
Abstract
Keywords
Introduction
Glottic incompetence caused by unilateral vocal fold paralysis (UVFP) exerts a significant impact on patient quality of life due to varying degrees of dysphonia and an increased risk of aspiration. Among the most common surgical treatments are type I (medialization) thyroplasty (MT), injection laryngoplasty (IL), and arytenoid adduction (AA). MT, developed by Isshiki et al., 1 is considered the gold standard treatment for UVFP and involves medialization of the vocal fold with an implant inserted via the thyroid cartilage. IL, introduced by Brunings, 2 corrects glottic incompetence by administering an injection of filler material into the vocal fold or paraglottic space; autologous fat has become a popular injection material since Mikaelian et al. 3 first described their procedure for autologous fat injection laryngoplasty (FIL). AA, also developed by Isshiki et al., 4 involves rotation of the arytenoid cartilage of the paralyzed vocal fold using a suture placed in the muscular process, reducing the glottal-level difference during phonation caused by UVFP. AA is often combined with MT, but it can also be performed as a standalone procedure. Although each of these procedures is reported to be effective for UVFP, few studies have directly compared their effectiveness, and there is no definitive consensus on the optimal procedure.
In a previous study, 5 we compared MT and FIL based on aerodynamic and acoustic outcomes at 1 month posttreatment and observed no significant difference between the 2 groups. Although the surgical approaches are quite different, both procedures adhere to the same concepts to complete the glottal closure by medializing the vocal fold. On the other hand, AA has a different concept to reduce the glottal-level difference by rotating the arytenoid cartilage.
In the current study, we aimed to compare background characteristics and treatment outcomes between patients who underwent MT or FIL and those who underwent AA.
Patients and Methods
This clinical study was approved by the Ethics Committee of Osaka Kaisei Hospital (identification number: 22-10).
Diagnosis
The degree of glottic incompetence, glottal-level difference, and passive movement of the arytenoid on the paralyzed side were assessed via laryngoscopic observation. 6 Computed tomography (CT) was performed to determine the arytenoid’s location and passive movement and to assess glottal-level differences during phonation. Surgical treatment was indicated 6 to 12 months after UVFP onset 7 or when recovery of motion was definitively not expected (surgical recurrent nerve sacrifice or malignant invasion). 8
Patients
Among 375 patients with UVFP, 135 underwent phonosurgery at the Osaka Voice Center of Osaka Kaisei Hospital from January 2009 to February 2013. All patients underwent MT, FIL, AA with MT, or AA alone. Surgical treatment options, as well as their advantages and disadvantages, were presented to each patient per the recommendation of the senior author, who has performed more than 100 laryngoplasties (R.M.). After explanation, patients chose which procedure to receive. From diagnosis made by endoscopic examination and CT, MT or FIL was offered to patients with mild glottal incompetence and seemed to have no glottal-level difference, and AA with MT or AA alone was recommended to patients with severe glottal incompetence and/or has glottal-level difference.
The inclusion criteria for this study were as follows: (1) no history of previous phonosurgery, and (2) available functional evaluations before and after surgery. Consequently, 87 patients (44 men and 43 women, median age 65 years, and range 17-86 years) were enrolled in this study. MT, FIL, AA with MT, and AA alone were performed in 12, 31, 38, and 6 patients, respectively. We sorted the former 2 surgical treatments into the thyroplasty (TP) group and the latter 2 into the AA group. Table 1 presents the background characteristics for the study population. Although we observed significant differences in age and etiology between the groups, there were no significant between-group differences in sex or the side of paralysis.
Patient Background Characteristics.
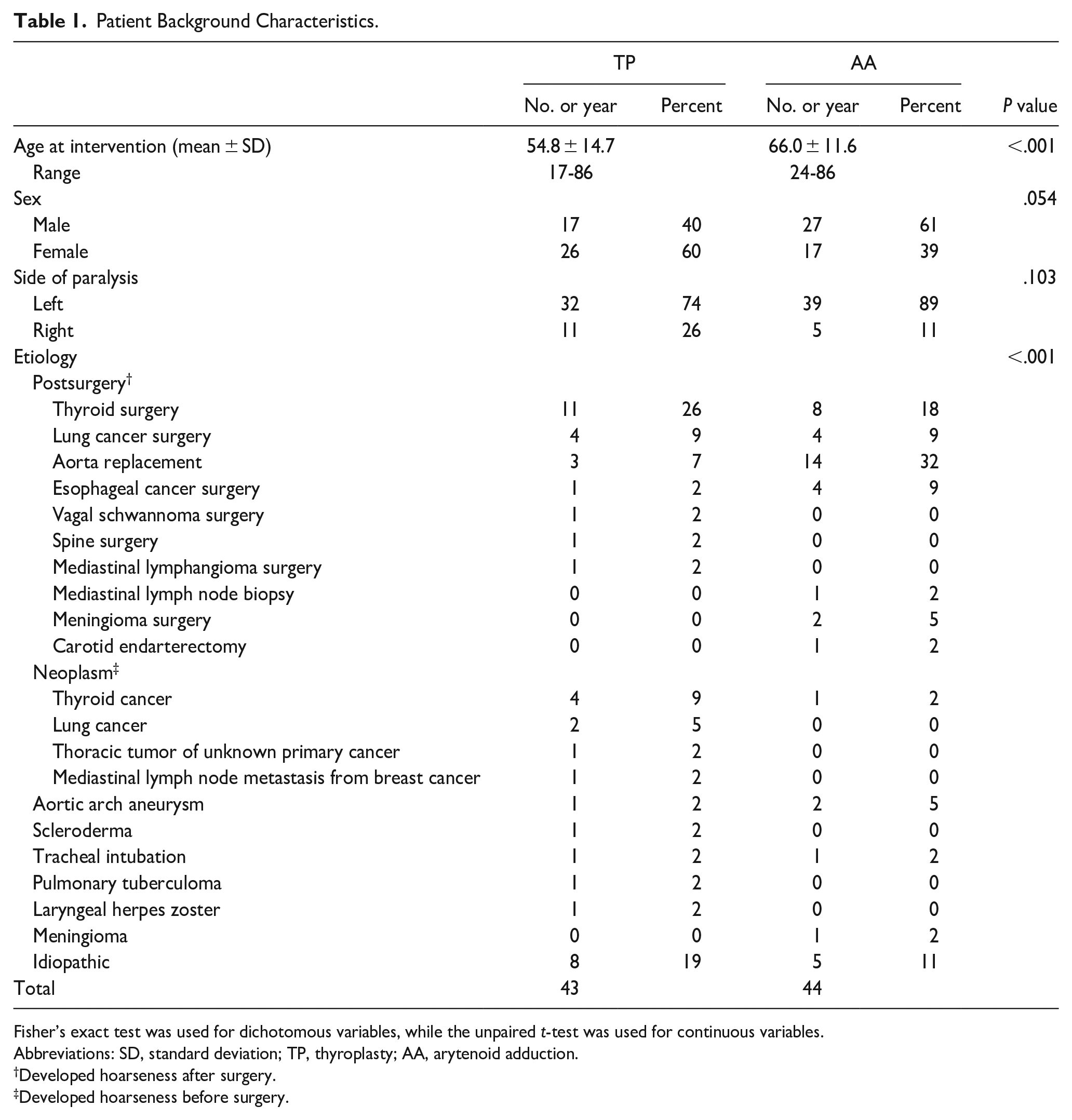
Fisher’s exact test was used for dichotomous variables, while the unpaired t-test was used for continuous variables.
Abbreviations: SD, standard deviation; TP, thyroplasty; AA, arytenoid adduction.
Developed hoarseness after surgery.
Developed hoarseness before surgery.
Surgery
MT was performed in the operating room under local anesthesia as described previously. 5 Hydroxyapatite (block-like implant) was used as an implant in 10 patients and expanded polytetrafluoroethylene (ePTFE; Gore-Tex®; W. L. Gore & Associates, Inc., Flagstaff, AZ, USA) was used in 2 patients. The insertion technique did not differ according to the type of implant used. FIL was performed in the operating room under general anesthesia as described previously. 5 Autologous fat was used as the injection material in all cases. AA was performed in the operating room mainly under general anesthesia without intubation by total intravenous anesthesia and monitored anesthesia care. Propofol was used as the sedative, and we monitored the depth of anesthesia and preserved spontaneous breathing, also using high flow nasal cannula as a support. One patient underwent tracheotomy because considering the patient’s small mandible and narrow pharynx, we assumed that we could not maintain the airway without intubation or tracheotomy during general anesthesia. Local anesthesia was used solely in another patient.
As described by Isshiki et al., 4 the incision line was made horizontally at the midline level of the superior and inferior thyroid notches. The subplatysmal flap was elevated, and the lateral border of the strap muscles was dissected from the anterior border of the sternocleidomastoid muscle. After rotating the thyroid cartilage medially and anteriorly, the inferior constrictor was dissected along the edge of the thyroid lamina. The muscular process of the arytenoid became palpable after separating the mucosa of the pyriform sinus from the thyroid cartilage. Thyroid cartilage was not removed to expose the muscular process. A 4-0 nylon suture was then tied through the muscular process. The other end of the suture was pulled anteroinferiorly and fixed to the thyroid cartilage to simulate the contraction of the lateral cricoarytenoid muscle, thus controlling the position of the arytenoid and reducing the glottal-level difference and horizontal glottic incompetence.
After AA, additional MT was performed. Hydroxyapatite was used as the implant material in 28 patients, while ePTFE and a silicon block were used in 9 patients and 1 patient, respectively. The insertion technique did not differ according to the type of implant used.
Follow-Up
The following voice parameters were evaluated in all patients just before, approximately 1 month after surgery. Several patients were able to evaluate 6 months after surgery. For each patient, maximum phonation time (MPT) was recorded as the longest duration of phonation when producing a vowel sound (/a/) at a comfortable pitch and loudness level across 3 efforts. Acoustic voice analysis was performed using the Multi-Dimensional Voice Program (KayPentax, Lincoln Park, NJ, USA). All tests were performed in a quiet room with a mouth-to-microphone distance of 10 cm. Analysis was performed for a sustained vowel sound (/a/) produced at a comfortable pitch and intensity level based on the following parameters: pitch period perturbation quotient (PPQ), amplitude perturbation quotient (APQ), and harmonic-to-noise ratio (HNR), which was converted from the noise-to-harmonic ratio (NHR) using the following formula:
Details regarding these acoustic parameters have been described previously. 5
Statistical Analyses
The Wilcoxon signed-rank test was used to compare pre- and posttreatment voice changes within each of the treatment groups. The Mann-Whitney U-test was used to compare pre- and posttreatment parameters between the 2 groups. The Bonferroni correction was performed for the post hoc analysis, and the P values mentioned in the results are corrected P values. Corrected P values were rounded to 1 when they were over 1. 9 When comparing background characteristics, Fisher’s exact tests were used for dichotomous variables, whereas unpaired t-tests were used for continuous variables. IBM SPSS version 25 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. The level of statistical significance was set at a 2-sided P value of <.05.
Results
In the pretreatment acoustic analysis, parameters were not obtained from 6 patients in the TP group and 13 patients in the AA group due to severe hoarseness. Posttreatment function was evaluated approximately 1 month (range 13-45 days) and 6 months (range 108-244 days) after surgery.
Preoperative Parameters
Table 2 shows the values of functional parameters obtained immediately before surgery. Before surgery, voice quality was significantly worse in the AA group than in the TP group for all aerodynamic and acoustic measures.
Pretreatment and Posttreatment Functional Parameters.
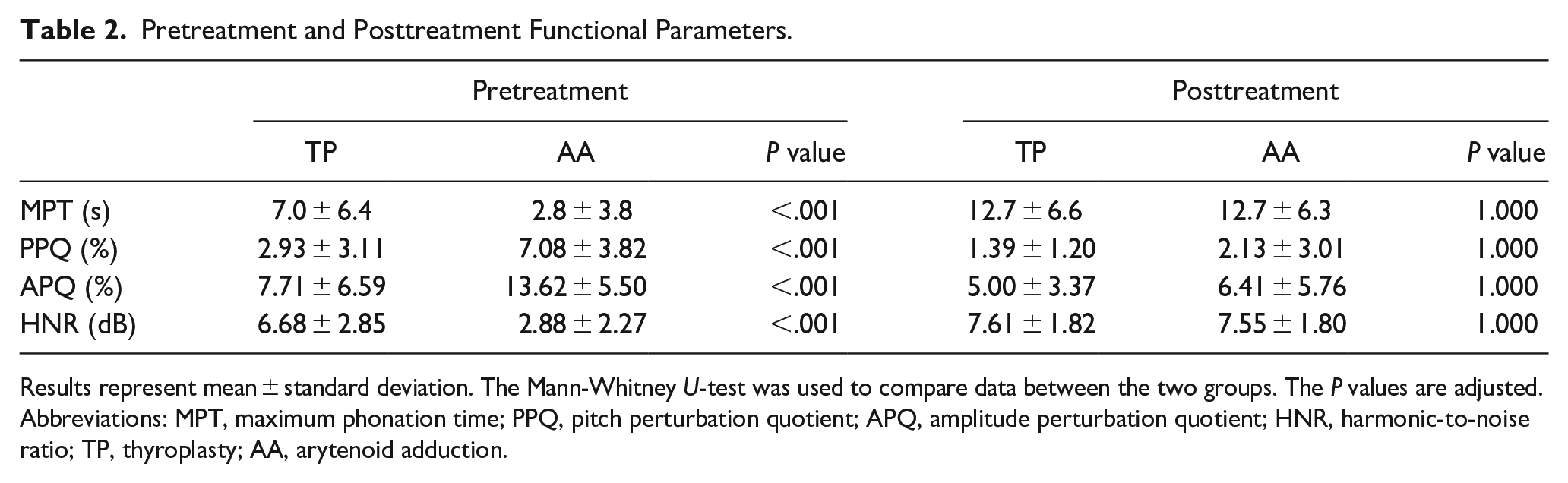
Results represent mean ± standard deviation. The Mann-Whitney U-test was used to compare data between the two groups. The P values are adjusted.
Abbreviations: MPT, maximum phonation time; PPQ, pitch perturbation quotient; APQ, amplitude perturbation quotient; HNR, harmonic-to-noise ratio; TP, thyroplasty; AA, arytenoid adduction.
TP Group Postoperative Outcomes at 1 Month
As shown in Figure 1A, TP yielded a significant improvement (increase) in MPT (s) (pretreatment: 7.0 ± 6.4 (mean ± standard deviation), posttreatment: 12.7 ± 6.6, P < .001) in 43 patients with UVFP 1 month after surgery. In the 37 patients from whom we were able to obtain pretreatment acoustic parameters, PPQ (%) (pretreatment: 2.93 ± 3.11, posttreatment: 1.39 ± 1.20, P = 0.012) significantly improved (decreased) after treatment. Although changes in APQ (%) (pretreatment: 7.71 ± 6.59, posttreatment: 5.00 ± 3.37, P = .195) and HNR (dB) (pretreatment: 6.68 ± 2.85, posttreatment: 7.61 ± 1.82, P = .678) were not significant, a clear trend toward improvement (decrease in APQ and increase in HNR) was observed.
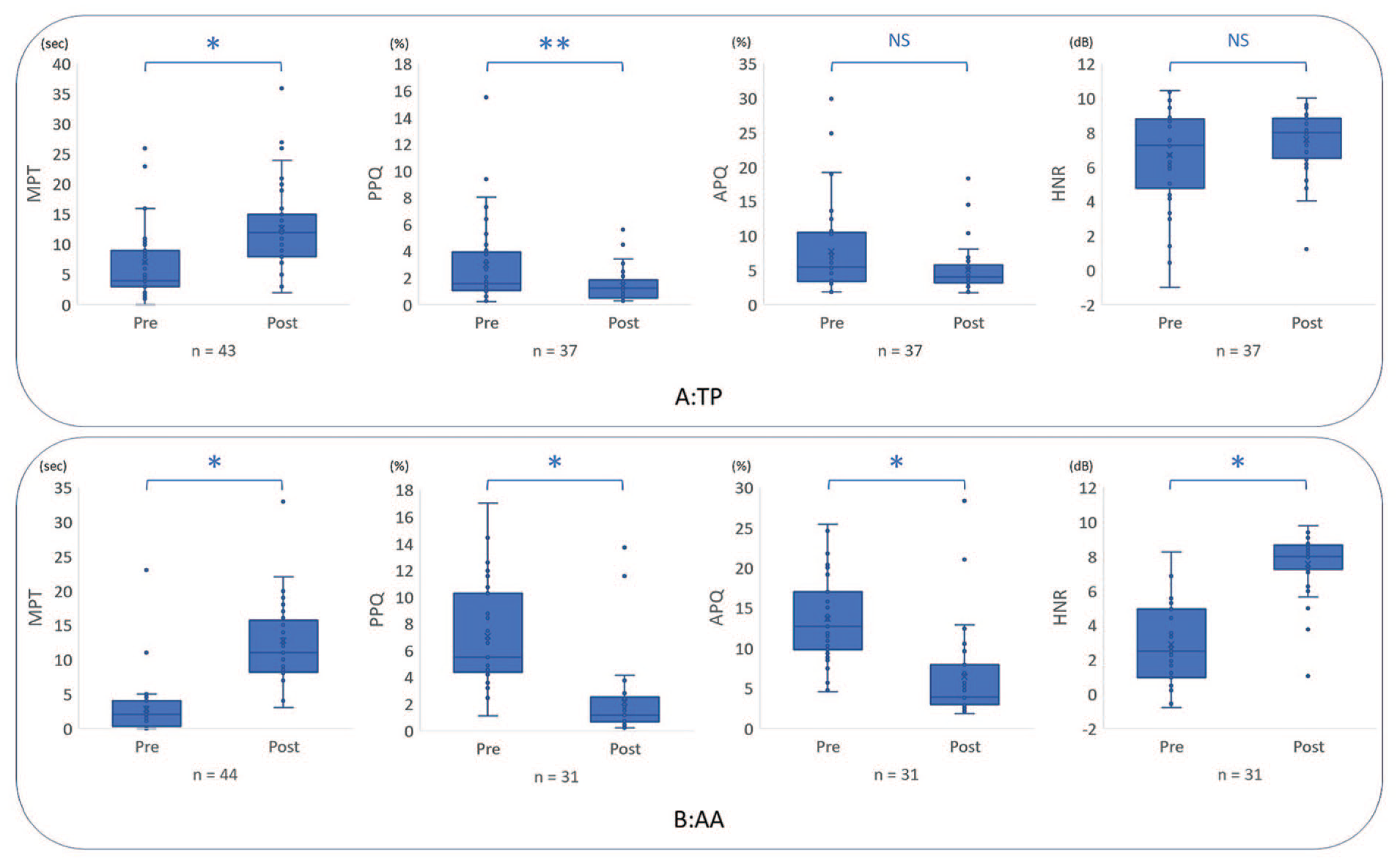
Changes in aerodynamic and acoustic parameters 1 month after surgery.
AA Group Postoperative Outcomes at 1 Month
As shown in Figure 1B, AA yielded a significant improvement (increase) in MPT (s) (pretreatment: 2.8 ± 3.8, posttreatment: 12.7 ± 6.3, P < .001) in 44 patients with UVFP 1 month after surgery. Among the 31 patients from whom we were able to obtain pretreatment acoustic parameters, we observed significant improvements in PPQ (%) (pretreatment: 7.08 ± 3.82, posttreatment: 2.13 ± 3.01, P < .001), APQ (%) (pretreatment: 13.62 ± 5.50, posttreatment: 6.41 ± 5.76, P < .001), and HNR (dB) (pretreatment: 2.88 ± 2.27, posttreatment: 7.55 ± 1.80, P < .001) (decreased PPQ and APQ and an increase in HNR) after treatment.
Postoperative Parameters at 1 Month
Table 2 also shows the comparison of functional parameters between the groups 1 month after surgery. There were no significant differences in any of the aerodynamic or acoustic measures between the 2 groups.
Postoperative Parameters at 6 Months
At 6 months after surgery, MPT (s) were obtained in 16 and 34 patients from TP and AA groups, respectively (pretreatment: 6.2 ± 8.5 vs 3.2 ± 4.2, posttreatment 1 month: 11.8 ± 9.2 vs 11.8 ± 4.7, posttreatment 6 months: 10.1 ± 2.8 vs 9.8 ± 6.0). Of those patients, acoustic parameters were managed to obtain in 13 and 23 cases in TP and AA groups, respectively [PPQ (%), pretreatment: 3.52 ± 1.12 vs 7.19 ± 4.11, posttreatment 1 month: 2.60 ± 0.88 vs 2.05 ± 2.78, posttreatment 6 months: 2.26 ± 0.20 vs 1.95 ± 2.09; APQ (%), pretreatment: 5.49 ± 4.67 vs 13.42 ± 5.56, posttreatment 1 month: 3.31 ± 3.76 vs 6.71 ± 6.30, posttreatment 6 months: 2.44 ± 2.76 vs 6.46 ± 6.76; HNR(dB), pretreatment: 7.07 ± 2.45 vs 2.95 ± 2.22, posttreatment 1 month: 7.78 ± 1.25 vs 7.64 ± 1.90, posttreatment 6 months: 8.58 ± 0.28 vs 7.68 ± 2.24]. Although the sample size at 6 months after surgery was too small and limited to conduct a meaningful statistical analysis, a clear trend of improvement maintaining from the first month was observed.
Discussion
In this study, we compared vocal outcomes 1 month following phonosurgery for UVFP between patients in the TP and AA groups. Our analysis indicated that surgeries in both the TP and AA groups were effective in treating UVFP. Although preoperative parameters were worse in the AA group than in the TP group for all aerodynamic and acoustic measures, there were no significant differences between the groups after treatment. These results are in accordance with the results described in a previous report. 10 Moreover, some patients were able to follow up until 6 months after surgery. Although the data were limited to conduct a meaningful statistical analysis, they showed clear trend of voice recovery until 6 months. In addition, previous studies have demonstrated that the surgical effects of MT or FIL on vocal recovery observed within the first postoperative month can last up to 6 months or even longer,11-14 and surgical effects of AA on vocal recovery at the postoperative third to sixth month could last a year.15,16 Given these findings, the patients included in the current study were likely to experience long-term favorable outcomes.
The TP group demonstrated significant improvements in MPT and PPQ but not in APQ or HNR. MPT is the parameter most frequently used for vocal evaluation and has been identified as a significant indicator of postoperative vocal outcomes. 17 The mean flow rate (MFR) is also a useful aerodynamic variable; however, we were able to evaluate MFR or lung capacity data from only a few patients in this study. Differences in the characteristics and methods used to calculate the 3 acoustic parameters (PPQ, APQ, and HNR) may explain the discrepant findings for each parameter, as noted in our previous report. 5 Additionally, the value of existing acoustic parameters as an index of therapeutic effect has been questioned. 18 Furthermore, the methods used to evaluate these parameters are limited, as inaccuracies and failures in frequency detection can occur depending on the type of voice analyzed. 19 The widespread use of more practical theories and devices, such as cepstral peak prominence, is desired.20-22
Due to severe hoarseness, pretreatment acoustic analysis was infeasible in 6 TP group patients and 13 AA group patients. Thus, voice quality was worse in these patients than in others, to the extent that the fundamental frequency could not be detected or measured. This difference in the number of patients corresponds to the finding that pretreatment parameters were worse overall in the AA group than in the TP group, as shown in Table 2. Voice quality improved to the point that postoperative acoustic analysis was possible, indicating surgical treatment for UVFP was effective for both groups. Our analysis indicated MPT improved in all 19 patients, further highlighting the effectiveness of treatment, and the mean MPT did not differ between the TP and AA groups before or after treatment (pretreatment: 2.8 seconds vs 1.3 seconds, posttreatment: 10.3 seconds vs 11.2 seconds).
This study had 3 major limitations. First, the follow-up period was relatively short. Although all patients were encouraged to return for follow-up examinations, patients in good condition tended not to return after a long period. Studies with longer follow-up periods will be conducted in the future. Second, the study was not designed as a randomized controlled study but as a retrospective case–control study. Therefore, there were significant differences in demographic characteristics between the groups, such as age and etiology, as shown in Table 1. This also resulted in differences in the number of patients between the groups. Third, the patients selected which procedure to undergo based on the recommendations of the senior author, which may have introduced bias. In fact, patients with glottal-level differences mainly underwent AA with MT or AA alone, whereas others underwent MT or FIL alone. Despite these limitations, no significant differences in posttreatment parameters were observed between the TP and AA groups, indicating that surgical selection was appropriate.
As shown in Table 1, the main causes of UVFP were thyroid disease (thyroid surgery or thyroid cancer) in the TP group and aortic aneurysm (aortic replacement or aortic aneurysm) in the AA group. Upon sampling patients with thyroid disease from the TP group and patients with aortic aneurysm from the AA group, the results of MPT did not differ from those observed for the overall population [pretreatment: 7.8 ± 7.4 vs 1.9 ± 2.8 (mean ± standard deviation), posttreatment: 12.9 ± 5.5 vs 11.9 ± 6.3]. Furthermore, although there were only 4 patients with aortic aneurysm in the TP group, voice quality in these patients did not significantly change after MT or FIL [MPT, pretreatment: 11.3 ± 5.9 (mean ± standard deviation), posttreatment: 12.3 ± 3.8; PPQ, pretreatment: 1.69 ± 1.51, posttreatment: 1.19 ± 0.53; APQ, pretreatment: 6.49 ± 4.72, posttreatment: 4.28 ± 1.83; HNR, pretreatment: 7.00 ± 2.54, posttreatment: 7.60 ± 1.14]. Among these patients, 2 patients who had severe glottal incompetence or glottal-level difference preferred FIL over AA for less invasive treatment, whereas the other 2 patients had almost no glottal-level differences or had good indications for FIL. In addition, although most of patients followed the surgical selection principle mentioned in “Patients and Methods” section and had a good result, few patients with glottal-level difference in CT underwent MT or FIL because of the mild glottal incompetence or the patients’ preference (mainly for less invasive treatment). Of those patients, most of their voices improved after surgery, but only 1 patient did not improve postoperatively, and his etiology was aortic aneurysm. These findings also indicate surgical selection was appropriate in each case, even when based on the patient’s etiology. This may aid in the selection of the appropriate surgical treatment for UVFP. For example, if the glottal-level difference during phonation is unclear, and it is difficult to determine whether AA or TP is appropriate, or when patients are wondering which surgery to choose, it may be possible to recommend treatment by referring to the patient’s etiology.
Although currently there are no international evidence-based guidelines concerning surgical treatment for UVFP, our findings may aid in surgical decision-making for these patients. Nonetheless, further studies with more precise sampling methods and randomized trials are required to confirm this hypothesis.
Conclusion
The current findings indicate that both TP and AA were effective for voice recovery in patients with UVFP under appropriate surgical selection. Our results also highlight the importance of preoperative evaluation and the potential value of etiology for selecting the appropriate procedure.
Footnotes
Acknowledgements
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by JSPS KAKENHI Grant (2020-2022), AMED under Grant Number 18dk0310092h000a, and Health and Labour Sciences Research Grant for Research on Rare and Intractable Diseases (R02-Nanchito (Nan)-Ippan-04) from the Ministry of Health, Labour, and Welfare of Japan.