
Abstract

Significance Statement
With a rising incidence of gonococcal infections, oral gonorrhea may be easily overlooked but is highly treatable with antibiotics. We describe a rare case of profound lingual tonsil hypertrophy associated with gonococcal pharyngitis requiring lingual tonsillectomy due to progressive symptoms despite appropriate antimicrobial therapy. This case highlights the importance of keeping a broad differential for sexually active patients with tonsillar hypertrophy as well as the unique management strategies deployed in symptomatic medically refractory cases.
A 22-year-old female presented with progressive cervical lymphadenopathy, dysphonia, dysphagia, snoring, and shortness of breath exacerbated by lying flat. She had a tonsillectomy in her youth and distant Epstein-Barr virus infection (immunoglobulin G positive, immunoglobulin M negative on serology). Notably, she was found to have a chlamydia infection at a routine gynecological visit 7 months prior. At the time of her visit, she denied any stridor, hemoptysis, fevers, or unintentional weight loss. She had no history of tobacco use.
Workup for her cervical lymphadenopathy included an ultrasound that showed an abnormal 1.8 × 1.2 × 4.5 cm left submental neck mass thought to be an enlarged lymph node. However, a computed tomography neck scan with contrast confirmed prominent lingual tonsillar tissues effacing the vallecular and exerting downward mass effect on the epiglottis without any pathologically enlarged lymph nodes (Figure 1). One week prior to her ENT clinic visit, she was screened for sexually transmitted infections, at her request, and pharyngeal swab was positive for Neisseria gonorrhoeae by polymerase chain reaction. Patient was treated with intramuscular ceftriaxone and repeat swab 4 weeks later confirmed clearance. During her ENT clinic visit, flexible laryngoscopy was notable for profound lingual tonsil hypertrophy with distortion of laryngeal anatomy (Figure 2).
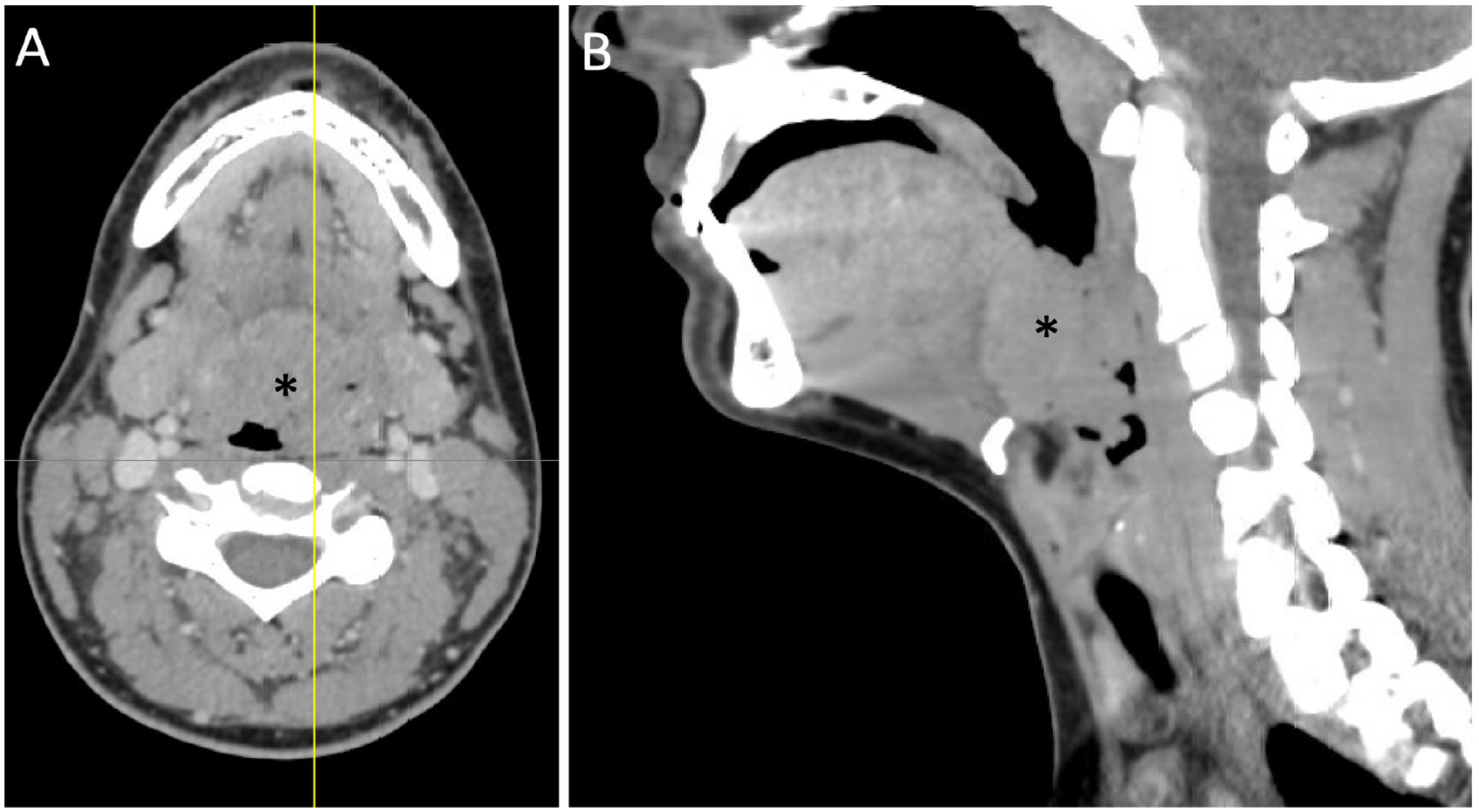
Computed tomography of the neck with contrast. (A) Axial scan showing remarkable lingual tonsil hypertrophy (*) with narrow and skewed airway. (B) Sagittal scan showing profound lingual tonsil hypertrophy (*) and narrowing the supraglottic airway.
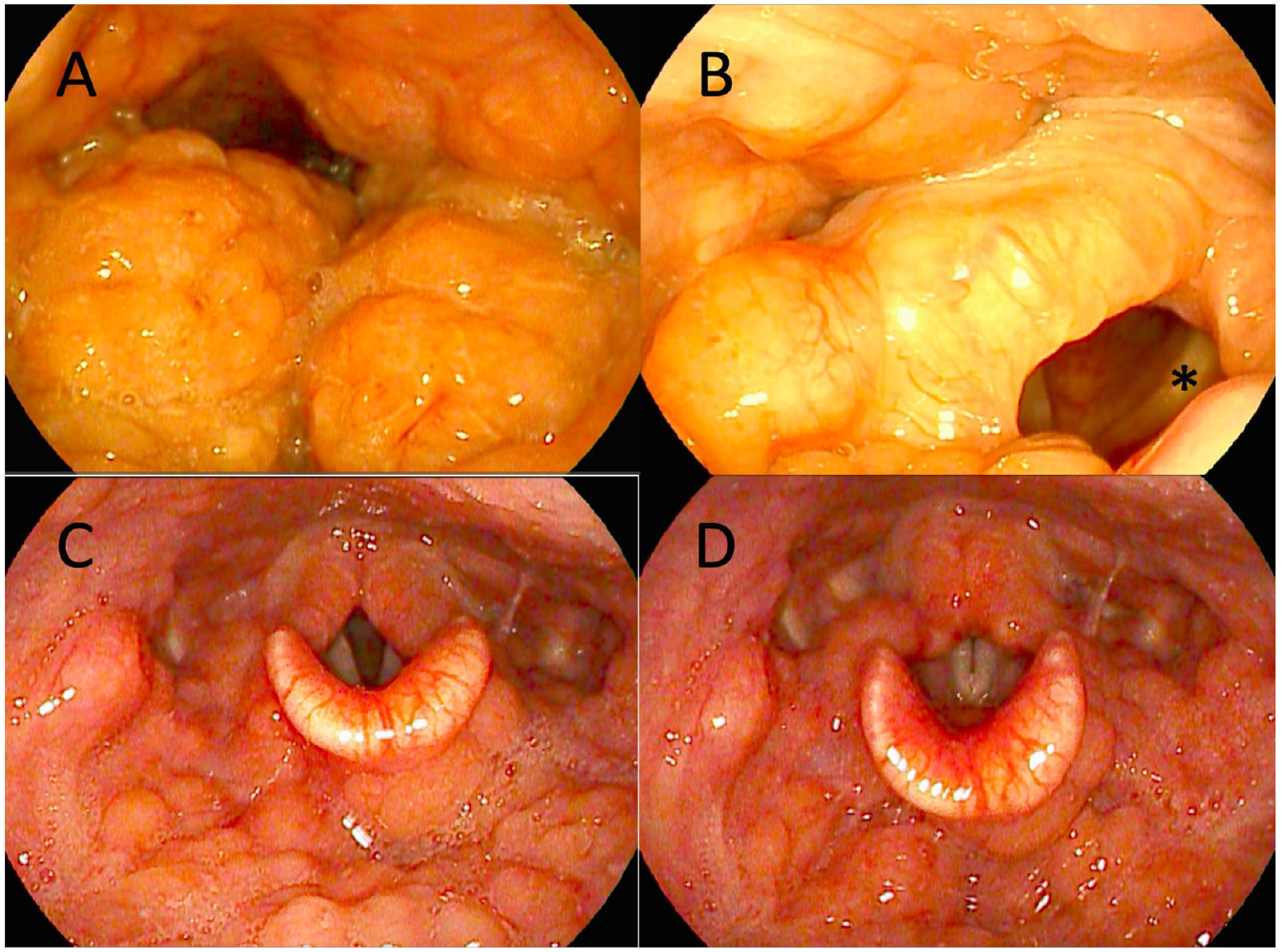
Flexible laryngoscopy of lingual tonsils. (A) Lingual tonsil hypertrophy seen on initial evaluation. Notably, no supraglottic structures are visible. (B) Laryngeal inlet around marked lingual tonsil hypertrophy and distortion of the epiglottis. Left true vocal fold (*) visible for reference. (C) Oropharyngeal view 6 weeks after lingual tonsillectomy, vocal folds resting posture. (D) Six weeks post-surgery, vocal folds adducted posture.
Patient remained severely symptomatic from her profound lingual tonsil hypertrophy and was subsequently taken for lingual tonsillectomy given airway and concerns for possible lymphoproliferative disease. The patient was intubated via an awake fiberoptic intubation due to the degree of supraglottic obstruction. Intraoperative findings demonstrated remarkably enlarged lingual tonsils with hypertrophy extending from the mid-tonsillar fossae inferior to the epiglottis with complete effacement of the vallecula and distortion of the epiglottis and surrounding laryngeal anatomy. A hybrid transoral approach using first the Crowe–Davis retractor followed by a Lindholm laryngoscope with carbon dioxide laser allowed complete removal of the lingual tonsils from their superior to inferior extent (Figure 3). A deformed and malacic epiglottis remained requiring epiglottopexy. Pathology showed follicular hyperplasia, no carcinoma or evidence of lymphoproliferative disorder. Operative cultures grew mixed oropharyngeal flora including light Fusobacterium growth. Four weeks after surgery, the patient presented with improved voice and swallowing, with resolution of snoring, shortness of breath, and neck swelling.
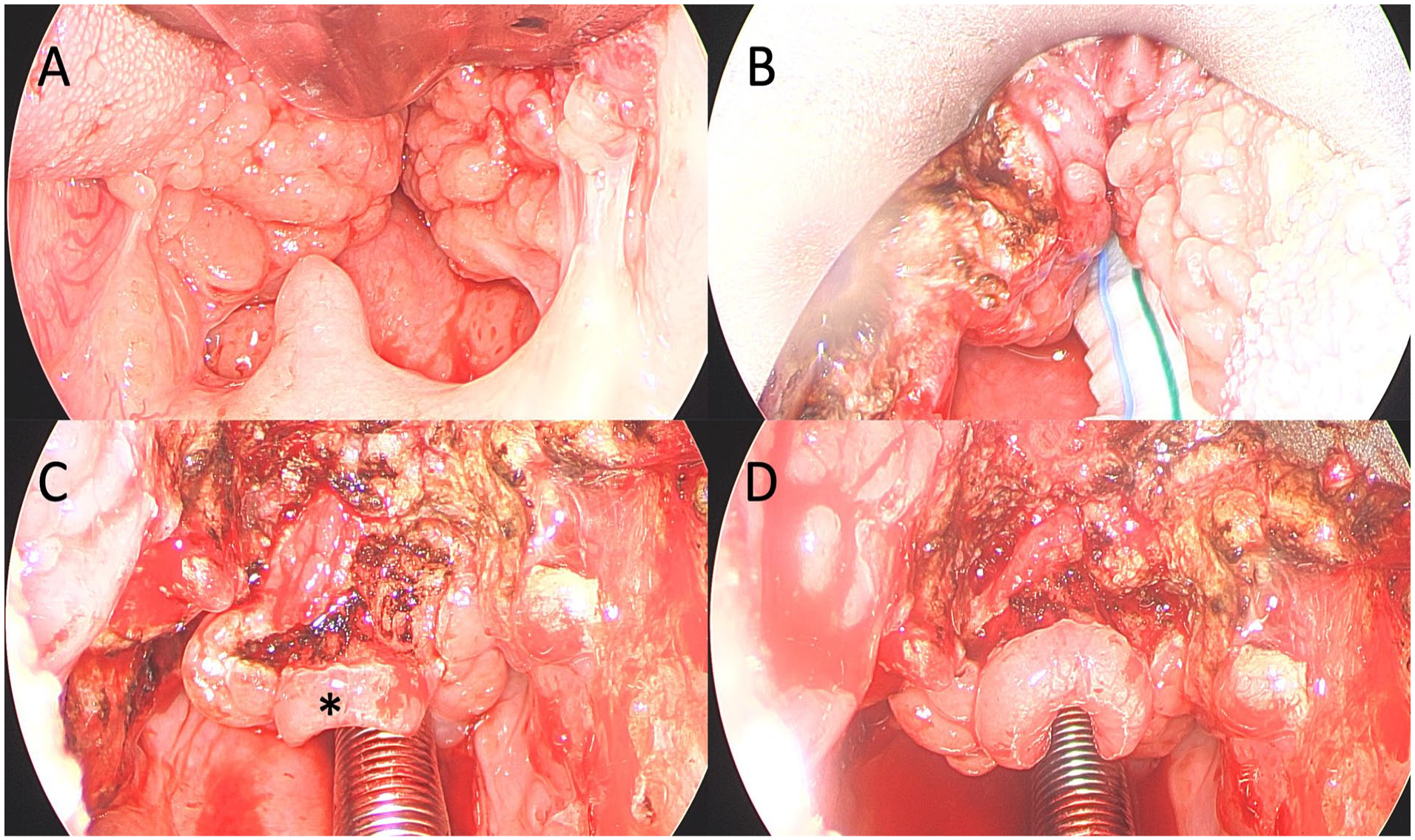
Surgical views from lingual tonsillectomy. (A) Oropharyngeal view using Crowe–Davis retractor, showing superior extent of lingual tonsils all the way to mid-tonsillar fossae. (B) Oropharyngeal view using Lindholm laryngoscope. Cottonoid is seen covering the laser safe endotracheal tube. (C) Defect after lingual tonsillectomy showing retroflexed epiglottis (*). (D) Final operative image following epiglottopexy anteriorly.
Gonorrhea is the second most common sexually transmitted infection in the United States. The number of reported cases of gonorrhea has continued to rise, with an increase of 25.4% from 2017 to 2021. 1 Adolescent and young adults between 15 and 29 years of age account for most new cases. 1 The most important risk factor for developing oral gonococcal infection is practicing oral sex.1,2 Gonococcal tonsillitis has been well described as a form of oral gonococcal infection with a wide range of symptomatology; some patients may remain asymptomatic, 64% present with sore throat, and 21% present with whitish-yellow exudates. 2 Cervical lymphadenopathy and fever are less common while tonsillar hypertrophy has not been previously described. 2 The treatment of oral gonorrhea involves a single intramuscular injection of ceftriaxone, rarely or if ever requiring surgical intervention.
There was a previous case of a 25-year-old homosexual male in which sore throat, exudate, and cervical lymphadenopathy resolved with ceftriaxone. His tonsils remained slightly enlarged but no further intervention was required. 2
Fusobacterium is a known colonizer of the human oropharynx. It has also been identified in cases of acute pharyngitis and associated with both tonsil hypertrophy and chronic tonsillitis syndromes.3,4 Its significance in this case is uncertain and additional research in this field is needed. Based on the acuity of her presentation, it is most plausible that acute gonococcal pharyngitis was her inciting event, leading to profound refractory lingual tonsillar hypertrophy.
There are many potential causes of lingual tonsil hypertrophy including infections and a compensatory hyperplasia after palatine tonsillectomy, both applicable to our patient. 5 Given the persistent and symptomatic lingual tonsil hypertrophy in our patient despite medical therapy and observation, a lingual tonsillectomy requiring a hybrid transoral approach was performed. 2 In addition, given the profound degree of tonsil hypertrophy within Waldeyer’s ring in this young otherwise healthy patient, there was a real concern for a possible lymphoproliferative disease. These factors supported surgical intervention both for symptomatic relief and for diagnostic clarity. This case highlights the importance of performing a comprehensive sexual history and keeping a broad differential for sexually active patients with laryngeal symptoms. It also highlights that antibiotics alone might not be enough to resolve symptoms and the considerations that are made for surgical intervention in these persistently symptomatic patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.