
Abstract
Objectives
Thyroid surgeries are among the most common operations performed in the world. Hypocalcemia following total thyroidectomy (TT) is a common complication that is sometimes difficult to correct. This study aims to determine the frequency of hypocalcemia and permanent hypoparathyroidism (PtHPT) following TT.
Methods
A total of 363 patient records were reviewed who underwent TT for any reason. Thirty-eight patients did not have a follow-up in the clinic in the postoperative period and were excluded from the final analysis with the final sample as 325. For patients who developed hypocalcemia during the postoperative hospital stay, their lowest calcium levels were recorded and medical records were reviewed for the period of one year for the requirement of oral calcium and active form of vitamin D (calcitriol or alpha calcidiol) in the outpatient setting. Patients who required calcium and vitamin D supplementation for up to 1 year were labeled as having PtHPT. Risk factors were analyzed among those who developed PtHPT.
Results
From a total of 325 patients postoperative hypocalcemia developed in 163 (50.2%) patients, and 162 (49.8%) patients remained normocalcemic. Permanent hypoparathyroidism was found in 42(12.9%) patients and transient HPT in 121 (37.2%). Age, severe postoperative hypocalcemia (PoHC), and readmission for hypocalcemia were independent risk factors for PtHPT.
Conclusions
Transient hypoparathyroidism (THPT) is common in our setup. Patients who develop severe hypocalcemia postoperatively and need readmission should be closely followed for the development of PtHPT.
Introduction
Thyroid surgery is a common and safe operation performed for several benign and malignant conditions such as obstructive goiter, differentiated thyroid cancer, medullary thyroid cancer, and suspicious thyroid nodule. 1 Thyroid surgery has different complications like hemorrhage, recurrent laryngeal nerve injury resulting in change in voice or airway obstruction, hypoparathyroidism (HPT), infection, and hypothyroidism. 2 Among this, Postoperative hypocalcemia (PoHC) is the most common side-effect of total thyroidectomy (TT) with a possibility of 20-30%. 3 Postoperative hypocalcemia or HPT occurs due to dysfunction of the parathyroid gland 4 which occurs due to damage, removal, or de-vascularization of one or more parathyroid glands during surgery. The hungry bone syndrome may occasionally contribute to immediate PoHC.
The incidence of Transient Hypoparathyroidism (THPT) ranges from 19% to 47%, and Permanent Hypoparathyroidism (PtHPT) incidence range from 0% to 30%. 5 There are several risk factors associated with the development of hypocalcemia after thyroid cancer surgery. Bilateral neck lymph node dissection, gross extrathyroidal extension, and the presence of the parathyroid gland in the pathologic specimen (i.e., inadvertent removal of the parathyroid gland) are proven to be significant risk factors. 6 Acute hypocalcemia such as PoHC is generally symptomatic with typical manifestations like paresthesia, muscle spasms, Chvostek’s or Trousseau's signs, and in extreme cases seizures. This is because of resultant neuromuscular hyperexcitability. Chronic hypocalcemia may be asymptomatic. Postoperative hypocalcemia requires calcium and an active form of Vitamin D supplementation, with monitoring until blood calcium returns to normal, which in turn increases health care costs and prolongs hospitalization. While all patients with symptomatic hypocalcemia require oral calcium, and or intravenous calcium and vitamin D, whereas asymptomatic patients may or may not need calcium supplementation. Due to the vital role Vitamin D plays in maintaining calcium metabolism, , the fact that Pakistan reports the highest occurrence of Vitamin D deficiency in adults in South Asia is a cause for great concern. A staggering 73% of the population in Pakistan is affected, with only 15.3% having adequate Vitamin D levels, regardless of their age or gender.7,8 Transient hypocalcemia generally responds favorably to replacement therapy within a few days or weeks but it is considered permanent when it does not return to normal within 6 to 12 months. 9
Currently, studies are focusing on the search for reliable early predictors of PoHC. Intraoperative or early post-operative parathyroid hormone measurements to identify the sub-group of patients who are at risk of PoHC have been suggested. 10 Measuring intraoperative or standard intact PTH levels, and making a new algorithm by combining more than 2 of these values have all been reported as useful predictors. 11 However, these predictors also facilitate the thyroid surgeon, which patients can be discharged early and safely.
This study aims to determine the frequency of PtHPT in patients with hypocalcemia after TT at a tertiary care hospital and its associated risk factors.
Patients and Methods
A retrospective cohort study was conducted on patients who underwent total or completion thyroidectomy for any reasons identified through electronic health records from January 1, 2014 to December 31, 2018 at the Aga Khan University Hospital Karachi. Health charts were reviewed for physician’s notes, intraoperative notes for the identification of parathyroid gland, pathology reports for the presence of parathyroid gland in the surgical specimen(Parathyroid gland was identified on microscopic examination, it appeared as a nodule with clear cells at the margins or in the adjacent thyroid parenchyma), medication use during admission and on discharge, and subsequent outpatient follow-ups. Laboratory parameters were recorded along with cytology reports and histopathology from online electronic records. Follow-up up to 1-year post-surgery was also recorded. Patients of either sex or age were included and those with known chronic kidney disease or parathyroid abnormality at the time of admission were excluded from the study. Post-operative lowest calcium level during admission was recorded.
Hypocalcemia is defined as serum total calcium <8.5mg/dl or ionized calcium <4.6mg/dl. Mild hypocalcemia is defined as serum total calcium between 7.5-8.4 mg/dl or ionized calcium > 3 mg/dl. Severe hypocalcemia is defined as serum total calcium < 7.5 mg/dl or ionized calcium < 3 mg/dl. Patient demographics and clinical, surgical, and histo-pathological characteristics were recorded. At each follow-up, the need for calcium and an active form of vitamin D replacement was also recorded for up to one year. Transient hypoparathyroidism was defined as hypocalcemia that persists for less than 1 year and PtHPT was defined as hypocalcemia lasting for one or more than 1 year. 12
As per the eligibility criteria, 363 patient charts were reviewed, out of which a total of 38 patients were excluded (37 patients were lost to follow-up and 1 patient underwent simultaneous parathyroidectomy) from the final analysis.
Data were analyzed using STATA version 14.0. Continuous data were reported as mean ± standard deviation and categorical data are presented as frequency along with percentages. Kruskal Wallis test was used for assessing the difference of means between normocalcaemia, transient hypocalcemia, and permanent hypocalcemia. Chi-squared test or student t-test was applied for the association between PtHPT patients and without PtHPT patients as appropriate. Applied logistic regression was applied for the risk factors of PtHPT. Odds ratio along with 95% CI were reported and P-value <0.05 was taken as significant. Ethics review committee approval was taken prior to the conduct of this study.
Results
Patient Characteristics.
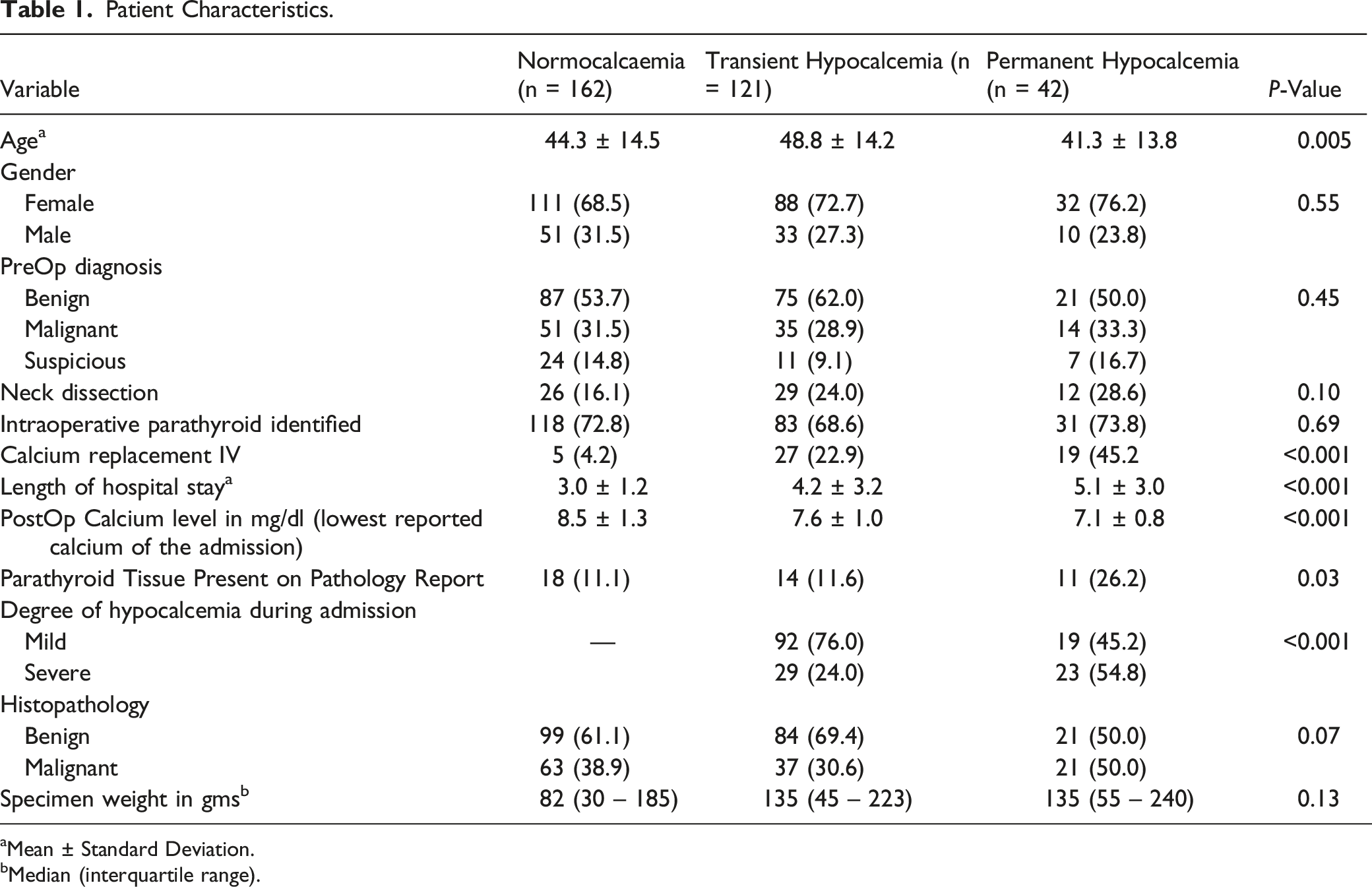
aMean ± Standard Deviation.
bMedian (interquartile range).
Variables Associated with and without Permanent Hypoparathyroidism.
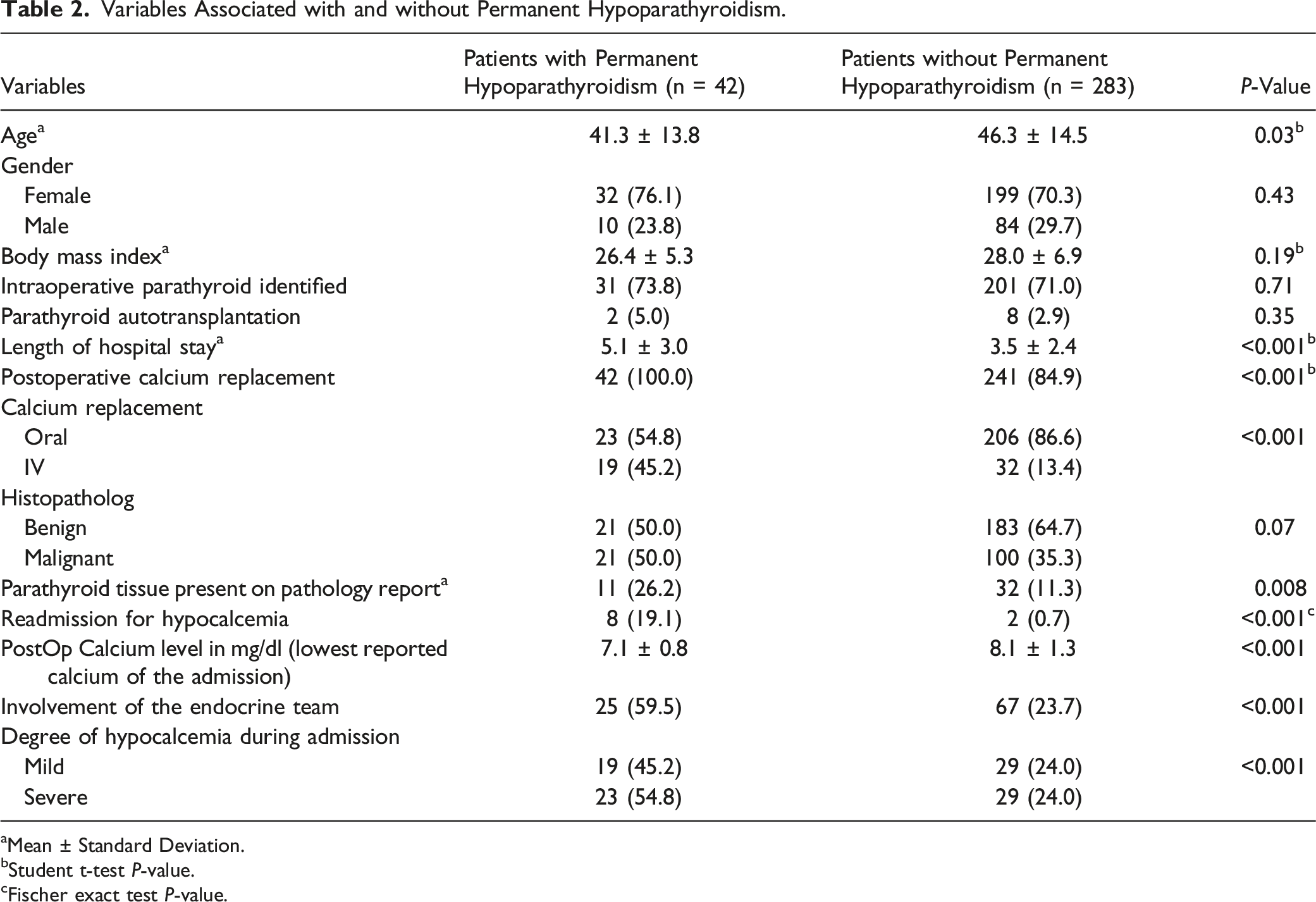
aMean ± Standard Deviation.
bStudent t-test P-value.
cFischer exact test P-value.
Univariate and Multivariate Analysis of Variables Associated with Permanent Hypoparathyroidism.

Discussion
Hypocalcemia after TT is a common complication. In our study, around 50% of patients developed hypocalcemia after TT which is comparable to other prospective and cross-sectional studies.13-15 A study in China reported hypocalcemia to be present in 27% of the patients and HPT in 15% of the patients. 16 Another study in India reported hypocalcemia to be present in 52% of the patients after thyroidectomy. 17 However, there is a dearth of research on this subject in Pakistan.
Parathyroid tissue was identified in a quarter of patients with PtHPT, devascularization of the gland may be a significant reason in remaining patients. Techniques have been developed for better identification of the blood supply of the parathyroid gland. According to an RCT intraoperative identification of parathyroid gland by angiography with indocyanine green (ICG) obviates the need for supplementation with calcium and vitamin D as it reliably predicts the blood supply of the parathyroid gland. 18
Postoperative serum calcium, intravenous calcium replacement, and readmission for hypocalcemia which shows the severity of hypocalcemia were associated with PtHPT. These patients should be followed more closely for the development of PtHPT. This has been previously shown in pediatric population where degree of PoHC was related to permanent hypothyroidism. 19
According to a meta-analysis, younger patients were more likely to develop hypocalcemia, 20 finding similar to our study. It is a significant morbidity that would remain with them lifelong. Young age with PtHPT results in more years taking calcium and vitamin D, a similar result found in patients with severe hypocalcemia after surgery in Graves disease. 21 In a retrospective study from Italy young patients undergoing neck dissection and with incidental parathyroidectomy have the highest risk of postoperative HPT after surgery for thyroid cancer. 13
In our study half of the patients who developed PtHPT had benign pathology though in a prospective cohort, surgery for cancer was the risk factor for PtHPT. 22 This is a concerning feature as POHC increases the duration of hospital stay which leads to increased healthcare costs, utilization of resources, and patient discomfort. In our study, patients who developed transient or PtHPT have longer length of stay. Fanget F et al reported in a systemic review that postoperative HPT is associated with increased costs due to additional therapy and additional hospital costs. 23
There are several limitations to our study that need to be taken into account. Firstly, the study was conducted at a single center, which may limit the generalizability of our findings to other settings, despite the hospital catering to a larger population from various parts of the country. Moreover, we did not analyze data on individual surgeon's experience, including years since training and volume of cases, which may have impacted our results. However, the surgery was performed by the same surgical team with high case volumes and good surgical experience. Another significant limitation is the absence of consideration for blood albumin levels when calculating calcium values. This is because albumin levels were not measured in the immediate postoperative period. However, it was measured for patients during their follow-up visits, and the results showed that their albumin levels were normal. Furthermore, we did not measure the thyroid volume in all patients on ultrasound, but instead recorded and analyzed the weight of the excised tissue to determine the median weight in grams of the thyroid tissue in 3 patient characteristic categories: normocalcemia, transient hypocalcemia, and permanent hypocalcemia. Lastly, our study is retrospective, which limits our ability to establish cause-and-effect relationships between HPT and TT. These limitations highlight the need for further research in this area to develop a more comprehensive understanding of the topic.
However, our study also has a major strength in its large sample size, which is a significant advantage. We included all consecutive patients, reducing the risk of selection bias.
Conclusion
In conclusion, post TT HPT is common. Younger patients who developed severe PoHC and those got readmitted for it should be followed more closely for the development of PtHPT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Contributions
AN has designed the concept, data collection data analysis and manuscript writing. SS has done data analysis and manuscript writing. FK, MW, and AH has collected the data. MS, MI, and MQM were involved in manuscript writing and proof reading of the article and submission.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.