
Abstract

Significance Statement
The monkeypox virus (MPXV) outbreak has spread worldwide. Clinical features may differ from the West African disease and be misleading. The community of men who have sex with men (MSM) appears to be at higher risk. Alerting the various practitioners who may encounter infected patients is necessary to prevent the spread of the disease. Rare and severe presentations in the pharynx and larynx have been described. However, a more common mild pharyngeal presentation should not be neglected.
Presentation of 2 Cases and Discussion
We report here the cases of 2 pharyngeal presentations of MPXV-positive patients with confirmed transmission through oral sex. The study was approved by the Foch IRB: IRB00012437 (approval number: 22-10-01) on October 6, 2022. Informed consent was obtained from the 2 patients. Patient 1 was an HIV-positive MSM. He presented with a history of unprotected oral sex and developed a sore throat within 72 hours. On physical examination, he displayed a single nodular lesion on the posterior pharyngeal wall (Figure 1) and an isolated skin papule in the right inguinal region. The pharyngeal lesion was borderless, flat, and painless and was considered to be the inoculation lesion. The description did not correspond to a syphilis canker. The diameter was approximately 2 cm. No skin rash appeared. Neither the partner nor his outcome was known. Real-time RT-PCR of swabs from the inguinal and pharyngeal lesions was positive for MPXV. Patient 2 was an HIV-negative MSM and presented for vaccination. He reported a history of sore throat 10 days prior to the consultation, treated with corticosteroids by his general practitioner within the context of a concomitant rash attributed to mosquito bites. He had unprotected oral sex with an unknown partner. On examination, the pharynx was inflamed with an enlarged right tonsil (Figure 2). A swab was taken from the right tonsil, and MPXV RT-PCR was positive, as were the visible skin lesions sampled.
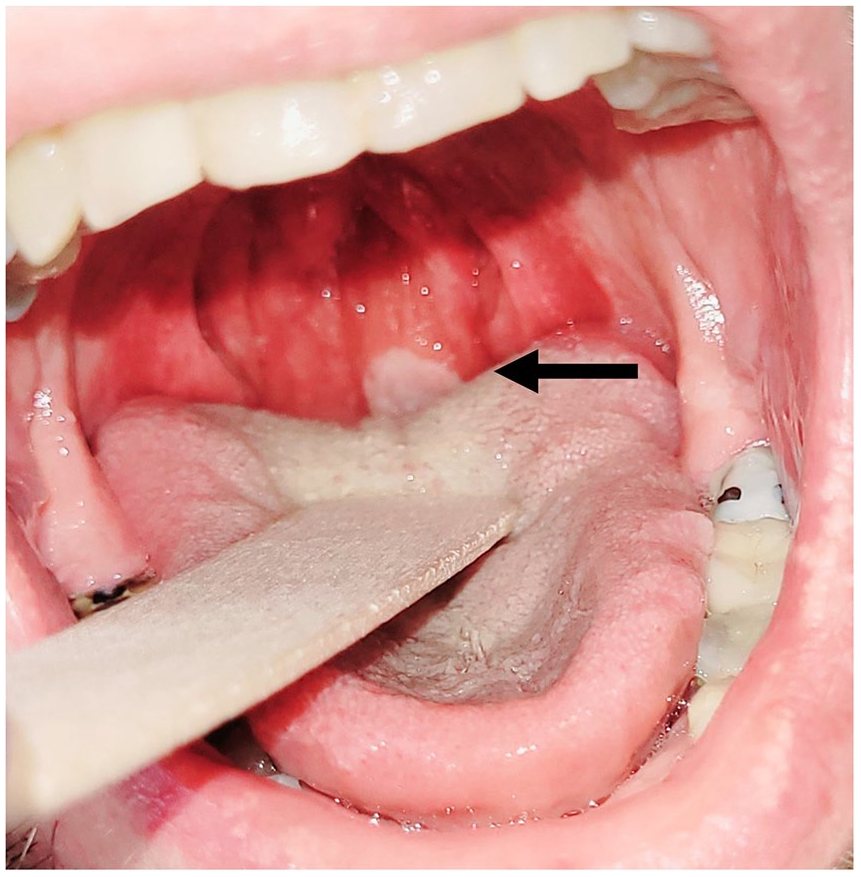
Patient 1’s nodular lesion on the posterior pharyngeal wall (arrow). Possible inoculation lesion of oral sexually transmitted monkeypox. The swab was RT-PCR positive.
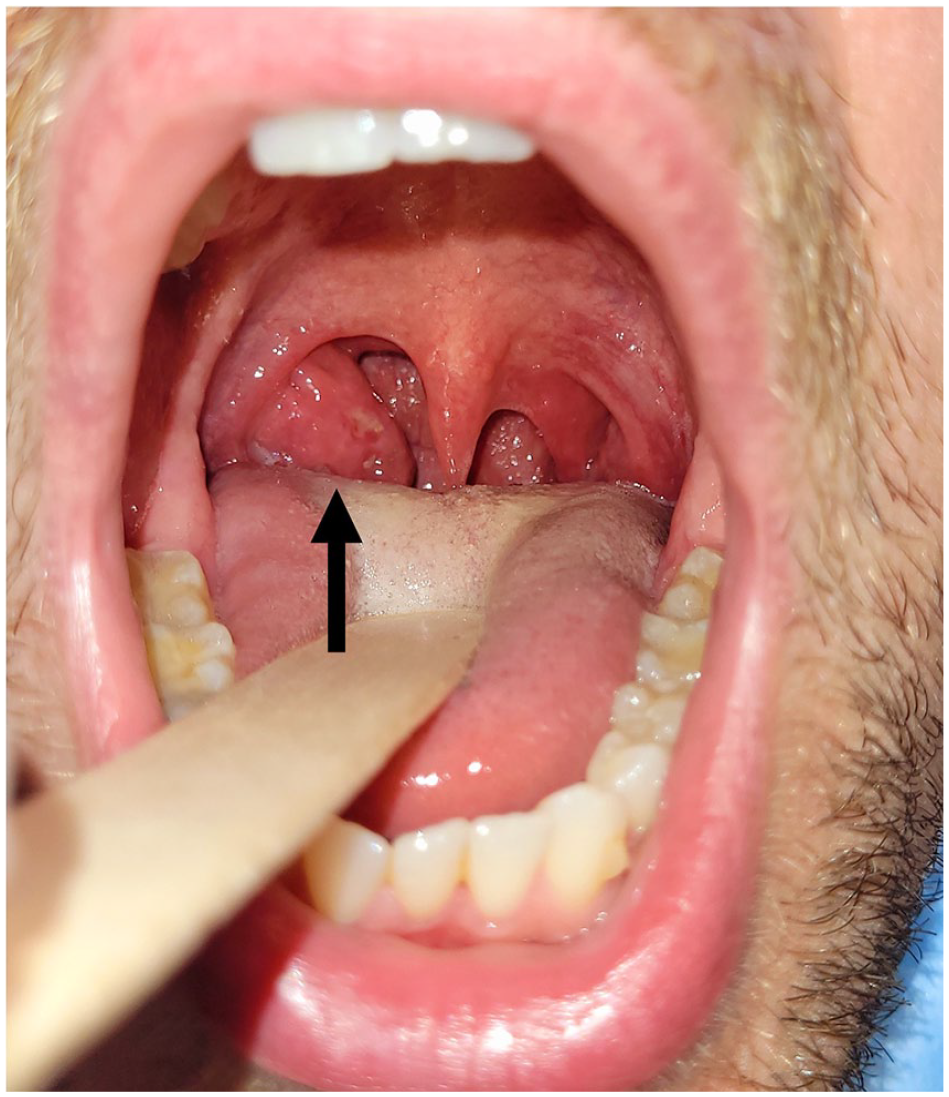
Patient 2’s enlarged right tonsil (arrow) in erythematous angina with rash after oral sexually transmitted monkeypox. The swab of the right tonsil was RT-PCR positive.
We report 2 examples of pharyngeal lesions after stated oral sexual transmission. Both presentations and the sexual nature of their transmission deserve to be quickly brought to the attention of our ENT colleagues and general practitioners.1,2 MPXV is transmitted through contact between humans. Incubation lasts less than 3 weeks but can be significantly shorter if the contact is highly positive. Vesicles may involve the palms, face, and genitals, which can be considered the site of inoculation, followed by the arms and entire body. Oropharyngeal MPXV lesions remain scarcely described, but they are not infrequent.3,4 Tarìn-Vicente et al 4 found N = 78 (43%)/181 patients with such lesions described, but presentations can be misleading, and an MPXV-positive “common sore throat” may be neglected. Diagnosis is made by real-time RT-PCR of swabs. Skin lesions are the most appropriate site to test for MPXV. 5 Pharyngeal lesions appear to be a reliable test site, but care must be taken with regard to how the swab is obtained from this area, that is, on a visible lesion versus random swabbing of the tonsils. 6 The differential diagnosis is oropharyngeal syphilis with a painless tonsillar ulcer and progressive enlargement of the cervical lymph node. Syphilis is a widespread infection with increasing frequency, particularly among MSM, but the systemic and cutaneous lesions occur years months after the canker. Previous studies have detected heterosexual men with MPXV.4,5 Thus, we urge vigilance when examining unusual acute pharyngeal lesions in any person, especially when pharyngeal lesions are associated with systemic symptoms. An important need is the possible development of rapid pharyngeal tests for ENT professionals combined with information on the recognition and management of MPXV. The MPXV outbreak is becoming an urgent public health issue; such presenting signs should prompt the consideration of MPXV, even in patients outside of the MSM community, for rapid identification so as to contain its spread.
Footnotes
Author Contributions
Baudouin: Concept, design, analysis. Vallée: Concept, design, analysis. Zucman: Concept, design, analysis. Hans: Concept, design, analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Foch IRB: IRB00012437 (approval number: 22-10-01) on October 6, 2022. Willing consent was obtained from the 2 patients.