
Abstract
Actinomycosis infection in the nasal cavity, especially an actinomyces rhinolith, is extremely rare. It should be considered in cases where a heterogenous calcified mass is found within the nasal cavity on endoscopy and radiographically. Treatment includes surgical debridement and a prolonged course of antibiotics, unique from the more typically encountered fungus ball. This case highlights the broad differential for chronic cough and throat pain and the importance of considering sinonasal contributions to throat symptoms.
Main Text
A 54-year-old male with a history of gastroesophageal reflux disease on acid suppression presented with throat pain and chronic cough since open heart surgery over one year prior. He denied sinus infections, nasal obstruction, or nasal discharge. On flexible laryngoscopy, a hard mass was found originating from his right ostiomeatal complex that looked fungal and heterogeneous in appearance. A computed tomography (CT) scan of the sinuses without contrast demonstrated asymmetric opacification and slight expansion of the right inferior nasal cavity with internal high-density debris appearing partially calcified (Figure 1). He then underwent endoscopic biopsy and debridement in the operating room. Computed tomography of the sinuses without contrast. Expansion of the right nasal cavity with internal high-density debris appearing partially calcified/mineralized (arrow) in the following planes (A) coronal, (B) axial, and (C) sagittal. Localizer lines present in panel B and C.
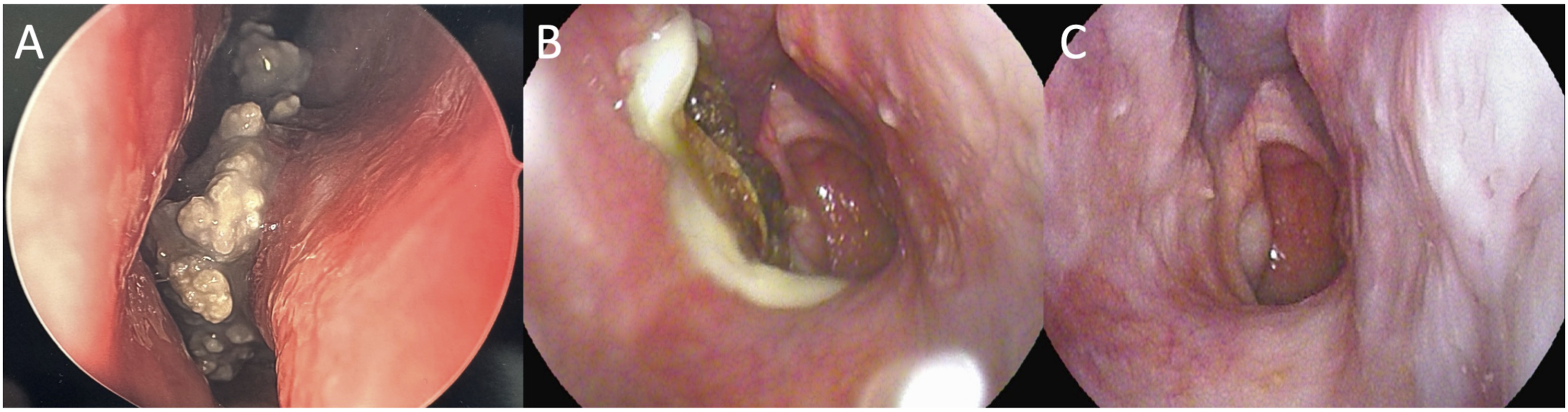
Intraoperative findings demonstrated a right-sided hard sinonasal mass with inflammation of the surrounding mucosa. Biopsy revealed free mucin with many clusters of filamentous organisms consistent with an actinomyces rhinolith on Gomori Methanamine Silver (GMS) stain (Figure 2). Surrounding mucosa revealed benign respiratory mucosa with marked lymphoplasmacytic infiltrate. The patient was started on amoxicillin 500 milligrams twice daily for actinomyces rhinolith as well as nasal saline irrigation. His cough and throat pain resolved after finishing a 4-month course of antibiotics. Endoscopic resolution is shown in Figure 3. Histology of nasal cavity mass with Gomori Methanamine Silver (GMS) stain. Free mucin with many clusters of filamentous organisms consistent with actinomyces are seen in each panel with the following magnification (A) 25.2x, (B) 25.2x, (C) 12.6x. Endoscopic images of nasal cavity actinomyces rhinolith. (A). Intraoperative photos within right nasal cavity (septum on right, inferior turbinate on left), (B) 7 weeks post-surgery, (C) 5 months post-surgery and at conclusion of antibiotic course.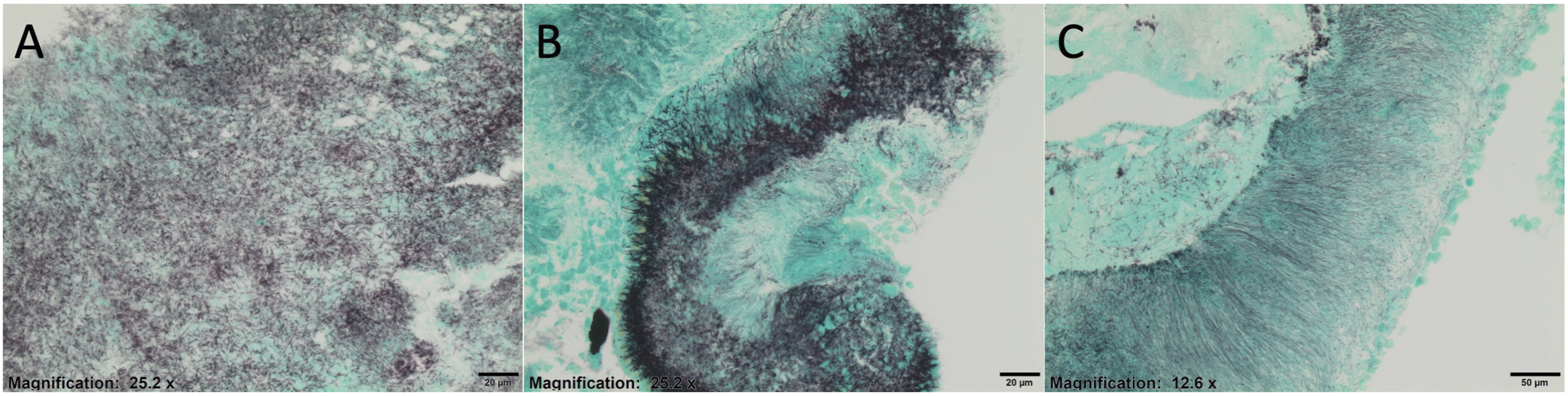
Rhinolith is a relatively rare condition caused by the mineralization of an endogenous or exogenous nidus in the nasal cavity. They are most found during anterior rhinoscopy and slowly can grow large enough to cause irritation of the nasal mucosa, discharge, and breathing problems. A recent case series of 23 patients with rhinoliths found that the most frequently reported symptoms were nasal obstruction (100%), purulent rhinorrhea (82.6%), nasal malodor (78.2%), oral malodor (26%), headache (26%), epistaxis (17.3%), and facial pain (4.4%). 1 In a similar series of 31 patients, rhinolith were most located between the inferior turbinate and septum. 2 Average age was 25 ± 12–15 years old with a similar distribution among men and women.1,2
Actinomycosis is a gram positive, filamentous, anaerobic bacterium. Actinomyces israelii is the most common pathogen and is part of the normal flora of the oral cavity, gastrointestinal, and urogenital tracts.3,4 For this bacterium to become pathogenic, two conditions must be fulfilled. First, a mucosal disruption must occur to allow the bacteria to invade into submucosal tissue. Second, after inoculation, Actinomyces spp. require synergistic bacteria to create an anaerobic environment to allow for growth and spread of infection. 5 Due to its dependence on synergistic bacteria, actinomyces infections are often polymicrobial. 6 Actinomycosis is characterized by chronic granulomatous inflammation with formation of small, sulfur-like granules due to their yellow, chalky appearance.
The literature has described actinomycosis affecting various anatomical structures (eg. face, bone and joint, respiratory tract, genitourinary tract, digestive tract, central nervous system, skin, and soft tissue structures). 6 Cervicofacial actinomycosis following odontogenic source of infection, is the most common clinical presentation, representing approximately 60% of reported cases.6,7 Only one case of a female with nasopharyngeal actinomycosis mimicking a rhinolith with sinonasal complaints has been reported 5 . This contrasts the unique presentation of our case, a middle-aged man with throat pain and chronic cough for more than one year in the absence of sinonasal symptoms.
Due to the continuous and progressive spread, as well as formation of abscesses, a clinician must thoroughly work up suspected actinomycosis to rule out common mimics such as malignancy, tuberculosis, or nocardiosis.4,6 Isolation of Actinomyces spp. from clinical specimens through bacterial cultures and pathology is the gold standard for diagnosis of actinomycosis.3-8 Due to its indolent growth and requisite anaerobic environment, this is often difficult to achieve, which possibly explains why only 10% of actinomycotic infections are correctly diagnosed at the time of initial presentation.6,7 Visualization of gram positive, branching, filamentous rods under H&E staining supports the histopathologic diagnosis while special stains such as GMS are often required. 7 Treatment strategy and duration varies depending on the site of infection and adequacy of debridement. Penicillin G or Amoxicillin are administered for 2-12 months due to the chronic nature of actinomycotic infections.4,6,7
This case demonstrates an actinomyces rhinolith incidentally found in a patient with no sinonasal complaints. This case highlights the extra-laryngeal considerations in the differential diagnosis of chronic cough and throat pain. An exam which often focuses on the larynx, this case supports the role of flexible laryngoscopy and the examination of sinonasal anatomy at the same time. It is important to consider actinomycosis in the differential diagnosis when a heterogenous hard partially calcified mass is encountered in the nasal cavity as the treatment is different than that for the more typically encountered mycotic mycetoma, or fungus ball.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.