
Abstract
Introduction
Residency boot camps have been established as an effective method of teaching. The first Otolaryngology-Head and Neck Surgery (ORL) ) boot camp described in the literature was developed at MedStar Georgetown University in 2011 to prepare junior residents for emergencies. 1 Since then, an increasing number of ORL residency programs have developed their own boot camps. A 2022 systematic review examining residency ORL boot camps across the world identified 16 studies demonstrating their efficacy. 2 Most boot camps were 1-day, intensive programs including didactics and clinical skills with task trainers and simulators. However, there is a paucity of studies and interventions aimed at increasing ORL knowledge and skill acquisition in medical school.
There are limited opportunities in the medical school curriculum to learn about the field of ORL and to acquire relevant clinical skills, especially during preclinical years. Studies have shown that about 50% of pediatric patients and 20% of adult patients seeing a general practitioner report an ORL complaint.3,4 Therefore, it is essential for all medical students to learn about common ORL problems and associated management regardless of their intended future specialty. Recent studies have demonstrated that comfort levels in managing ORL problems can be improved through teaching reinforcement.5,6 Such intervention aims to prepare medical students to handle these problems adequately prior to starting clinical clerkships.
The objective of this pilot study was to investigate the impact of implementing an ORL boot camp in preclinical undergraduate medical education to help first- and second-year medical students learn about common ORL problems and become more comfortable performing basic ORL clinical skills so that they would be prepared better to provide care for patients during clerkships and in their future careers.
Methods
A 3-hour boot camp consisting of didactics/demonstrations and clinical skills experiences was developed by the authors (L.J.T. and R.T.S.) (Figure 1). A flyer was sent out to all first- and second-year medical students at Drexel University College of Medicine for recruitment to the study. Written informed consent was obtained by all subjects. During the first 5 minutes of the boot camp, an anonymous pre-test consisting of 21 subjective (0–5 point Likert scale; 0 = none, 5 = most) and objective (content) questions was administered to all subjects via Google Forms to assess baseline demographics and ORL knowledge. Random number identifiers were assigned to subjects to permit pre- and post-tests to be deidentified and paired. Next, subjects participated in didactics and demonstrations for 85 minutes presented by the senior author (R.T.S.). These sessions included a brief introduction into the field of ORL, description of common ORL pathologies, associated management and procedures, and demonstrations of basic ORL procedures typically performed in clinic. Topics included hearing loss, tinnitus, dizziness, facial paralysis, otitis, turbinate hypertrophy/epistaxis, chronic sinusitis, obstructive sleep apnea, skull base tumors, pharyngitis, tonsillitis, dysphonia, vocal fold masses, vocal fold paresis/hypomobility, laryngopharyngeal reflux, dysphagia, lymphadenopathy, thyroid pathology, neck masses, and others. Next, subjects practiced basic ORL skills on their peers in small groups under the supervision of attending physicians, residents, and senior medical students in the Otolaryngology Pathway for 85 minutes. Skills included otoscopy, tuning fork tests, examination with a nasal speculum, and oral, basic cranial nerve, and neck examination. During the last 5 minutes of the boot camp, deidentified post-test consisting of 24 subjective (0-5 point Likert scale; 0 = none, 5 = most) and objective (content) questions was administered via Google Forms to evaluate the efficacy of the boot camp in developing knowledge, self-confidence, and interest in ORL.
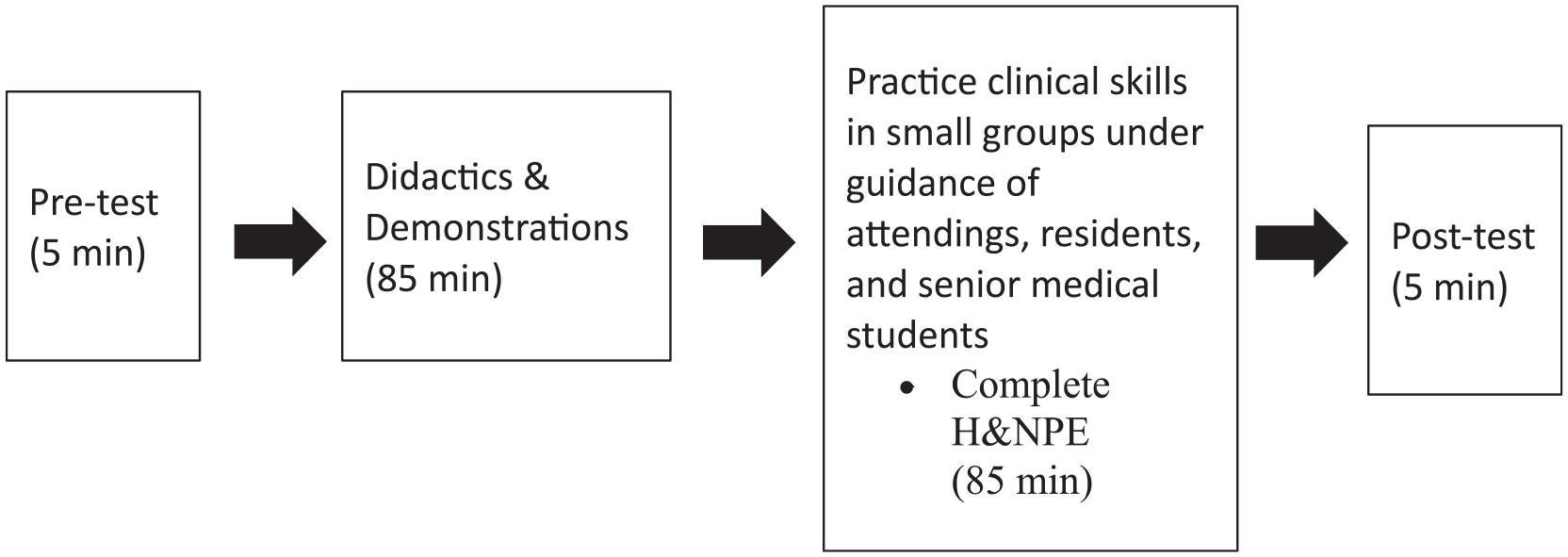
Organization of boot camp.
Mean pre- and post-test self-reported ratings and content examination performance were compared using two-sampled independent t-tests. Data were analyzed with SPSS 28.0 (IBM Corporation, Armonk, New York, USA), and significance was defined at the P < .05 level.
Results
A total of 17 first- and second-year medical students participated in the boot camp. Seventeen students completed pre-tests and 16 completed post-tests. Of the 17 subjects, 15 reported a surgical specialty as their current specialty of interest (13 ORL, 1 General Surgery, 1 Orthopedic Surgery), and 2 reported an interest in primary care or a medicine subspecialty (gastroenterology). Subjects had a mean Likert rating of 1.47 for prior experience/exposure to ORL and a mean of 2.25 head and neck physical examination (H&NPE) performed prior to the boot camp, which included a less comprehensive H&NPE taught in the current curriculum. Ratings of self-reported knowledge of ORL and comfort level in performing H&NPE increased significantly from 2.06 to 3.00 (P = .019) and 1.76 to 3.44 (P < .001), respectively, after the boot camp (Figure 2). Performance on the 12-question content exam also increased significantly from 42.16% to 71.35% correct (P < 0.001). Interest in doing a clinical rotation in ORL increased from 4.24 to 4.69 (P = 0.344), and interest in ORL as a career increased from 3.94 to 4.38 (P = 0.38), although results were not significant. Furthermore, ratings of the importance of ORL in primary care increased from 3.94 to 4.25 (P = 0.139), but results were also not significant.
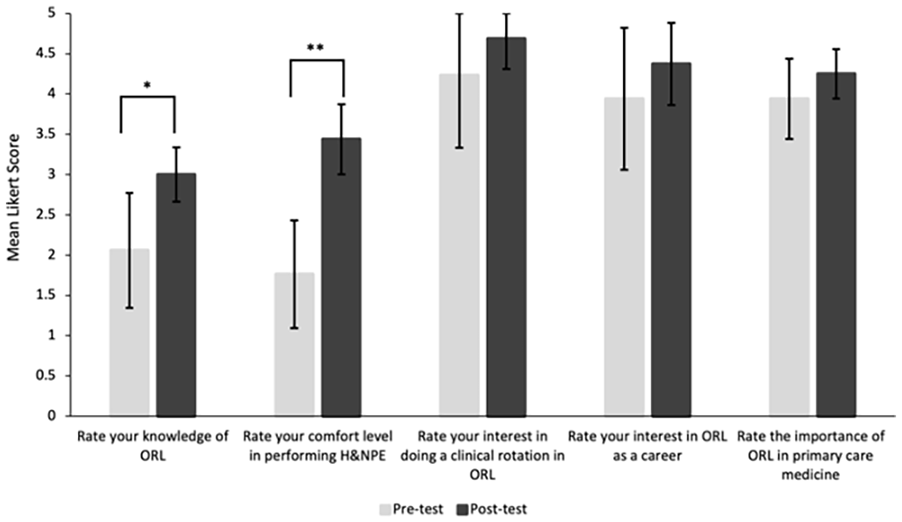
Medical students’ ratings of knowledge, comfort level, interest, and importance of otolaryngology. ORL = otolaryngology. Pre-test: n = 17, Post-test: n = 16, Error bars indicate 95% confidence interval.
Overall, subjects rated the effectiveness of the boot camp as 4.69, with 0 being not effective and 5 being very effective. 100% of respondents answered “Yes” to the prompts “Do you feel that the boot camp was helpful in preparation for clinical rotations?”; “Do you think that the boot camp should be incorporated to the medical education curriculum?”; and “Do you feel that the boot camp is helpful in career exploration?” Furthermore, 81.25% of respondents believed that the boot camp should replace the Head and Neck Foundations of Patient Care session in the current curriculum at Drexel University College of Medicine and 93.75% believed that it should be added in addition to the current curriculum.
Discussion
To our knowledge, this is the first study to use subjective and objective measures to assess the efficacy of an ORL boot camp for preclinical medical students. These first- and second-year medical students have less clinical exposure compared to senior medical students because the first 2 years are dedicated mostly to didactic learning of the basic sciences and foundational clinical skills. There is also often significantly less emphasis on teaching ORL in the curriculum compared to specialties such as cardiology, pulmonology, nephrology, musculoskeletal medicine, neurology, psychiatry, gastroenterology, endocrinology, and reproductive health. Studies performed at United States medical schools over the past 20 years have consistently demonstrated underrepresentation of ORL in preclinical medical school curricula, resulting in variable and limited exposure for students.7-10 Additionally, ORL clinical skills are not emphasized. At our institution, there is currently only 1 formal ORL 60-minute H&NPE skills lesson taught in the first-year curriculum. This H&NPE covers basic tests and is not comprehensive. Many medical schools across the US face similar challenges since the H&NPE is taught across fields of medicine other than ORL such as family medicine, internal medicine, and neurology. 9 Without more exposure and practice, students often do not feel confident in their H&NPE skills, especially when using instruments like otoscopes and tuning forks. This is significant because ORL problems constitute a large proportion of complaints from pediatric and adult patients presenting to primary care specialists,3,4 which comprise approximately half of third-year core clerkships. Additionally, because of limited exposure, students may not know until later in their medical training, typically during third-year surgical electives, whether they are interested in ORL. This may deter students from pursuing ORL even if they do have an interest in the field, since it is one of the most competitive specialties, 11 and they may not have the relevant experiences and the time to build a strong residency application prior to submission. Furthermore, the availability of an ORL elective is dependent on the individual hospital at which a student rotates. So, it is possible that a student may never gain clinical experience in ORL prior to deciding what specialty to pursue. Our boot camp aims to equip medical students with basic knowledge of and skills in ORL to prepare them for clerkships and to increase exposure to and potentially interest in the field.
This study demonstrates that a single 3-hour boot camp for medical students can be an effective method of teaching. Students reported increased knowledge in ORL and increased comfort level in performing a H&NPE. This is consistent with a previous study that found an increase in medical student self-reported comfort levels after participating in a H&NPE teaching session as part of their school curriculum. 5 However, that study did not evaluate knowledge. In addition to self-reported measures, we included 12 content questions in the pre- and post-tests to assess knowledge. Performance on the exam material demonstrated nearly a 70% increase in ORL knowledge after the boot camp. All subjects felt that the boot camp was helpful in preparation for clinical rotations and for career exploration, and they opined that the boot camp should be incorporated into the medical education curriculum.
Currently, ORL teaching for preclinical medical students at US medical schools is typically in the form of anatomy lab and basic science lectures, without a focus on diagnosis and management of ORL pathologies.9,10,12 It also may be in the form of clinical shadowing, online reading material, online question banks, simulation modules, and isolated H&NPE teaching sessions.9,10 Opportunities to learn about ORL in depth in medical school are provided to students in their clinical years, primarily through third year electives and fourth year sub-internships. Additionally, novel interventions such as simulation curricula have been directed at improving management skills for clinical medical students, as they have been shown to be too challenging for preclinical medical students due to insufficient prior knowledge and low familiarity with ORL. 13 Our boot camp bridges the gap for preclinical medical students by reviewing basic anatomy, providing robust clinical background information, and applying basic clinical skills with instructions and frequent feedback from teachers.
There are limitations to this study that are important to consider. While the recruitment flyer was sent out to the entire first- and second-year classes and all efforts were made to recruit a diverse sample population, the subjects in our study were biased toward those who were already interested in ORL (76.47%). This may explain the unanimous and near-unanimous positive subjective responses regarding the helpfulness and effectiveness of the boot camp, as well as the absence of a significant difference after the boot camp in interest in doing a clinical rotation in ORL, interest in ORL as a career, or the importance of ORL in primary care, all of which were high on the pre-test. The boot camp was developed as a non-mandatory extracurricular session; and as such, it is likely that those who were interested in ORL were more likely to attend compared to those interested in other specialties. Participation was voluntary and no remuneration was offered. These factors also may explain the small sample size. It is possible that a higher-powered study with a subject pool with more diverse interests could demonstrate differences. Despite these limitations, we believe that valuable information was transmitted to students from the boot camp, even to the biased group of people already interested in ORL. The increases in self-reported knowledge and comfort levels were still significant, and those measures are less likely to be affected by biased interest in ORL. For instance, none of the subjects, including those interested in ORL, had used a head mirror or nasal speculum prior to the boot camp. This novel experience likely influenced their ratings. The significant increase in objective content exam material performance provides further support. The results from this pilot study show promise; however, further studies with a larger cohort, including those not already interested in ORL, should be performed to determine whether such intervention increases interest in ORL.
Conclusions
Implementing an ORL boot camp consisting of didactics/demonstrations and clinical skills in undergraduate medical education appears to be an effective and efficient method of teaching for preclinical medical students. By increasing early exposure to ORL, it also holds potential for increasing student interest in the field. Further studies including larger, more diverse cohorts are encouraged.
Supplemental Material
sj-pdf-1-ear-10.1177_01455613231179686 – Supplemental material for Otolaryngology-Head and Neck Surgery Boot Camp in Preclinical Undergraduate Medical Education: A Pilot Study
Supplemental material, sj-pdf-1-ear-10.1177_01455613231179686 for Otolaryngology-Head and Neck Surgery Boot Camp in Preclinical Undergraduate Medical Education: A Pilot Study by Leona J. Tu and Robert T. Sataloff in Ear, Nose & Throat Journal
Supplemental Material
sj-pdf-2-ear-10.1177_01455613231179686 – Supplemental material for Otolaryngology-Head and Neck Surgery Boot Camp in Preclinical Undergraduate Medical Education: A Pilot Study
Supplemental material, sj-pdf-2-ear-10.1177_01455613231179686 for Otolaryngology-Head and Neck Surgery Boot Camp in Preclinical Undergraduate Medical Education: A Pilot Study by Leona J. Tu and Robert T. Sataloff in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
The authors thank the faculty and staff in the Department of Otolaryngology-Head and Neck Surgery at Drexel University College of Medicine for their assistance in teaching the H&NPE to students.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Drexel University Institutional Review Board (protocol 2209009462).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Drexel University Institutional Review Board (protocol 2209009462) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the subjects for their anonymized information to be published in this article.
Research Data
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials. Supplementary material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.