
Abstract
Although nasopharyngeal angiofibroma is an expected tumor in adolescent males, it is uncommon in the elderly. Because of its high vascularity or bleeding during biopsy, surgical resection can be life threatening. Therefore, nasal angiofibroma should be kept in mind in existing masses especially in elderly patients and support should be obtained from imaging methods.
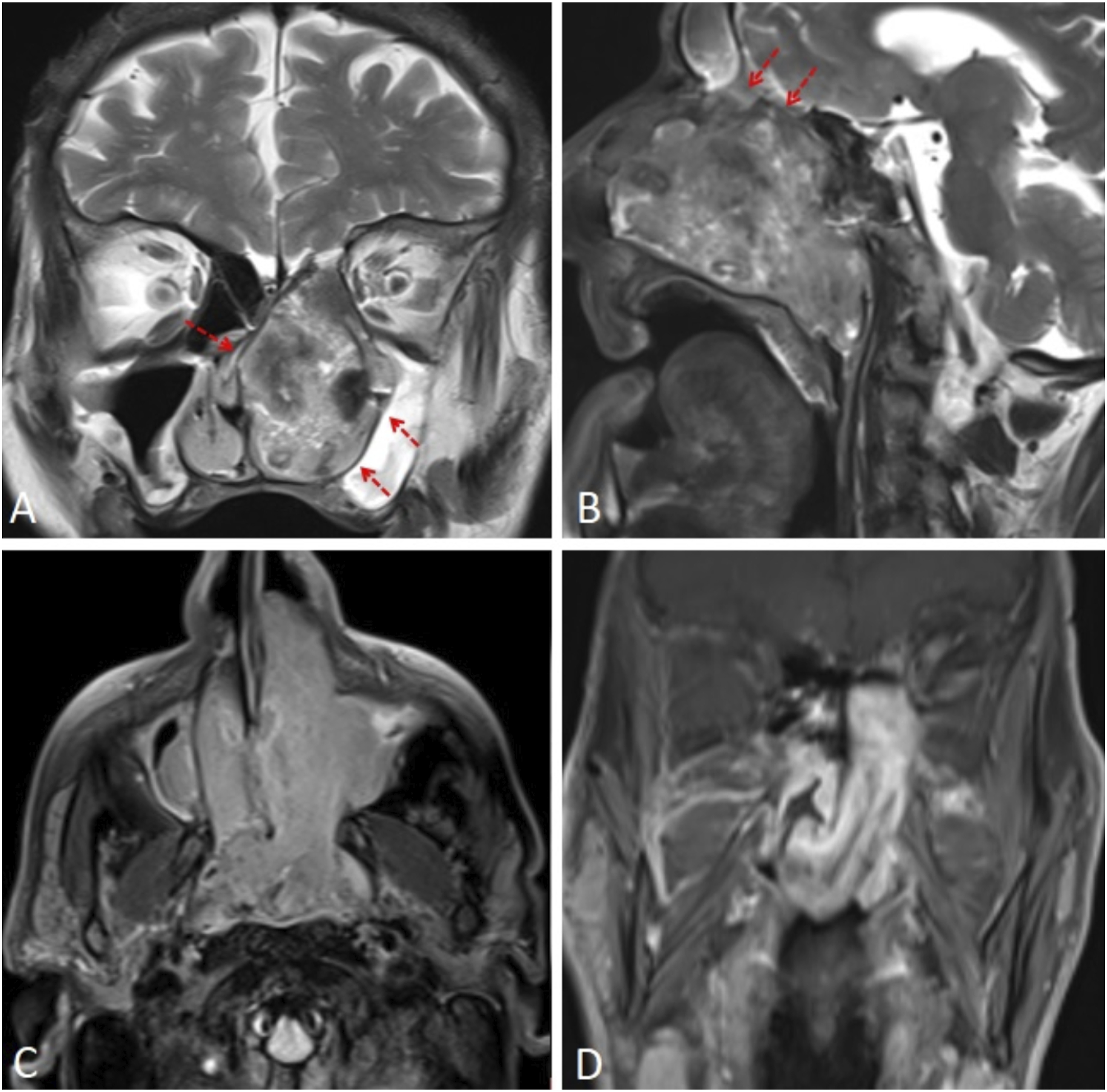
A 77-year-old man presented to our otorhinolaryngology clinic with left-sided nasal obstruction, difficulty in breathing, and intermittent epistaxis. He had no known chronic disease other than diabetes mellitus and no history of trauma or surgery. Examination revealed a mass lesion filling the left nasal cavity and extending into the nasopharynx. Contrast-enhanced head and neck computed tomography (CT) was performed with a possible diagnosis of squamous cell carcinoma. The images obtained showed a heterogeneous mass lesion approximately 7 × 6 × 4 cm in size, filling the left nasal cavity and nasopharynx. The lesion was heterogeneously contrast enhancing and destroyed the medial wall of the left maxillary sinus and nasal septum (Figure 1). Contrast-enhanced magnetic resonance imaging (MRI) was performed to show soft tissue extension. The mass lesion was hypointense on T1-weighted images, heterogeneously hyperintense on T2-weighted images, and contained signal void areas. The lesion originated from the left lateral wall of the nasopharynx and almost completely obliterated the nasopharynx and left nasal cavity. The ethmoid cells appeared invaded superiorly. Intense contrast enhancement of the mass was observed in contrast-enhanced series (Figure 2). Histopathologic examination of the biopsy specimen taken from the nasal cavity revealed the diagnosis of angiofibroma. The patient did not accept the operation and radiotherapy was applied. Axial (A) and sagittal (B) contrast-enhanced CT images show a heterogeneous contrast enhancing mass (asterix) filling the nasopharynx and left nasal cavity, destroying the maxillary sinus wall and nasal septum (arrows). T2-weighted images of coronal (A) and sagittal (B) sections show a heterogeneous hyperintense mass. The lesion pressure remodels the maxillary sinus and nasal septum and extends to the ethmoid cells (arrows). Postcontrast axial (C) and coronal (D) sections show significant contrast enhancement.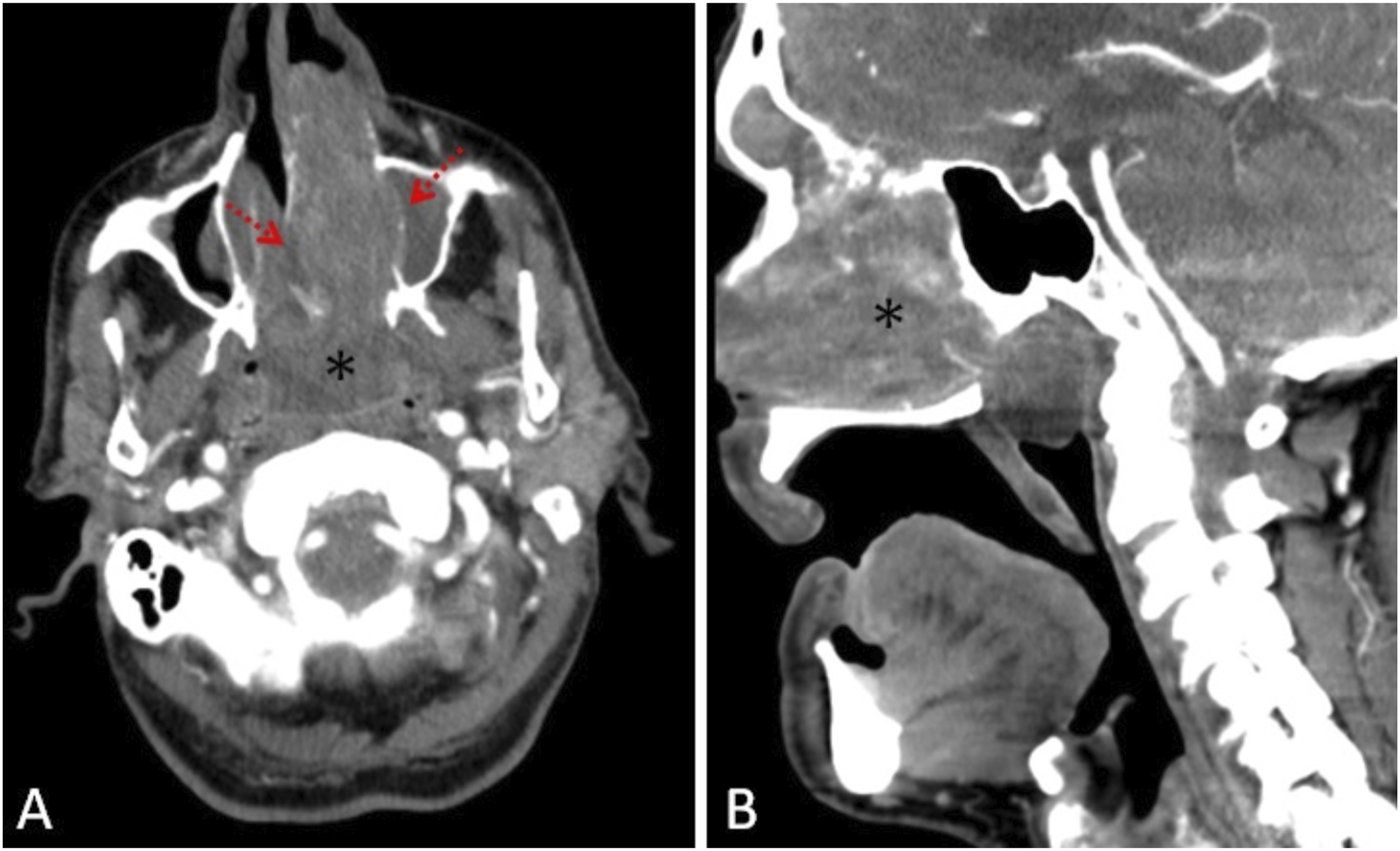
Nasopharyngeal angiofibroma accounts for less than 1% of head and neck neoplasms. It is mostly seen in the age range of 10–25 years and in males and is very rare in the elderly. They are benign but locally aggressive vascular tumors originating from the sphenopalatine fossa.1,2 Although the etiology is not known exactly, it is theorized to be a true neoplasm as well as a vascular malformation due to the remnant of the first branchial artery. 3 The main symptoms are unilateral or bilateral nasal obstruction and epistaxis. Depending on the extent of the lesion, progressive swelling, hyposmia, headache, visual disturbances, proptosis, and neurological deficits may occur. Anamnesis, clinical symptoms and physical examination are important in the diagnosis. Characteristic findings on CT and MR imaging also support the diagnosis, show the extent of the lesion, and are used in follow-up. Definitive diagnosis is made histopathologically, even if it is risky in terms of bleeding.2,3 The lesion has a soft tissue density with lobulated contour on CT images and destructive changes in the bones can be easily observed. Angiography can be used to identify the feeding artery in patients who can undergo embolization. On MR images, signal void areas within the lesion with heterogeneous intensity on T2-weighted images (salt and pepper appearance) are typical. The lesions are markedly contrast enhanced on postcontrast imaging due to their high vascularity. Surgical resection with or without preoperative embolization is the first treatment option. Radiotherapy can be applied in patients who cannot undergo surgery or who have recurrence.3-5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.