Furthermore, we searched for factors that might affect the success and major complication rates using a meta-regression model. We found a significant decrease in the success rate with increasing age at the time of decannulation. In addition, the risk of major complications increases with increasing time from decannulation to closure.
Limitations
The main limitation is that most of the included studies were retrospective, relying on the participants’ recollections of events; therefore, they would be susceptible to recall bias besides the inherent bias of observational designs. Moreover, most of the analyses in our study were single-arm meta-analyses and the double-arm meta-analyses included only 2 studies; thus, we were unable to accurately determine the best procedure as single-arm meta-analyses lacked the direct comparison between the 2 procedures. This resulted from the extremely limited number of studies comparing both procedures in existing literature. Therefore, we recommend conducting randomized controlled trials comparing both procedures in future.
There are different indications for both surgical procedures; however, the main goal was to investigate the efficacy and safety of flap closure and to compare it with standard primary closure surgery. In addition, we performed double-arm meta-analyses comparing the 2 procedures in studies that included patients with the same baseline characteristics; however, as the number of eligible studies was small, we included single-arm studies to compare the efficacy of both procedures. Therefore, further randomized control trials including patients with the same baseline characteristics comparing both procedures are necessary.
Conclusion
Both primary and flap repairs of TCF are acceptable therapeutic alternatives with effective closure success and complication rates. Flap closure showed a lower incidence of complications and could be considered as an alternative approach or when other techniques have failed. However, more prospective randomized studies comparing these 2 procedures are needed to support our results.
Supplemental Material
sj-docx-1-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-docx-1-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-2-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-docx-2-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-3-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-docx-3-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-4-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-docx-4-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Supplemental Material
sj-docx-5-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-docx-5-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Supplemental Material
sj-png-6-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-png-6-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Supplemental Material
sj-png-7-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-png-7-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Supplemental Material
sj-png-8-ear-10.1177_01455613231179690 – Supplemental material for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review
Supplemental material, sj-png-8-ear-10.1177_01455613231179690 for Comparison Between Flap and Primary Closures of Persistent Tracheocutaneous Fistula: A Scoping Review by Nasser Almutairi, Waleed Alshareef, Latifah Almakoshi, Abdulmajeed Zakzouk, Abdullah Aljasser and Ahmed Alammar in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.