
Abstract
Background
Studies on neck management of early-stage floor of mouth (FOM) squamous cell carcinoma (SCC) are very few and controversial. We aimed to study whether elective neck dissection (END) for patients with clinically stage T1N0M0 (cT1N0M0) FOM SCC is beneficial for survival.
Methods
Information on patients diagnosed with cT1N0M0 FOM SCC between 2004 and 2015 was collected from the Surveillance, Epidemiology and End Results (SEER) database. Cox proportional risk models and Kaplan–Meier curves were used for survival analysis and log-rank tests were performed to compare whether overall survival (OS) and cancer-specific survival (CSS) differed. Propensity score matching (PSM) was performed to eliminate the effect of confounding variables.
Results
There were 1014 patients with cT1N0M0 FOM SCC. Among them, END group: 455 cases; observation group: 559 cases. COX regression analysis before PSM demonstrated hazard ratio (HR) in the observation group compared to END (OS: 1.108 (.926–1.326), P = .262; CSS: 1.033 (.772–1.382), P = .827). There was no survival difference between END and observation survival before PSM (5-year OS: 71.8% vs. 67.8%, P = .180; 5-year CSS: 84.5% vs. 84.8%, P = .930); the matched results were the same as before PSM.
Conclusion
Observation may be a more appropriate option compared with END in cT1N0M0 FOM SCC.
Introduction
Oral cancer is the seventh most common cancer worldwide. 1 Recent global estimates have indicated that there will be 377713 new cases and 177757 deaths from oral cancer in 2022.2,3 Among them, squamous cell carcinoma (SCC) comprises more than 90% of all oral malignancies.4,5 As one of the common sites for oral cancer, the floor of mouth (FOM) accounts for about 27.2% of it. 6 Although treatment modalities are improving, the prognosis for FOM SCC remains poor, with 5-year overall survival (OS) rate of 39% and cancer-specific survival (CSS) rate of 59%. 7 This is mainly due to the abundant lymphatic drainage in the oral cavity and the early onset and duration of local lymph node metastases in oral SCC. 8 It has been reported in several publications that lymph node metastases can reduce patient survival by 50% compared to lymph node negativity.9,10,11
Management of the neck in patients with negative clinical lymph nodes has been controversial, considering the presence of occult neck metastases that are clinically and imaging undetectable. Among others, proponents of elective neck dissection (END) have argued that the procedure reduces recurrence rates and improves survival in patients. 12 However, pro-observation scholars have evidenced that in cT1-2N0 patients, the OS and disease-free survival of patients were not statistically different between END and observation. 13 Hongshi Cai et al. have reported that there was no statistical difference in cervical lymph node recurrence in FOM between the END and observation groups. However, considering the small number of patients with cT1-T2N0 FOM SCC, it remains to be determined whether END treatment is superior to the observation group. 13
The tongue and FOM are common sites from which early nodal metastasis develop in the oral cavity, and many research have demonstrated that END in early-stage tongue cancer is associated with reduced regional recurrence and prolonging OS.14–16 However, the incidence of FOM SCC is small, and most studies were single-center, therefore the debate on whether END for early-stage FOM SCC is beneficial for survival is still inconclusive. Surveillance, Epidemiology and End Results (SEER) is a publicly available oncology database that collects information from nearly 30% of the US population. Here the purpose of our study was to use the data from SEER to quantify the value of END for clinically staged T1N0M0 (cT1N0M0) FOM SCC.
Materials and Methods
Data Acquisition
Data of patients with FOM SCC which diagnosed as 6th American Joint Committee on Cancer (AJCC) N0 stage were obtained from the SEER database through the SEER*Stat software (version 8.4.0; www.seer.cancer.gov). Inclusion criteria were displayed in Figure 1: (1) International Classification of Disease for Oncology third edition (ICD-O3) site codes (“C04.0-Anterior floor of mouth,” “C04.1-Lateral floor of mouth,” “C04.8-Overlapping lesion of floor of mouth,” “C04.9-Floor of mouth, NOS”). Morphology codes were: 8070/3-8076/3; (2) SCC was confirmed by pathology; (3) FOM SCC was the only cancer or the first primary tumor diagnosed; (4) year of diagnosis was from 2004 to 2015. Exclusion criteria were (1) non-T1N0M0 patients; (2) OS less than one month; (3) unknown race and cause of death information; (4) lymph node surgery as a biopsy, unknown; (5) radiotherapy information as a radioactive transplant; (6) the code of tumor size was unknown. As the SEER database is a public database, institutional review of patient informed consent is not required. OS was defined as the interval between the date of surgery and the date of death from any cause or the date of the last follow-up visit. CSS was measured as the interval from the date of surgery to the date of death due to the FOM SCC. The flowchart of this study. Abbreviations: SEER, Surveillance, Epidemiology and End Results.
Statistical Analysis
The Cox proportional risk model was used to determine prognostic factors for survival in cT1N0M0 FOM SCC, and survival curves were graphed by the Kaplan–Meier method, with log-rank tests comparing END group with observation group patients for differences in OS and CSS. In additional, to minimize the effect of confounding factors, we performed propensity score matching (PSM) with a 1:1 ratio of END to observation patients, and then used a logistic regression model to calculate the propensity score for each patient. The model included the following variables: age, sex, race, year of diagnosis, tumor grade, tumor size, marital status, and radiotherapy and chemotherapy. Matching was performed using a non-replacement caliper matching method. The caliper value was set at .01. The standardized mean difference (SMD) was used to evaluate whether variables were balanced between the observation and END groups before and after matching, with SMD value <.10 as the criterion for adequate balance.17,18 All statistical analyses were performed using R statistical software (version 4.0.3). The test was P < .05.
Results
Baseline Characteristics
Clinical Characteristics of cT1N0M0 FOM SCC Patients before and after Matching.

Note: Others = American Indian/Alaska Native or Asian or Pacific Islander.
Abbreviations: END, elective neck dissection; PSM, propensity score matching; SMD, standardized mean difference.
COX Regression Analysis
COX Regression Analysis of OS and CSS in Patients with cT1N0M0 FOM SCC before Matching.
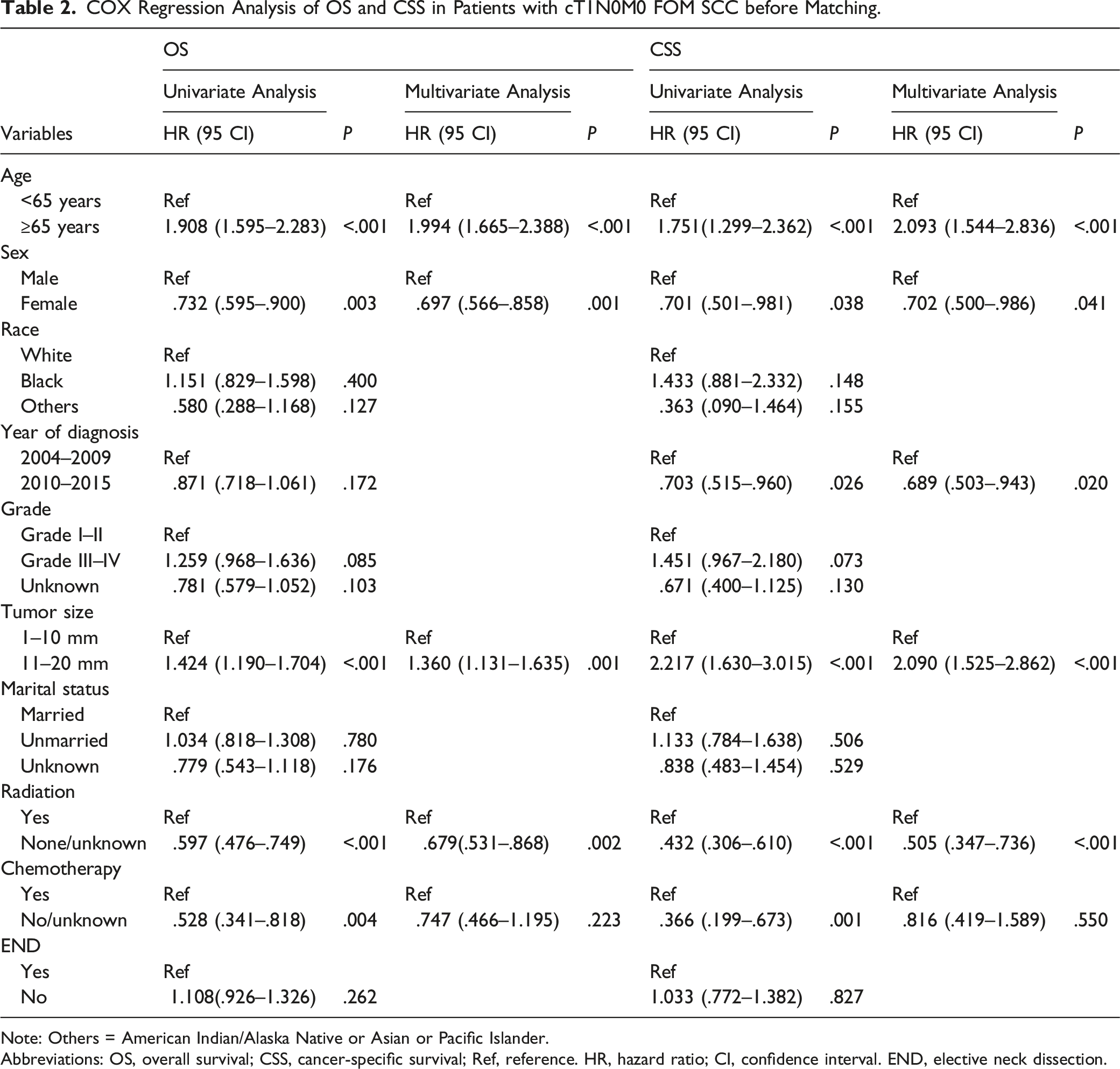
Note: Others = American Indian/Alaska Native or Asian or Pacific Islander.
Abbreviations: OS, overall survival; CSS, cancer-specific survival; Ref, reference. HR, hazard ratio; CI, confidence interval. END, elective neck dissection.
COX Regression Analysis of OS and CSS in Patients with cT1N0M0 FOM SCC after Matching.

Note: Others = American Indian/Alaska Native or Asian or Pacific Islander.
Abbreviations: OS, overall survival; CSS, cancer-specific survival; Ref, reference; HR, hazard ratio; CI, confidence interval; END, elective neck dissection.
Comparison of Survival Between END and Observation Groups
Kaplan–Meier survival curves for OS and CSS before PSM were exhibited in Figure 2A-B, where it can be observed that there was no statistical difference in survival in the END compared to the observation group (5-year OS: 71.8% vs. 67.8%, P = .180; 5-year CSS: 84.5% vs. 84.8%, P = .930). Moreover, there was still no significant difference in survival in the END group compared with the observation group after PSM (Figure 2C-D). To further assess whether survival differed between the END group and the observation group on various clinical characteristics, we performed subgroup survival analysis on the matched cohort. As presented in Figure 3A-B, the hazard ratio (HR) values for the observation group were close to 1 compared to the END on each subgroup and were not statistically different (P > .05). Survival curves for patients with cT1N0M0 FOM SCC receiving END versus observation group. A: OS before PSM; B: CSS before PSM; C: OS after PSM; D: CSS after PSM. Abbreviations: FOM, floor of mouth; SCC, squamous cell carcinoma; END, elective neck dissection; OS, overall survival; CSS, cancer-specific survival; PSM, propensity score matching. Forest plots for subgroup analysis of OS (A) and CSS (B) after matching C: Plot of differences between variables before and after matching, (SMD) less than .1 is the criterion for balance. Abbreviations: OS, overall survival; CSS, cancer-specific survival; SMD, standardized mean difference. Note: Others = American Indian/Alaska Native or Asian or Pacific Islander.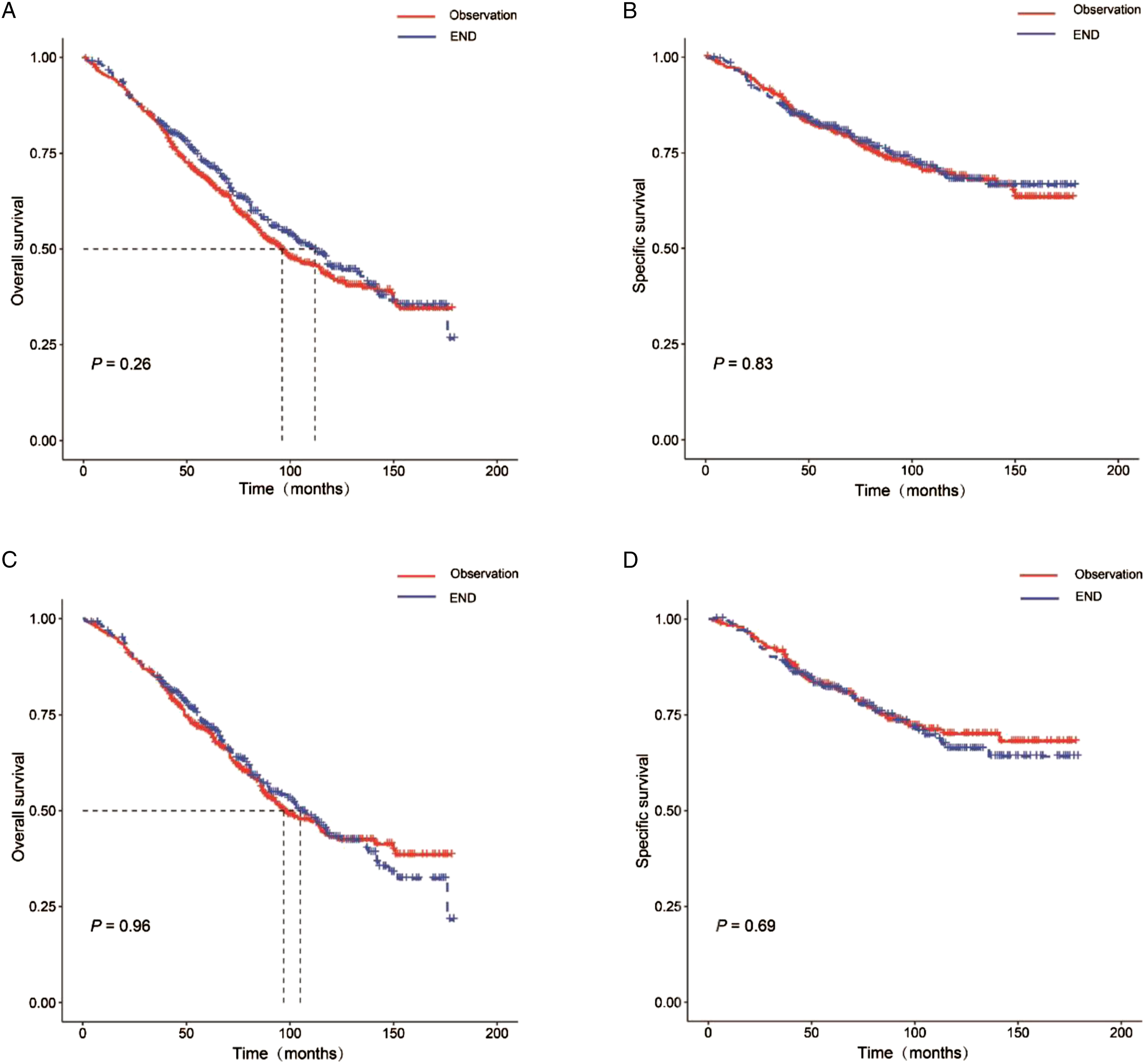

Discussion
The FOM, as one of the common sites of oral cancer, has been studied by most scholars in combination with malignancies in other subsites of oral due to the risk factors for recurrence and survival that are similar to those of the oral cancer population. 19 It has been suggested that when the risk of occult metastases exceeds 15-20%, END can be performed to avoid the spread of occult metastases.20,21 However, most studies on lymph node dissection grouped T1 and T2 together. This could lead to bias and error in the analysis of patients with T1 staging due to the differences in clinical presentation between the two. For instance, Conner Massey et al had noted that in oral cancer patients the rate of occult lymph node metastasis in T1 patients was 11.5%, while the rate of occult metastasis in patients with T2 tumor was more than twice that of T1 (24.5%), so they recommended the use of END in the T2N0M0 group, which was observed in the T1N0M0 OSCC group. 8 Similar results have also been made with FOM SCC, where Paolo Cariati et al. discovered occult lymph node metastases in 12.9% and 30.7% of patients with T1 and T2 stage, respectively. 22 This suggests that the value of END should be evaluated separately for the T1 and T2 groups.
We collected data on 1014 patients with cT1N0M0 FOM SCC through the SEER database to assess the value of END. The results showed that END was not a prognostic factor for it. Moreover, there was no significant difference in OS and CSS in the observation group compared to the END group (P > .05). Considering the possible bias from confounding factors, we implemented PSM for the END group and observation. After matching, with 346 patients in each of the END and Observation groups, we found that there was still no difference in OS and CSS between the two groups, which was essentially the same as before matching (P > .05). This indicated that the END group had no survival advantage in terms of OS and CSS compared with the observation groups. Given that there is insufficient data to support the need for lymph node dissection in early-stage FOM SCC, many academics have focused on the utility of sentinel lymph node biopsy (SNB). SNB is a new diagnostic tool that detects microscopic tumor deposits in the lymph nodes of the neck. The advantage of this approach is that treatment is tailored to the individual patient and only those patients with positive anterior lymph nodes can undergo therapeutic neck dissection. Alvarez J et al found that biopsy was not harmful to the survival of patients with floor of mouth cancer and prevented 65% of patients from undertaking END. 23 However, it has a 14% false negative, 23 so further research is needed on its application in FOM cancer. Furthermore, our study demonstrated that age, tumor size and radiotherapy were independent prognostic factors for T1N0M0 mouth floor cancer before and after matching. It has been widely established that age and tumor size are risk factors for survival in cancer patients. 24 However, it was surprising that our analysis found a lower risk of death in patients without radiotherapy compared to radiotherapy in cT1N0M0 FOM SCC. Satvir Saggi et al. have also reported negative effects of radiotherapy on CSS in the early-stage FOM cancer. 19 These findings may be related to inadequate treatment or severe complications. 25
In conclusion, observation may be a more appropriate option for patients with cT1N0M0 FOM SCC. Despite these findings, there are limitations to our study. First, in the 8th edition of AJCC staging, 26 T1 has been updated as tumor size of ≤ 2 cm and depth of infiltration (DOI) ≤ 5 mm. It has been found that DOI is also closely related to survival, with a 5-year OS rate of 93.3% for patients with tumor thickness < 4 mm. In contrast, the OS rate was only 33.3% in cases with DOI >4 mm. 22 And the National Comprehensive Cancer Network (NCCN) guidelines strongly recommend END for patients with tumor thickness greater than 4 mm. 27 However, this information was not provided in SEER database. In addition, possible coding errors of the SEER database and the absence of specific information on the extent of lymph node dissection, side effects and complications of surgery, chemotherapy and radiotherapy had limited our interpretation of the results. Finally, PSM eliminated the effect of confounding factors, but itself may introduce potential selection bias and the level of evidence remains lower than in randomized controlled clinical trials. 28 With these limitations in mind, multicenter, prospective, randomized controlled trials are required to minimize confusion and confirm these findings.
Conclusion
In conclusion, in this study population of cT1N0M0 FOM SCC, there was no significant difference in OS and CSS in the observation group compared with END. Observation may be an appropriate option but further study is warranted.
Footnotes
Acknowledgements
Thanks to the creators of the SEER database and all the staff for providing us with a public database.
Author Contributions
TL conceived the project, designed the research and drafted the manuscript. CC, YW directed this research. CJ, YW, and XX revised the manuscript. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Central University Basic Research Fund of China (No. WK9110000146).
Ethical Approval
As the SEER database is a public database, ethics and patient consent are not applicable in our study.
Informed Consent
There is no need for institutional review of patient informed consent for the SEER database is a public database.