
Abstract
Objective
To explore the effect of cold-water irrigation on post-tonsillectomy pain after coblation.
Methods
Data from 61 adult patients who underwent coblation tonsillectomy in our hospital from January 2019 to December 2020 were collected, and the patients were randomly divided into the cold-water irrigation group (Group 1) and the room-temperature irrigation group (Group 2). Group 1 was irrigated with ice water mixed saline with the help of a pressure band, and Group 2 was irrigated with room-temperature saline. During the operation, we monitored the temperature of the operating cavity in real time. We recorded the postoperative pain for 11 consecutive days from the day and the 10th day after the operation.
Results
The postoperative pain score was significantly lower than that in Group 2, except on the 2nd, 3rd and 7th and 8th days after the operation.
Conclusion
The perfusion of cold water during coblation tonsillectomy is helpful to reduce postoperative pain.
Introduction
Tonsillectomy has a long history. Surgeons have been trying to invent and improve surgical instruments and methods to ensure the safety of patients’ surgery and reduce the incidence of postoperative complications. 1 Postoperative complications of tonsil surgery mainly include postoperative bleeding and postoperative pain. The latter is more common, which will increase the number of days in the hospital, affect diet, and reduce the quality of life in the perioperative period. 2 Exploring potential ways to reduce postoperative pain will help to improve this situation.
There are several tonsillectomy methods, including traditional tonsillectomy, which relies on so-called “cold-knife” dissection; tonsillectomy with the assistance of a CO2 laser or ultrasonic instrument; and electrocautery excision methods such as monopolar or bipolar instruments and coblation techniques.3,4 Radio-frequency coblation tonsillectomy has been gradually recommended and popularized in recent years. 4 Its main principle is to use a low-frequency current of approximately 100 kHz to excite electrolytes such as NaCl into “low-temperature plasma” with energy, which directly splits biological macromolecules such as proteins into O2, CO2, N2, and other gases to achieve tissue resection or coagulation. 5
Previous studies have shown that the main advantages of coblation tonsillectomy are less bleeding during the operation, shorter operation time, less pain 24 hours after surgery, and reduction of primary postoperative bleeding rate. 6 However, there are also controversies. Another study has shown that although the temperature due to coblation during surgery is cooled by room-temperature saline, it is still a relatively “hot and sharp” resection operation, and there are still several shortcomings, such as postoperative pain, longer recovery time, and slow pseudomembrane shedding. 7 Thus, surgeons should make greater efforts to reduce post-tonsillectomy pain. During the coblation operation, the plasma radio-frequency scalpel head is always irrigated with room-temperature saline but not with cold water. The effect of cold-water irrigation of the coblation site on post-tonsillectomy pain has not been prospectively studied. This study investigated and compared the effect of cold-water or room-temperature water irrigation of the coblation site on post-tonsillectomy pain.
Methods
General Information
The data of 61 adult patients who underwent coblation tonsillectomy in our hospital from January 2019 to December 2020 were investigated, including 24 males and 37 females aged 18–68 years, with an average age of 36.4 ± 12.8 years. None of the patients had postoperative bleeding. The study was approved by the Ethics Committee and the institutional review board of Beijing Chaoyang Hospital, and all patients signed the informed consent form. The inclusion criteria were as follows: (1) adult patients with chronic tonsillitis aged over 18 years; (2) patients who underwent coblation tonsillectomy; and (3) patients undergoing bilateral tonsillectomy. The exclusion criteria were as follows: (1) refusal to participate in the clinical trial; (2) acute tonsillar infection; and (3) pediatric patients.
Surgical Treatment
All cases included in this study were completed by the same surgeon (Mo Liu) to avoid research bias due to differences in the level of the surgeons. All patients were randomly divided into 2 groups: the cold-water irrigation group (Group 1, 38 patients) and the room-temperature irrigation group (Group 2, 23 patients). For Group 1, ice water mixed 0.9% saline (Figure 1A, yellow arrow) was applied, while a pressure band was used to ensure the output of cold water (Figure 1B). To ensure the temperature of the saline, 500 ml 0.9% saline was placed into the freezing layer of a refrigerator the day before surgery and removed 2–4 hours before the operation to reach its ideal state—saline with a small amount of ice block. Group 2 was irrigated with normal saline placed under a room-temperature environment, while the water temperature was kept at 23∼24°C. During the operation, the temperature of the operative cavity was measured, the temperature change was monitored in real time (Philip, Germany, Figure 1C and 1D), and the nasopharynx temperature monitoring tube was used for intraoperative real-time temperature monitoring (Figure 1E) to record the lowest and average temperature during the operation. Details of the cold-water irrigation group. (A) ice water mixed 0.9% saline (yellow arrow) and room-temperature saline (below); (B) a pressure band was used to ensure the output of cold water. (C) The temperature change was monitored in real time (red arrow); (D) connectivity electrode for temperature monitoring. (E) The nasopharynx temperature monitoring tube was used for intraoperative real-time temperature monitoring.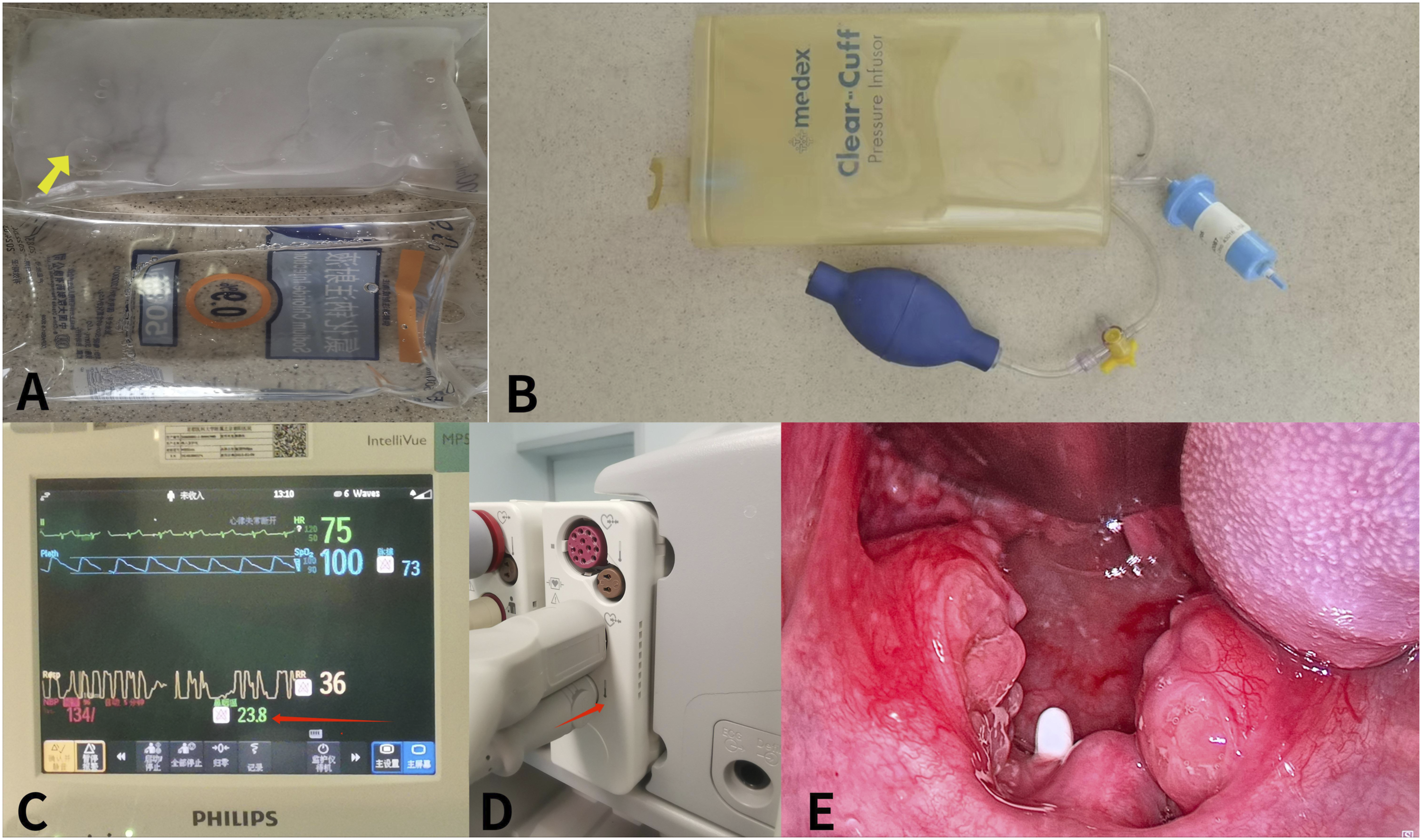
Perioperative Parameter Record
The perioperative parameters were recorded, including operative time, perfusion fluid temperature, preoperative pharyngeal temperature, and the mean, minimum, and maximum temperature of the operative cavity during surgery. The swelling of the uvula was recorded, which refers to visible uvula swelling to the naked eye at the end of the operation, and the congestion around the mucosa of the operation area at the end of the operation was also recorded. The volume of bleeding during tonsillectomy was evaluated.
Postoperative Pain VAS Score
Postoperative pain was evaluated with a visual analog scale (VAS) score. The VAS score range is 0–10, of which 0 represents no pain and 10 represents severe pain. The daily pain scores of the patients on the day and 10 days after the operation were recorded consecutively. As the average hospital stay of the patients was 3–5 days, after discharge, a daily follow-up telephone call was made to record the pain VAS score. All scores were recorded before the use of any analgesic drugs.
Statistical Methods
All statistical calculations were completed using SPSS 20.0, including measurement data such as age and operation time. The differences between groups were analyzed using an independent sample t test, the differences between counting data groups were analyzed using a cross table chi-square test, and the homogeneity of variance was used to test whether the data were in line with the square distribution. Spearman correlation analysis was conducted for the correlation analysis of various clinical features, and the difference was considered statistically significant when a P value was <0.05.
Results
General Demographic Data Statistics
Statistics of General Demographic Data of the 2 Groups (x ± s).

Group 1: The cold-water irrigation group; Group 2: The room-temperature irrigation group; BMI: Body mass index.
Intraoperative Parameter Differences Between Groups
Intraoperative Parameter Statistics of 2 Groups (x ± s).
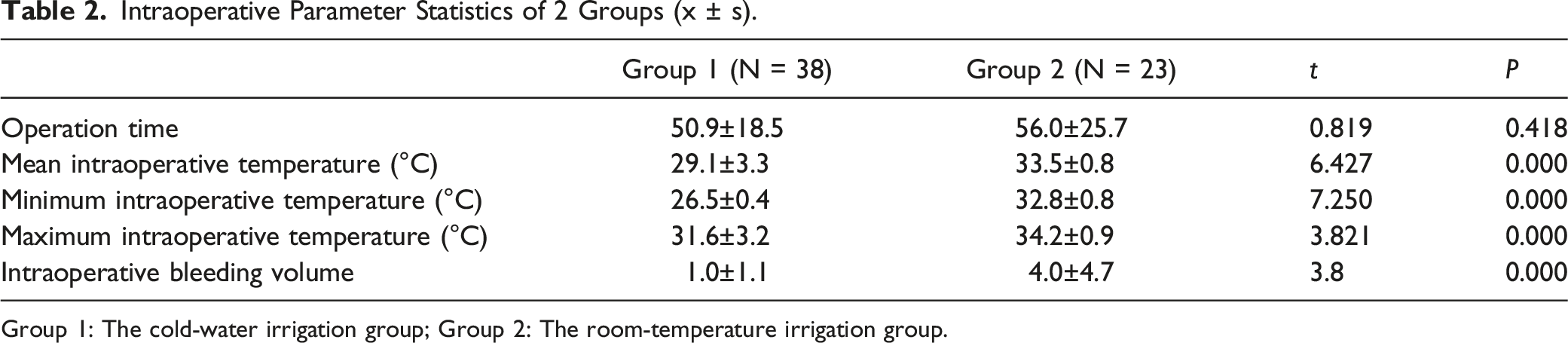
Group 1: The cold-water irrigation group; Group 2: The room-temperature irrigation group.
At the end of the operation, the incidence of uvula swelling in Group 1 was significantly lower than that in Group 2 (34.8% vs. 81.6%, χ2 = 13.607, P = 0.000), and the incidence of swelling of the surrounding mucosa was significantly lower than that in Group 2 (0.0% vs. 47.8%, χ2 = 24.681, P = 0.000). The intraoperative bleeding volume differences between the 2 groups infer that the intraoperative bleeding volume of Group 1 was significantly lower than that of Group 2 (4.0 ± 4.7 ml vs. 1.0 ± 1.1 ml).
Analysis of the Difference in VAS Scores at Different Times after the Operation
Statistics of VAS Parameters of Postoperative Pain in the 2 Groups (x ± s).
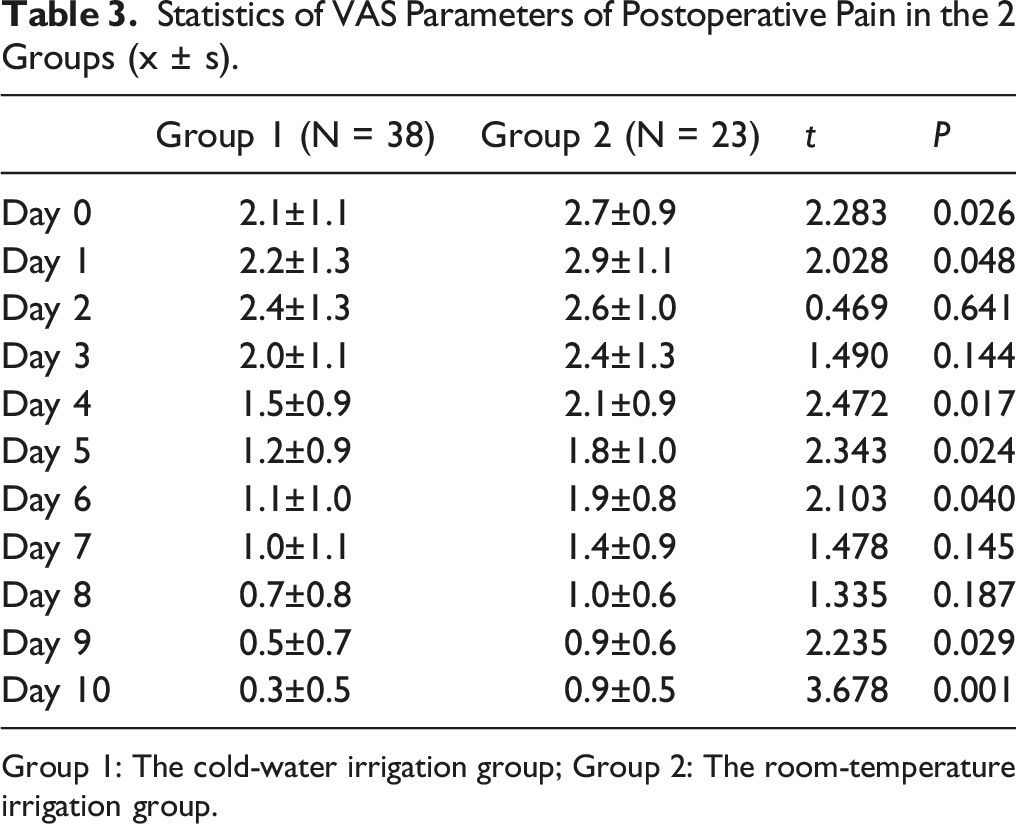
Group 1: The cold-water irrigation group; Group 2: The room-temperature irrigation group.
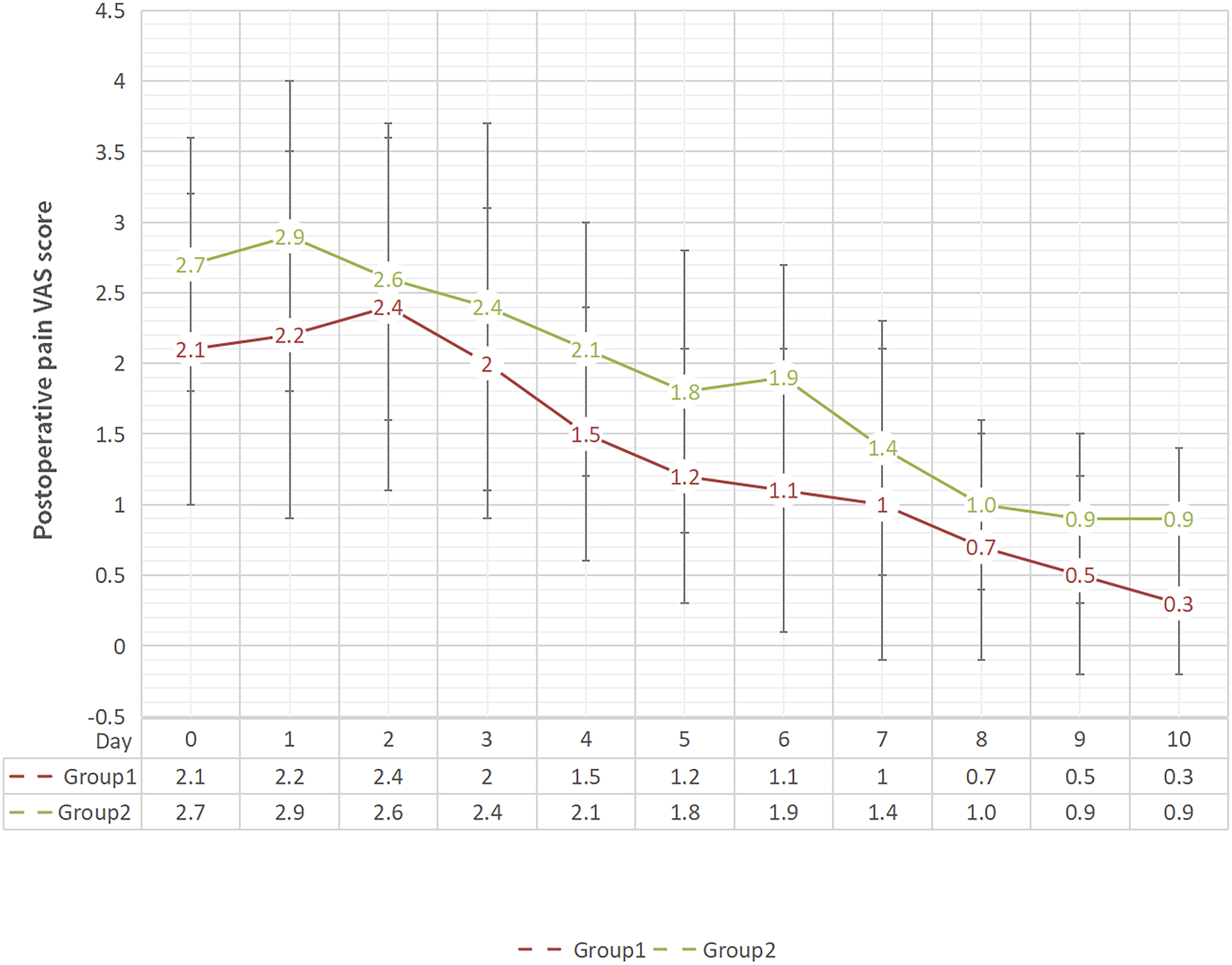
The trend of the postoperative pain VAS score of the 2 groups.
Discussion
Coblation technology has been widely used to perform tonsillectomy, and saline irrigation is necessary during such surgery. In this study, the temperature of intraoperative perfusion water was changed, and the temperature of the operative cavity of each patient was monitored in real time. The comparative study found that the use of ice water mixed saline for coblation irrigation during tonsillectomy could better relieve postoperative pain and reduce intraoperative bleeding.
The principle of coblation surgery is to stimulate the ion shock of tissue and cells through a strong radio-frequency electric field so that the electrolytes can be converted into an ionic state and form a plasma zone composed of highly plasma particles, accurately breaking the molecular bonds between tissue and cells. As these cells are broken and crushed, we can excise and ablate the diseased tissue. 5 Compared with other instruments, such as monopolar and bipolar electrocoagulation, the postoperative inflammatory reaction to tissues is less acute, and the postoperative recovery is faster. 8 However, although it is called “low-temperature,” cooled by room-temperature saline irrigation, the local temperature of the operative is still high in real time, and there is still a small heating effect on the surrounding tissues. In this study, ice water mixed saline was innovatively used to irrigate the tissue at a lower temperature, which was close to 0°C. The tissue temperature was kept at a lower temperature, while some heat was taken away through heat exchange, which further reduced its damage to the tissue and the postoperative inflammatory reaction.
The pain after tonsil surgery is mainly caused by stimulation of nerve endings, local inflammation after surgery, and traction and injury of myofibers below the tonsil.9,10 It has been indicated that immediately cooling the burn wound can reduce pain, inhibit tissue damage, and accelerate the wound healing process. 11 Similarly, immediately cooling the thermal damage caused by electrocoagulation on the tissue can also help postoperative wound healing and reduce postoperative pain.
Previous studies have shown that the use of coblation surgery, compared with the use of other electrosurgical equipment, has significantly reduced postoperative pain, which may be due to the gentle operation during the surgery, less traction and extrusion. Meanwhile, the thermal damage range of peripheral tissues caused by low-temperature operation is 1.29–1.59 mm2, which is rather small.5,6 The repeated squeezing of the pharyngeal constrictor muscle is reduced, the damage to muscle fibers is small, and the stimulation of nerve endings surrounding the tonsil, such as the vagus nerve and glossopharyngeal nerve, is small.5,6 Therefore, the postoperative pain is mild, the wound reaction is mild, and there is no obvious pharyngeal edema. 12 The coblation tonsillectomy group had a significantly reduced concentration of pain-inducing factor interleukin-1 (IL-1) and an increased concentration of pain relieving factor IL-8, which may be the reason for mild postoperative pain.12,13
However, whether there is any difference in the pain of patients after coblation tonsillectomy with saline irrigation at different temperatures remains unclear. This study found that the pain of patients after the use of ice water mixture saline irrigation was less, which may be related to the lower temperature that resolves the heat involved in the tissues in a timely manner, further constraining the thermal damage to the surrounding tissues and nerves and reducing the inflammatory reaction and the release of IL-1.11,12 The specific mechanism requires further experimental research.
In addition, studies have also found that at the end of tonsillectomy, the use of cold water to flush the surgical cavity can significantly reduce the postoperative pain of patients, including on the 1st, 2nd, 4th, 7th, and 10th days after surgery. It is suggested that cold water be used to cool the temperature of the tonsil fossa and pharyngeal mucous membrane during tonsillectomy. The study found that the principle may be to minimize tissue hyperthermia, reduce inflammation and reduce tissue necrosis through cooling. 13 The patients who had cold water for irrigation therapy had significantly less pain on the operation day and the 1st, 4th, 5th, 6th, 9th, and 10th days after the operation than those in the normal temperature group, indicating that the operation cavity was also flushed to a certain extent while the low-temperature plasma radio-frequency knife head was flushed, further reducing the postoperative pain of patients.
The advantages of this study are as follows: (1) Innovative use of ice water mixture saline, together with a pressure band, to achieve the purpose of using cold water for intraoperative irrigation and to reduce the real-time temperature of the surgical cavity. (2) This study found that when the temperature of the operating cavity is reduced, it actually helps to reduce the amount of intraoperative bleeding, reduce the postoperative pain, promote postoperative recovery, and improve the quality of life of patients during the perioperative period; (3) The postoperative pain score of the patients was monitored for 11 consecutive days from Day 0 to Day 10 after operation to more comprehensively evaluate the postoperative pharyngodynia of patients.
This study has the following limitations: (1) The patients who were included were from a single-center data, and there is an inevitable small bias in case selection. (2) All the enrolled patients in this study were operated on by the same clinician. In the future, tonsil surgery performed by doctors with different seniority levels should be observed to evaluate the impact of operators on the results of this experimental study. (3) The number of included cases is still small, and a larger sample size is needed for further research in the future to verify the results.
In conclusion, the results of this study found that the use of ice water mixed saline for irrigation during coblation tonsillectomy was indeed helpful in reducing the amount of intraoperative bleeding and postoperative pain in patients, providing a decision-making reference for clinicians when conducting coblation tonsillectomy.
Footnotes
Author Contributions
Drafting the manuscript: Mo Liu, Zufei Li. Acquisition of data: Zhitong Fan, Shuai He, Xinying Ge. Analysis of data: Zufei Li, Mo Liu, Shuai He, Xinying Ge, Yuanyuan Ren, Fei Xia. Revising the manuscript for important intellectual content: Zufei Li, Ningyu Wang, Cong Xu. Conception and design of the study: Cong Xu, Mo Liu, Zufei Li, Ningyu Wang.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All of the procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants and guardians included in the study.