
Abstract

Introduction
Thyroid fine needle aspiration (FNA) biopsy is the cornerstone in the evaluation of thyroid nodular disease. Surgeon performance of both ultrasound and biopsy is rapidly becoming part of Head and Neck Surgery clinical practice. Surgeon-performed ultrasound and biopsy benefits the patient by consolidating care and allowing surgeons to become familiar with patient anatomy. This also allows for better preoperative planning and patient disclosure.
Despite the routine use of imaging guidance, between 3 and 35% of FNAs are non-diagnostic.1-6 These insufficient samples prompt repeat office visits, additional procedures, and delays in care. Ideally, the rate of non-diagnostic thyroid FNAs is less than 10%.
We hypothesized that immediate on-site review of FNA samples by a clinician could potentially reduce non-diagnostic sampling and prevent treatment delay. Our goal was to determine if FNA samples that are immediately reviewed on-site for adequacy are associated with a lower rate of non-diagnostic results.
Patients and Methods
We performed a retrospective chart review of all thyroid FNAs over a 30-month period (July 1, 2014 to December 31, 2016) at our tertiary care center in Seattle, Washington. Ultrasound-guided FNAs obtained by a single otolaryngologist which underwent immediate on-site review by the same surgeon for adequacy were compared to all ultrasound-guided FNAs generated by clinicians without on-site review. The surgeon received education from a board-certified cytopathologist on features constituting sample adequacy. A pathology laboratory assistant was employed to process slides with a rapid Papanicolaou stain for on-site review for adequacy. After samples were deemed adequate by the performing surgeon, samples were subsequently reviewed by a pathologist with stratification by Bethesda category. Samples in the comparison group were obtained by radiologists, endocrinologists, and otolaryngologists. Samples which had undergone immediate on-site review for adequacy were compared to those without immediate review using a standard chi-squared statistical tests with significance for P < .05. There were no exclusion criteria.
Results
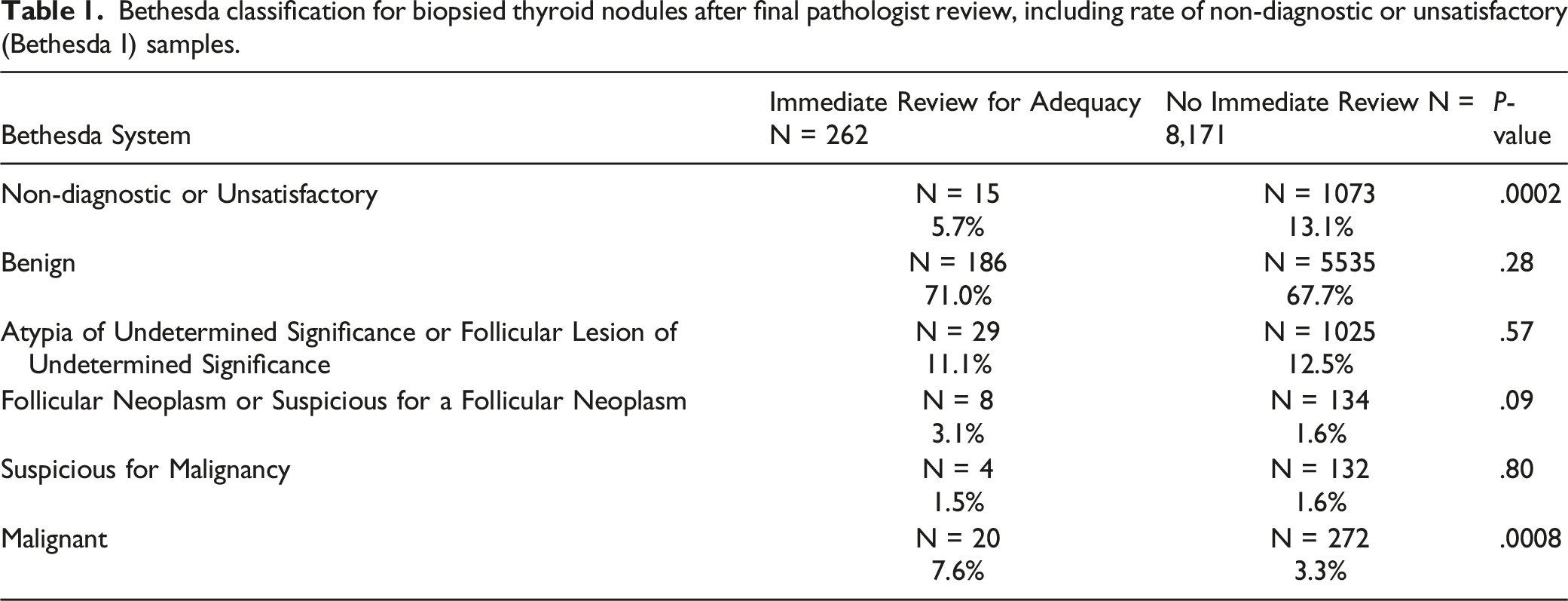
Bethesda classification for biopsied thyroid nodules after final pathologist review, including rate of non-diagnostic or unsatisfactory (Bethesda I) samples.
Discussion
Immediate review of thyroid FNA samples has previously been shown to improve diagnostic yield.1,3,4 FNAs that undergo on-site review correlate with a reduction in diagnostic ambiguity.
Our study showed a statistically significant reduction in non-diagnostic samples with on-site review. This clinician-inspired improvement decreases time to treatment and reduces cost associated with a second biopsy and an additional formal pathology review. There is no need for a pathologist to be present at the initial immediate clinical review if clinicians have been trained to recognize adequacy criteria for FNA. In our study, there was also a significantly higher rate of malignant diagnoses. Though our primary goal was ensuring adequate cellularity on FNA sample, surgeons that are familiar with thyroid carcinoma and its associated cytopathology can recognize cancer based on early slide review, encouraging prompt communication between surgeons and pathologists over concerning findings.
Surgeons are incorporating ultrasound-guided FNA into their practices. There is not a large learning curve; it has been shown that surgeons can achieve 85% adequacy in 300 cases. 2 Surgeons can work to incorporate on-site review for adequacy into their clinical practice. Improved understanding of FNA cytopathology as well as the decreased delay in treatment associated with improved adequacy need not be limited to surgical practices. We encourage other clinicians to adopt on-site review of FNA samples, either by themselves or a cytopathologist, as their patients will likely derive similar benefit.
A possible confounder in this study is referral, however, in our hospital system, patients are referred at random to the first available practitioner. There is no bias for referral based on the size of nodules or nature of disease. The heterogeneity in clinicians obtaining samples in the comparison group is another confounder. Our results were not stratified by specialty of clinician, nodule size, or characteristics, which could be an area of further investigation.
Conclusion
On-site review for adequacy of clinician-performed thyroid FNA reduces non-diagnostic samples. With the increase in popularity of surgeon-performed FNAs in clinic, training surgeons to recognize features of cellular adequacy may further streamline the diagnostic process and aid in timely management of malignant disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.