
Abstract
We report a case of a 63-year-old male who presented with synchronous pT1N1 p16-positive squamous cell carcinoma (SCC) of the left tonsil and pT4N0 p16-negative SCC of the left tongue.
Keywords
Introduction
Patients diagnosed with head and neck squamous cell carcinoma (HNSCC) are at an increased risk of developing second primary malignancies (SPMs). 1 It is estimated that synchronous SPMs of the head and neck arise in up to 6% of newly diagnosed HNSCC patients. 2 -4 Identification of these synchronous SPMs is significant, given that they can alter the patient’s treatment plan and surgical approach. Often, SPMs arise from a similar etiology (e.g., tobacco or human papillomavirus (HPV)). Here, we describe a unique case of synchronous HNSCCs with different etiologies.
Case Report
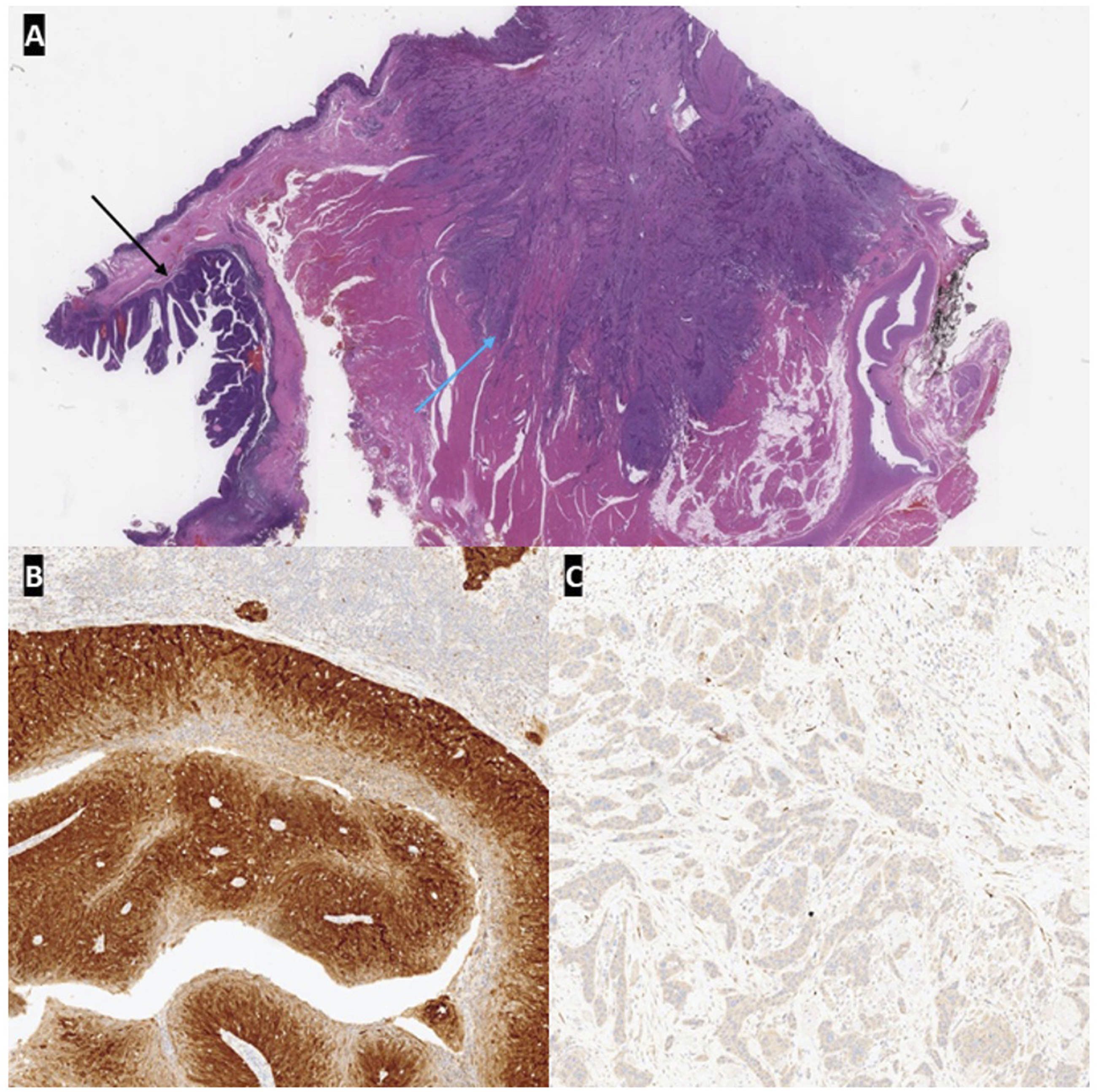
A 63-year-old non-smoker male with a past medical history of hypertension presented to the clinic with a 6-month history of tongue discomfort and a left posterior oral base of tongue sore. The tongue sore was biopsied and reported as a p16-negative keratinizing SCC. Upon exam, the patient had left hypoglossal nerve weakness and a firm submucosal mass in the left base of the tongue. Staging CT and PET scans revealed an intensely hypermetabolic 2.5 cm in the left base of the tongue and a left jugulodigastric lymph node, cT2N1M0 (Figure 1). The patient underwent a left partial glossectomy and oropharyngectomy (including the left base of tongue and left palatine tonsil), with left neck dissection and forearm flap reconstruction. Final pathology showed a p16-negative keratinizing SCC of the tongue with clear margins. Interestingly, microscopic examination of the ipsilateral palatine tonsil revealed an unexpected p16-positive non-keratinizing SCC (Figure 2). Two neck lymph nodes had metastatic p16-positive SCC. The patient was diagnosed with both a pT1N1 p16-positive SCC of the left tonsil and a pT4N0 p16-negative SCC of the left tongue in close proximity. Combined 18F-FDG PET/CT in the axial view. Intensely hypermetabolic mass in the left floor of the mouth and left posterior tongue (marked with white arrow in figures 1A and 1C), and borderline-sized left jugulodigastric lymph node with moderate hypermetabolism (marked by blue arrow in figures 1B, 1C, and 1D). (A) Photomicrograph showing the relationship between the p16-positive SCC (black arrow) involving the tonsil and p16-negative SCC (blue arrow) involving the tongue (H&E, 6x). (B) p16 immunohistochemical stain showing strong diffuse positivity in the tonsil SCC (80x). (C) p16 immunohistochemical stain showing no staining in the tongue SCC (80x).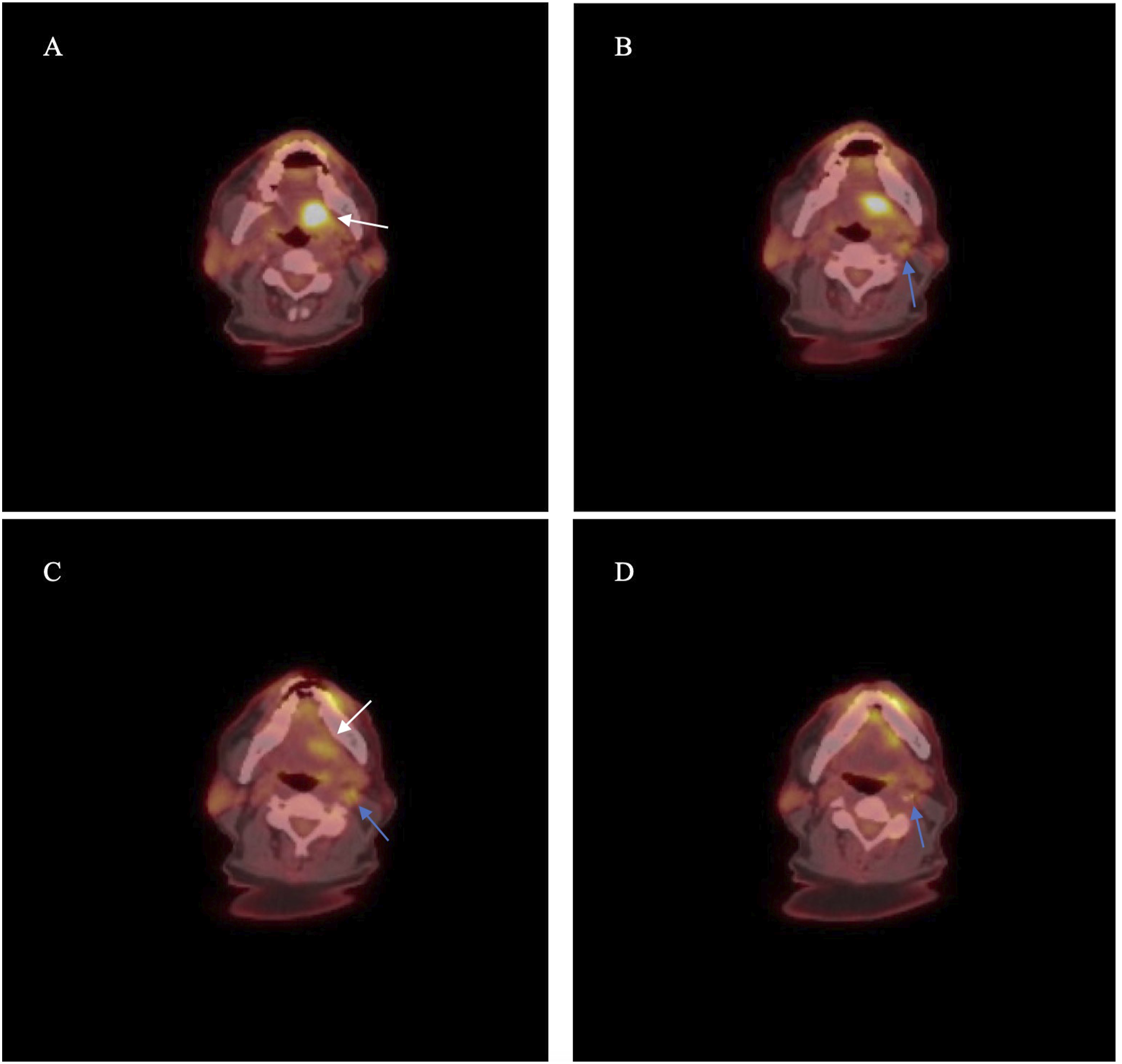
Discussion
SPMs are a significant obstacle to long-term survival in patients with HNSCC. We report a case of synchronous p16-negative and p16-positive SCC of the head and neck. Given the difference in the pathogenesis of HPV-mediated SCC, the co-occurrence of these subtypes is rare. While smoking-related HNSCC has been on the decline over the past 30 years, rates of squamous cell carcinoma of the oropharynx have been steadily increasing. The rise of oropharyngeal carcinoma has been mainly attributed to HPV. 5 The burden of oncogenic HPV strains has led to a sharp increase of HNSCC in younger age groups with no or little exposure to tobacco. 6 Given that HPV is sexually transmitted, early sexual debut and a higher number of sexual partners (including oral sex partners) are major risk factors for developing HPV-mediated HNSCC. 7 In contrast to HPV-unrelated HNSCC, HPV-mediated cases typically have a more favorable prognosis. Estimates suggest a 75–80% survival rate and better response to the chemo/radiotherapy. 8
Accumulating evidence suggests a decreased risk of SPMs in HPV-mediated HNSCC. It is hypothesized that lower rates of exposure to tobacco and lack of a field cancerization effect due to limited integration of HPV DNA into the tumor tissue are plausible explanations for this observation. 1,9 -11 Treatment of synchronous malignancies in the head and neck can be challenging due to potentially different treatment recommendations and morbidity of multisite disease. In this case, the same surgical field was able to address both tumors without additional surgery, and the same adjuvant treatment (radiation +/− chemotherapy) was indicated for both tumor types. In other cases, heterogeneity of stages and differences in sites of SPM complicate the treatment process, hence the lack of standardization of treatment among this patient population. Communication between specialists involved in multidisciplinary teams is crucial for treatment planning in patients with this complexity. While there is sparse literature on the management and treatment of these patients, timely detection and appropriate treatment approach are essential. Pre-operative exams and imaging did not separately identify a SPM in this case (likely due to tongue cancer overshadowing on imaging). Providers should be comprehensive and cautious in their workup to assess potential SPM in head and neck cancers.
Conclusion
Second primary malignancies present a potential risk for head and neck cancer patients. Although HPV-mediated SCC is associated with lower rates of SPM, as presented in this case, the emergence of synchronous malignancies with varied pathogenesis is still plausible. Patients presenting with high-risk factors for the development of both HPV-mediated and HPV-unrelated SCC should be considered for further evaluation for the possibility of synchronous tumors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (July 2023):
Article type has been updated.
Informed Consent
Informed consent was waived and not sought in our case study due to the lack of any identifying patient information.