
Abstract
We report a case of a 6-month-old male that presented with wound dehiscence, in part due to mechanical tongue trauma, following bilateral cleft lip repair. A silastic sheeting dressing with retention sutures was uniquely fashioned to decrease wound tension and protect the surgical site from patient interference. This solution may potentially be used in similar circumstances.
Keywords
Introduction
Cleft lip (CL) results from failure of fusion of the medial nasal prominence and the maxillary prominences. 1 Cleft palate (CP) is the failure of fusion of the palatal shelves of the maxillary processes, resulting in a cleft of the hard and/or soft palates. 1 Surgical treatment for CL/P generally includes surgery for cleft lip repair between 2 and 3 months of age for unilateral cleft lip and 3-6 months for bilateral cleft lip, and surgery for cleft palate repair between 10 and 12 months of age. 2 Postoperative complications of cleft lip and palate repair can include wound dehiscence, in this case with patient interference disrupting the tight wound closure. This complication is particularly concerning because it requires reoperation. 3 Effective prevention of postoperative wound dehiscence includes maintenance of an optimal healing environment and protection from external factors. 4
Case Report
An infant male presented with a bilateral cleft lip and palate that was wide with very protuberant premaxilla. The patient had a maternal family history of cleft palate. Presurgical taping was performed due to lack of access to nasoalveolar molding (NAM) and was successful in improving the width of the cleft lip and protuberance of the premaxilla somewhat. At age 6 months, the patient was brought to the operating room for bilateral cleft lip repair and did well initially postoperatively.
One week postoperatively, the patient’s mother noted that a structure of the vermillion appeared disconnected, initially presenting after bottle feeding. A photo taken by the patient’s mother at this time appeared to show detachment of Dermabond glue (Figure 1). A subsequent lateral view photo showed potential dehiscence of the vermillion. Dermabond was removed in the emergency room, and visualization confirmed surgical site dehiscence and epidermolysis of the skin over the incision site in the prolabial segment. Revision cleft lip repair the following morning was successful, and Dermabond was reapplied. Images taken one week status post primary cleft lip repair by patient’s mother, demonstrating detachment of Dermabond glue and findings concerning for surgical site dehiscence.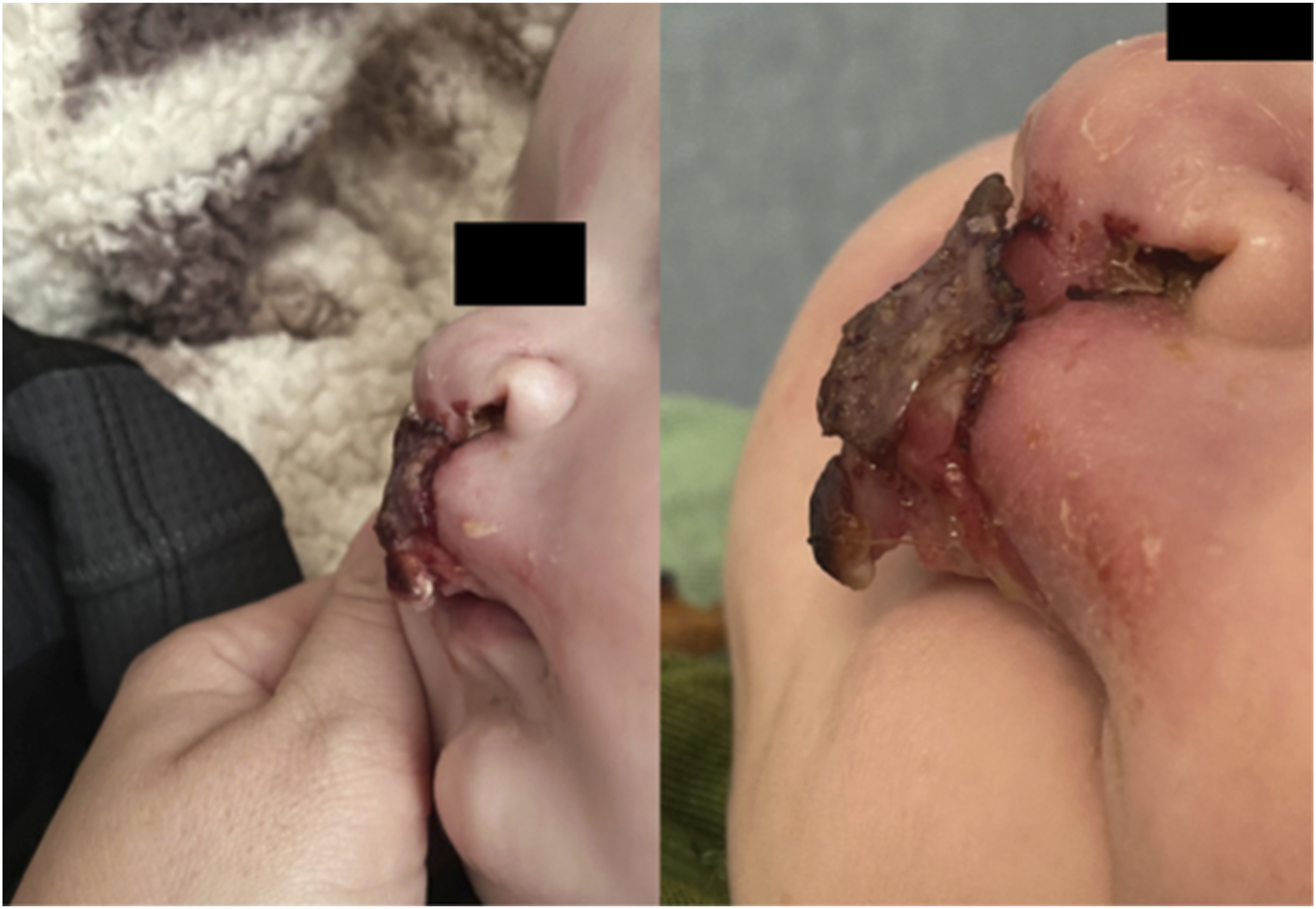
One day status post revision cleft lip repair, the patient’s mother noticed recurrent detachment of Dermabond, potentially secondary to patient interference with repetitive licking of the surgical site. Steri-strips were applied two days later, but had fallen off by the following day. After a discussion with the patient’s parents including options of re-repair or letting the wound heal by secondary intention with delayed revision repair, a second revision cleft lip repair was agreed upon, two weeks after the initial repair.
Extensive manipulation of the surgical site after two surgeries and decreased availability of tissue at the vermillion presented increased risk for recurrent dehiscence. A retention suture type mechanism was needed to help decrease tension between the maxillary prominences and medial nasal prominences, and prevent patient manipulation. An apparatus using silastic sheeting was constructed, which was rolled underneath the vermillion and over the cutaneous lip, and held in place with 3-0 Prolene retention sutures through-and-through the vermillion (Figure 2). This was to serve as a physical barrier between the patient’s tongue and surgical site to facilitate wound healing. In addition, Xeroform gauze was tucked in under the silastic dressing over the area of epidermolysis. This apparatus was left in place for two weeks, was well tolerated, and presented no problems with feeding. Despite continued molestation of the surgical site from the patient’s tongue, the patient healed well with no recurrent complications. Images taken postoperatively following second revision cleft lip repair. (A) Taken immediately postoperatively, demonstrating silastic sheeting installed on the interior and exterior vermillion to prevent patient manipulation and facilitate wound healing. (B) Taken 6 months postoperatively, demonstrating well-healed surgical site.
Discussion
Cleft lip with or without cleft palate is the most common craniofacial malformation in newborns, affecting roughly 14.5 per 10,000 live births. 5 Primary cleft lip repair is often scheduled between 3 and 6 months of age and typically requires 3-4 months of presurgical manipulation to achieve its desired outcome. 3,6 Presurgical lip taping to better approximate the edges of the cleft, commonly referred to as “tissue creep,” can decrease risk of flap dehiscence, particularly in patients with wide bilateral clefts with protrusive premaxilla. 2 Nasoalveolar molding (NAM) can also be used to accomplish the same goal; however, this form of presurgical treatment is not always accessible. 7,8 In this case, surgery was scheduled at 6 months due to his prominent premaxilla and significantly wide gap.
A common postoperative complication of cleft lip repair is disruption of the sutures by the patient and is the reason why arm restraints may be recommended for infants postoperatively. 9 Though we do not routinely use arm restraints, we observed in this case that the patient’s tongue manipulation of the area may have contributed to repeated vermillion dehiscence. Thin sheets of silastic have previously been used during the nasal repair portion of cleft lip nasal deformity and have been useful in aiding surgical site healing, namely, via closing dead space and offering stability to the vermillion. 10 This case offers a new indication for such measures, namely, to serve as a physical barrier against molestation of the surgical site from the patient’s tongue, as well to hold a Xeroform dressing in place to further facilitate healing. This technique ultimately proved effective with this patient and may be considered in future similar patients as a prophylactic measure to avoid complications associated with revision procedures necessitated by dehiscence or other complications following primary repairs.
Conclusion
The patient in this case is an infant male with bilateral wide cleft lip and palate, with a significant alveolar gap and protruding premaxilla. Primary left lip repair was completed but was complicated by postoperative dehiscence. During revision surgery, it was determined that a normal operative procedure was not sufficient to prevent repeat dehiscence. As such, silastic sheeting was applied to the surgical site and held in place by retention sutures to take additional tension off the wound and to prevent patient interference in healing. This barrier was successful in facilitating the healing process in the patient, and may be worth considering in other cases with complicating anatomy such as wide alveolar gaps, or in the presence of other factors, such as patient interference, which may complicate healing and lead to similar complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report.