
Abstract
Background
Diabetes is associated with a risk of idiopathic sudden deafness. The main treatment of diabetic sudden deafness is systemic and topical application of steroids. Topical steroid therapy reduces systemic adverse reactions compared with systemic therapy.
Purpose
The aim of this study was to conduct a meta-analysis design on the improvement value and recovery rate of pure tone mean hearing threshold (PTA).To investigate whether there is difference between local and systemic steroid treatment as the initial treatment for sudden deafness patients with diabetes.
Methods
We searched databases from publication date to October 1, 2022 including PubMed, EMBASE, Cochrane Library, web of science, CNKI, Wan fang Database, China Biomedical Literature Database (CBM), and VIP information resource system. A systematic literature review was conducted on the efficacy and safety of local and systemic steroid therapy for diabetic sudden deafness. RevMan5.4 and stata14 software were used for Meta-analysis.
Results
A total of 23 studies were included in this study, covering 1777 patients, including 885 cases in the observation group (local steroid group) and 894 cases in the control group (systemic steroid group). Meta-analysis showed that there was a significant difference in the total effective rate of local and systemic steroid treatment for diabetic sudden deafness between groups (RR = 1.17, 95% CI = 1.11-1.22, P < 0.05). The effective rate in the observation group was higher than that in the control group. For the improvement of PTA, the difference between groups was statistically significant (RR = 6.60, 95% CI = 3.07-10.14, P < 0.05). The improvement of PTA in the local steroid group was higher than that in the systemic steroid group. Subgroup analysis showed that there were significant differences between groups in hormones, drug administration, follow-up time and course of disease.
Conclusion
Topical steroid therapy is effective in the treatment of diabetic sudden deafness. Hormone methylprednisolone has high effective rate; the shorter the course of disease and the longer the follow-up time are, the higher the total effective rate will be. Tympanic injection is more effective than post-aural injection. Topical steroid injections are safer for hormonal side effect.
Keywords
Introduction
Idiopathic sudden deafness 1 is the full name of idiopathic sudden sensorineural deafness (hereinafter referred to as ISSNHL), also known as “sudden deafness,” which refers to sudden sensorineural hearing loss with unknown reasons within 72 hours, with hearing loss of at least 30 dBHL at 2 adjacent frequencies, and may be accompanied by tinnitus, ear tightness, numbness around the ear, dizziness, nausea, and vomiting. Epidemiology shows that the annual incidence rate of ISSNHL in the United States 2 is 5-20/100,000 people, and there are about 66,000 new cases every year. Incidence increases with age. Because of the different degrees of hearing loss, accompanying symptoms, basic diseases and treatment timing of patients, some patients have poor prognosis or even hearing loss cannot be recovered, which has seriously affected the normal work, life and learning. In order to carry out early and effective treatment to help patients recover, it is urgent to find a treatment method with high safety and effectiveness.
The etiology and pathophysiological mechanisms of ISSNHL have not been fully elucidated. Hearing loss can be caused by both local and systemic factors (i.e., vascular impairment disease, viral infection, rupture of the cochlear intima, autoimmune diseases, sexually transmitted diseases, tumors). ISSNHL is closely related to diabetes, and the incidence of diabetes has been increasing in recent decades. 35.1% of patients with diabetes have hearing loss. 3 Compared with the non-diabetic group, the incidence of ISSNHL in the diabetic group 4 was 1.54 times higher, and the risk of developing ISSNH increased with the severity of diabetes. Diabetes is a risk factor and poor prognostic factor for ISSNHL. Microvascular disease, a common complication of diabetes, is also an important factor leading to hearing loss. Animal experiments have shown that the atrophy of striatum in diabetic patients 5 is considered to be one of the possible causes of ISSNHL. Kumar et al. 6 pointed out that patients with diabetes had significant peripheral or central hearing and vestibular end organ damage. The treatment of patients with diabetic sudden deafness is still controversial clinically and there is no universally accepted protocol. Systemic and local steroid therapy has been proved to be effective; however, systemic corticosteroid administration in diabetic patients can lead to steroid-induced hyperglycemia, and glucose fluctuation can lead to the degeneration of potential auditory pathway 7 . Another treatment method for diabetic sudden deafness is local injection of steroids. Studies by Kakehata et al. 8 have shown that intratympanic dexamethasone treatment is at least as effective as systemic intravenous dexamethasone treatment for patients with diabetic sudden deafness. It has been pointed out by Zhang et al. 9 that the injection of methylprednisolone at acupoints behind ears can effectively improve PTA level and reduce blood glucose level of patients with diabetic sudden deafness. Thus, local injection of corticosteroids can not only increase local hormone concentration levels, but also reduce systemic adverse reactions.
At present, the most common treatment methods for patients with diabetic sudden deafness are systemic steroid shock treatment, steroid tympanic injection, auricular point injection and neurotrophic, improving inner ear circulation and other drug treatments in a short time after the onset of diabetes, which can also be used as an adjunct treatment of hyperbaric oxygen treatment. The US 2019 ISSNHL clinical guidelines 1 pointed out that patients with sudden deafness should use combination therapy, such as systemic (including oral, intravenous) and local (tympanic steroid injection) treatment. Local steroid (retroauricular and tympanic) administration is considered as the first-line treatment in accordance with the guidelines for sudden deafness in China. 10 Local treatments include auricular injection and tympanic injection. Therefore, tympanic injection and auricular injection were classified as local steroid therapy in this study. There is no unified standard for the route and type of local steroid administration so far, and no consensus has been reached on steroid treatment for diabetic sudden deafness. In view of the uneven clinical studies on local injection of steroids and systemic application of steroids to treat diabetic sudden deafness, we conducted a meta-analysis on the existing original literature to provide an evidence for steroid treatment for patients with diabetes combined with sudden deafness. We have conducted a rigorous screening of the literature from countries around the world, and only some articles of high quality in China were available for post-aural injection treatment.
Methods
Retrieval Strategies
The databases of PubMed, Cochrane, Web of Science, Embase, CBM, CNKI, VIP and Wan fang were retrieved by computer, and the retrieval formula was revised and improved according to the retrieval results. The published articles on local application of steroids and systemic application of steroids to treat diabetic sudden deafness in China and abroad before October 2022 were systematically and comprehensively collected. Chinese search terms: sudden deafness, idiopathic sudden deafness, sudden deafness, idiopathic sudden sensorineural hearing loss, sudden sensorineural hearing loss, and sudden sensorineural hearing loss; Steroid hormones, steroids, corticosteroids, glucocorticoids, hormones, methylprednisolone sodium succinate, dexamethasone, prednisone, budesonide, prednisone, methylprednisolone, methylprednisolone, diabetes, type 2 diabetes. The English search term is: Hearing Loss, Sudden; Sudden Hearing Loss; Deafness, Sudden; Sudden Deafness; Idiopathic sudden deafness; Sudden sensorineural hearing loss, SSHL; idiopathic sudden sensorineural hearing loss; Steroid; Steroids; steroids; corticosteroid; Corticosteroids; dexamethasone; prednisone; Methylprednisolone; budesonide; glucocorticoid; Diabetes Mellitus; Diabetes; type 2 diabetes.
Inclusion Criteria
Subject
This study was conducted in adult patient with ISSNHL in at least 2 patient groups, one receiving local steroid administration only as an initial treatment and the other receiving systemic corticosteroids. Inclusion in the study must be accompanied by diabetes mellitus regardless of race, age, gender, or course of disease. Studies reporting known causes of hearing loss such as stroke, nasopharyngeal carcinoma, acoustic neuroma, and Meniere’s disease were then excluded. To be included in this study, the study must report the mean pure tone hearing threshold (PTA) or the number of patients with successful outcomes.
Intervention Measures
Patients in the observation group were given glucocorticoid locally (including tympanic injection, Eustachian tube administration, and acupoint injection after ear), while those in the control group were given glucocorticoid systemically (orally or by intravenous drip). Other interventions were consistent, and routine treatment or not could be given at the same time.
Efficacy Evaluation Indexes
1. Recovery: The hearing of the impaired frequency returns to normal, or reaches the level of healthy ear, or reaches the level before the illness; 2. Marked effectiveness: the hearing with impaired frequency is improved by more than 30 dB on average; 3. Effective: The hearing at the impaired frequency is improved by 15-30 dB on average; 4. Ineffectiveness: The hearing loss frequency is increased by less than 15 dB on average. The effective rates of the local steroid administration group and the systemic steroid administration group were compared.
Exclusions
1. Previous treatment; 2. Patients with other systemic diseases that cannot tolerate hormone therapy; 3. Repetitively published literature; 4. No control group test; 5. Animal research and non-clinical trials on pharmacology, pharmacokinetics and adverse drug reactions; 6. In case of insufficient data, the authors of the main study were contacted and the study was excluded if no answer was provided.
Literature Screening, Data Extraction, and Bias Risk Assessment for Inclusion in the Study
The original data included in the literature for this systematic evaluation were independently extracted by 2 reviewers (Wang and Zhao). In case of disagreement, discuss the ruling with the third party (Chen). According to the PICO principle, the final evaluation results were shown in Risk of bias graph and Risk of bias summary. Tables were made and the original data in the literature were extracted from the research proposals and inclusion criteria of each study, including ① basic information of the inclusion study, such as study title, name and nationality of the author, and the time of publication of the magazine. ② Basic characteristics of the subjects, including sample size, age, gender, onset time, mean hearing threshold before onset, and blood glucose level in each group; ③ Treatment method, treatment effect, follow-up time and adverse reactions of the intervention measures; ④ Key elements of bias risk evaluation; ⑤ Interested outcome measures and outcome measures, such as PTA threshold, standard deviation (SD), PTA improvement and standard deviation after treatment, and the number of patients who recovered completely in each group.
Statistical Methods
The extracted Meta were subjected to meta-analysis using RevMan5.4 and Stata14.0 software. Heterogeneity of included articles was examined. If P > 0.1, I2 < 50%, indicating no heterogeneity, the fixed effect model was adopted. If P ≤ 0.1, I2 ≥ 50% the random effect model was used. The Relative risk (RR) and the 95% Confident interval (CI) mean difference (in dB) of PTA between the 2 categorical data were calculated.
Subgroup Variable Analysis
The following potential subgroup variables were also analyzed: steroid type, follow-up time, course of disease, and mode of administration.
Results
Literature Retrieval and Screening Results
As of October 2022, the literature retrieval and screening results were completed according to the flow chart of systematic article collection (see Figure 1). A total of 661 literature articles were retrieved. Unrelated articles were excluded from the articles with reading titles, and the abstracts and full-text articles that were repetitive and did not meet the inclusion criteria were read. Two articles were not included because the original text was not found, and finally 23 randomized controlled studies were included. Flow chart of the included articles.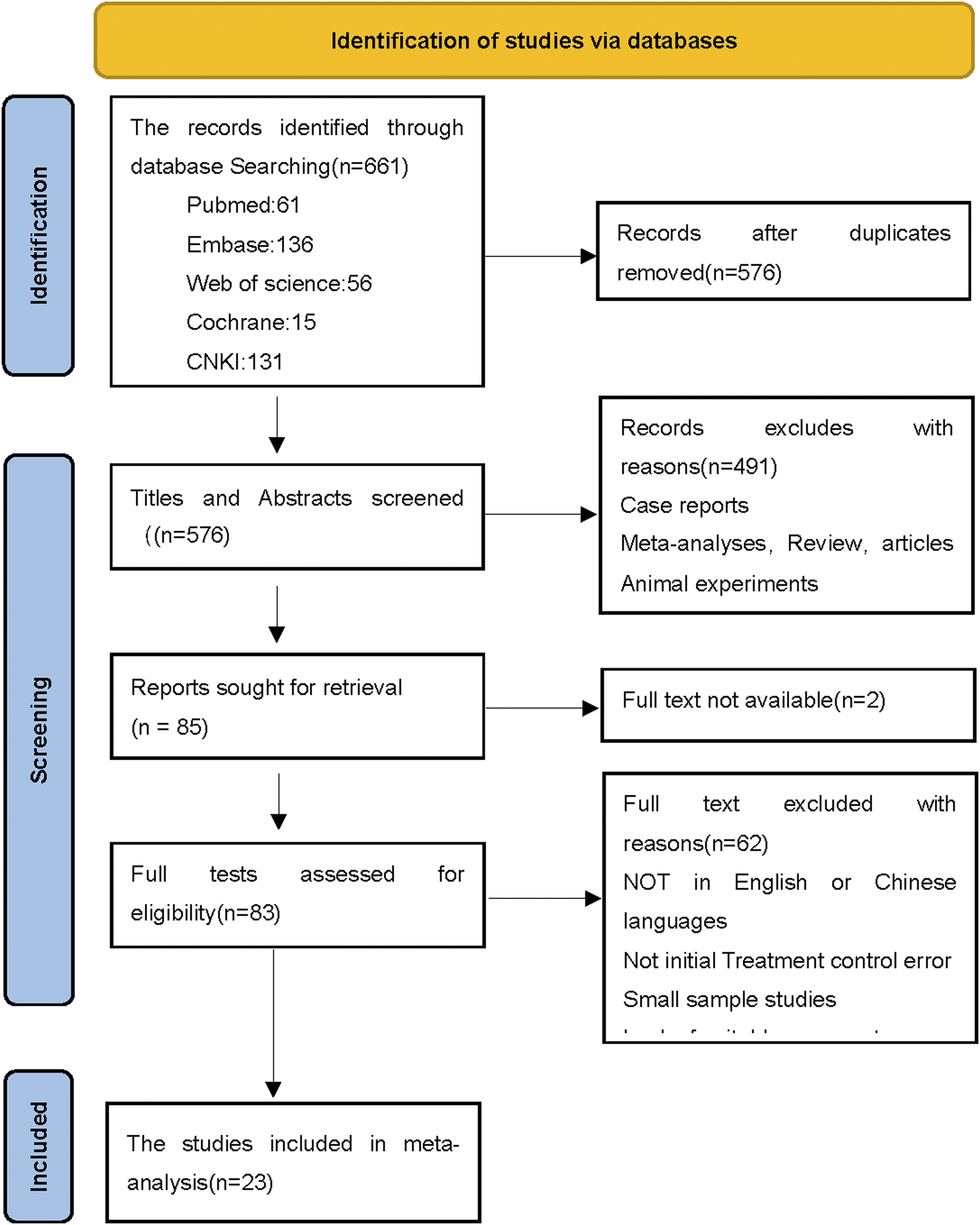
Basic Characteristics of Inclusion Studies and Results of Bias Risk Assessment
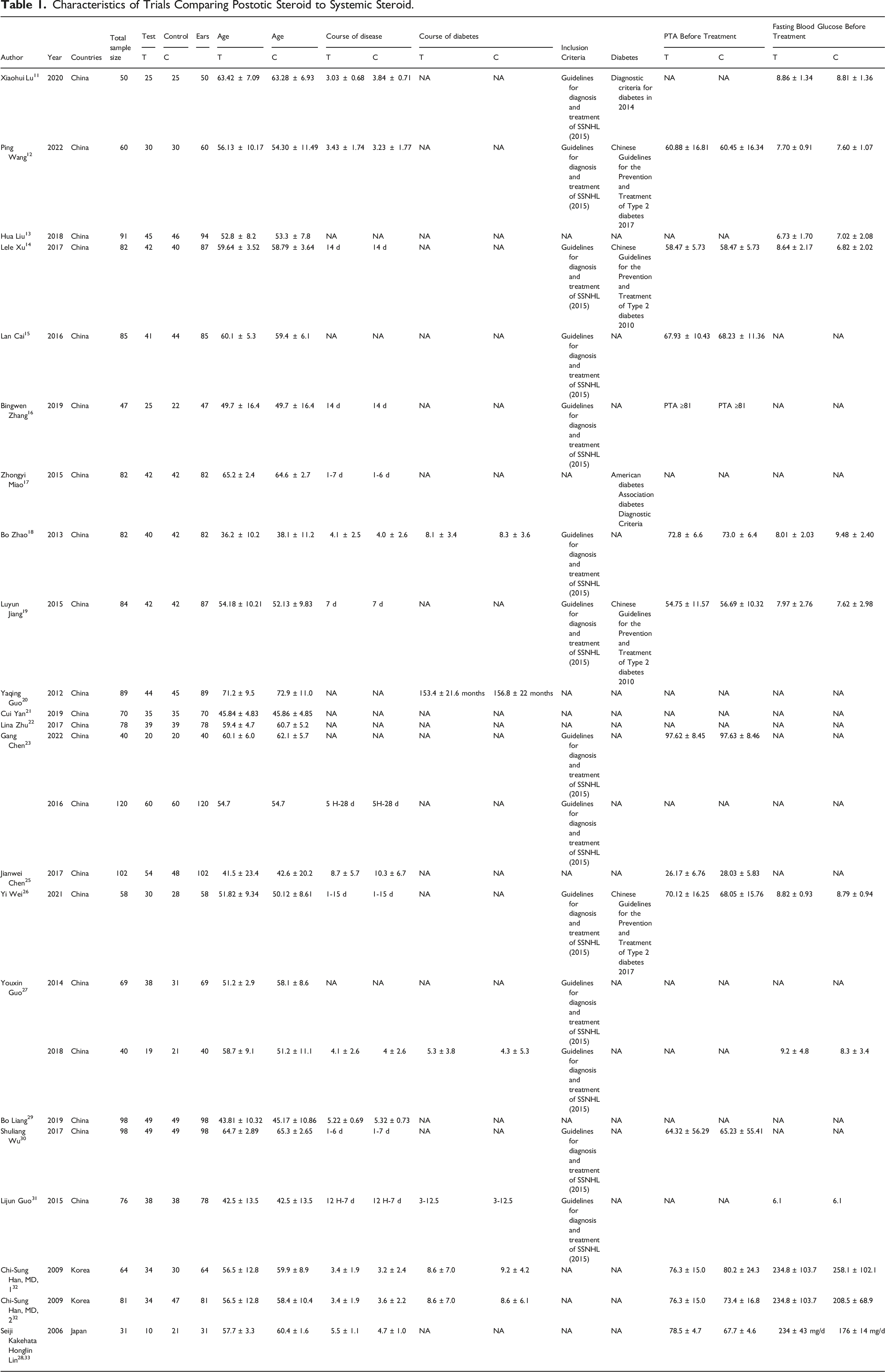
Characteristics of Trials Comparing Postotic Steroid to Systemic Steroid.
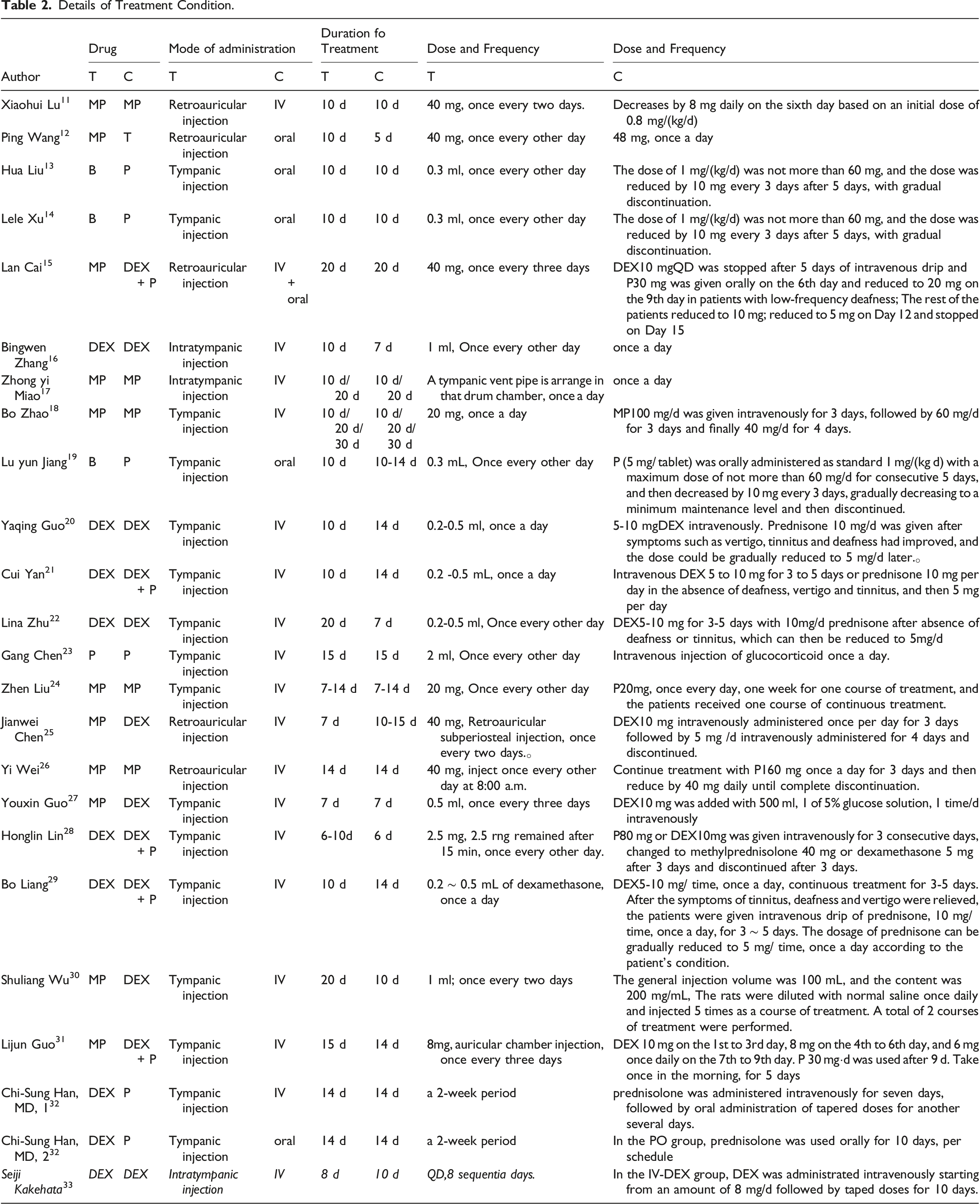
Details of Treatment Condition.
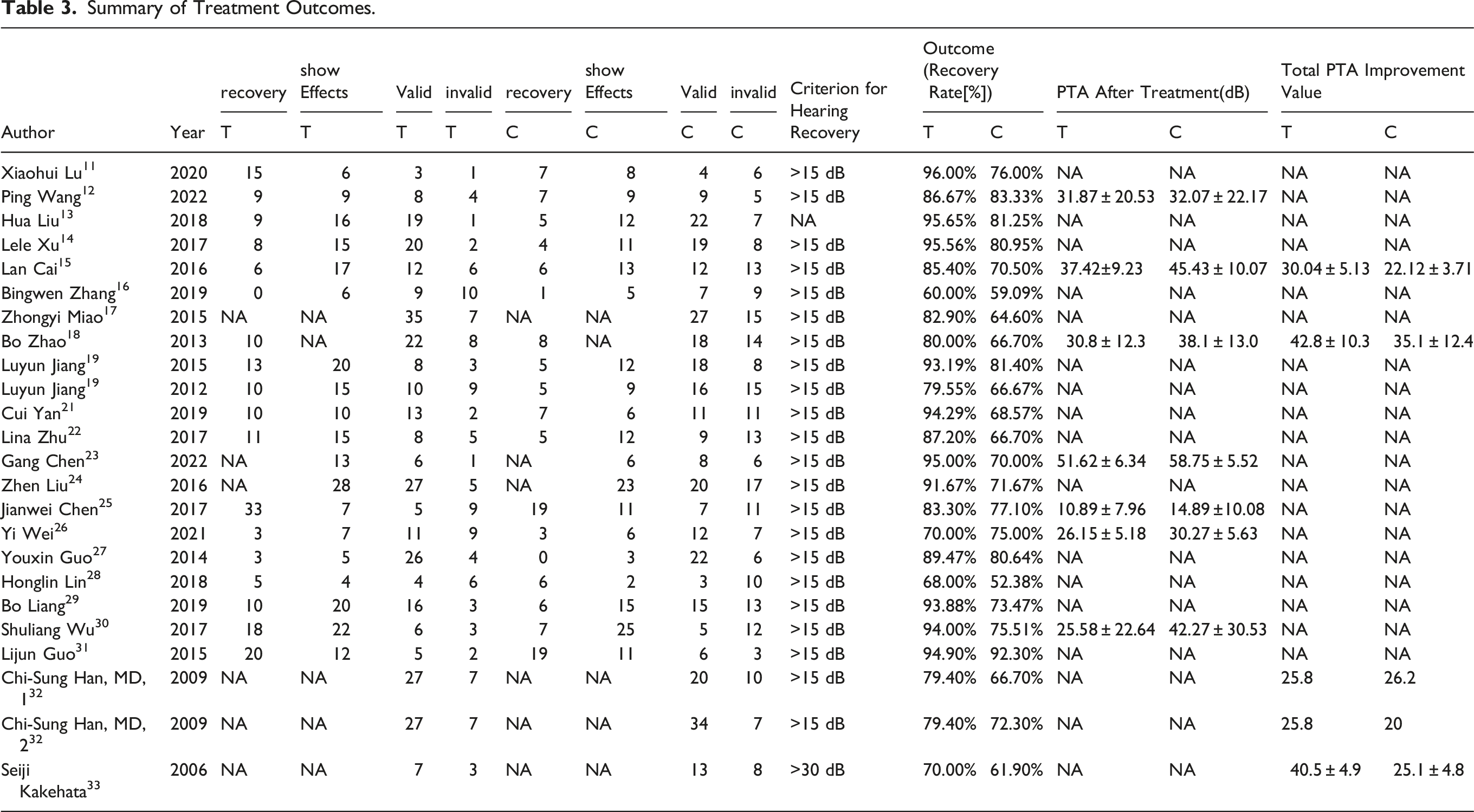
Summary of Treatment Outcomes.
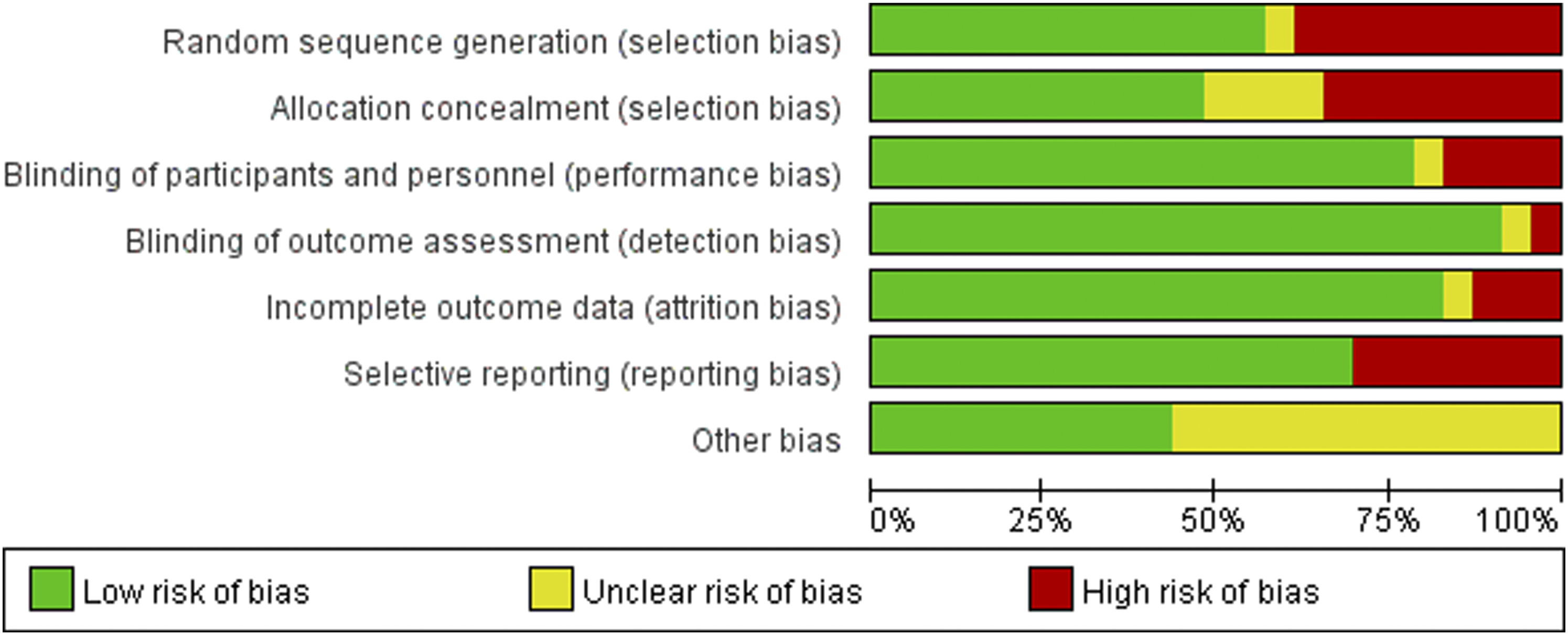
Risk of bia graph. Review authors’ judgments about each risk of bias item presented as percentages across all included studies.
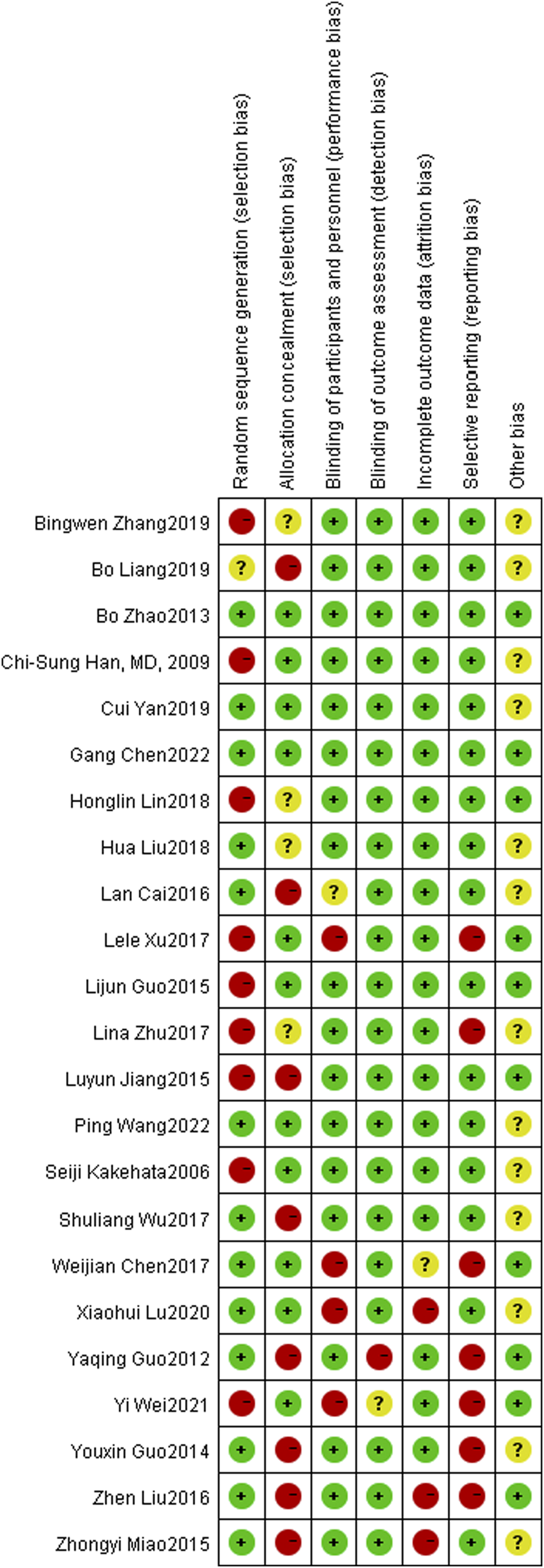
Risk of bias summary: Review authors’ judgments about each risk of bias item for each all included study.
Evaluation of Included Literature Quality
The Cochran Handbook5.0 was adopted to evaluate the literature quality, and the overall literature research quality was good. Baseline data were comparable, and there was a high risk of selective bias in the literature. The risk assessment table for literature evaluation is shown in Figure 2-3.
Comparison of the Total Effective Rates of Local and Systemic Steroids in the Treatment of Diabetic Sudden Deafness
A total of 23 articles (Figure 4) were covered, covering 891 cases in the local observation group and 885 cases in the systemic control group. P = 0.07, I2 = 32% in the heterogeneity test, and there was homogeneity among the studies, and fixed effect model analysis was used. The results showed that the difference between the local steroid observation group and the systemic steroid control group was statistically significant, with RR = 1.17 CI = 1.11-1.22, P < 0.05. The local steroid observation group was more efficient than the systemic steroid control group in the treatment of diabetic sudden deafness. The funnel plot was symmetrical, indicating that the publication bias was small (Figure 4). Forest chart and funnel chart of total effective rate comparison between local and systemic steroids in the treatment of diabetes sudden deafness.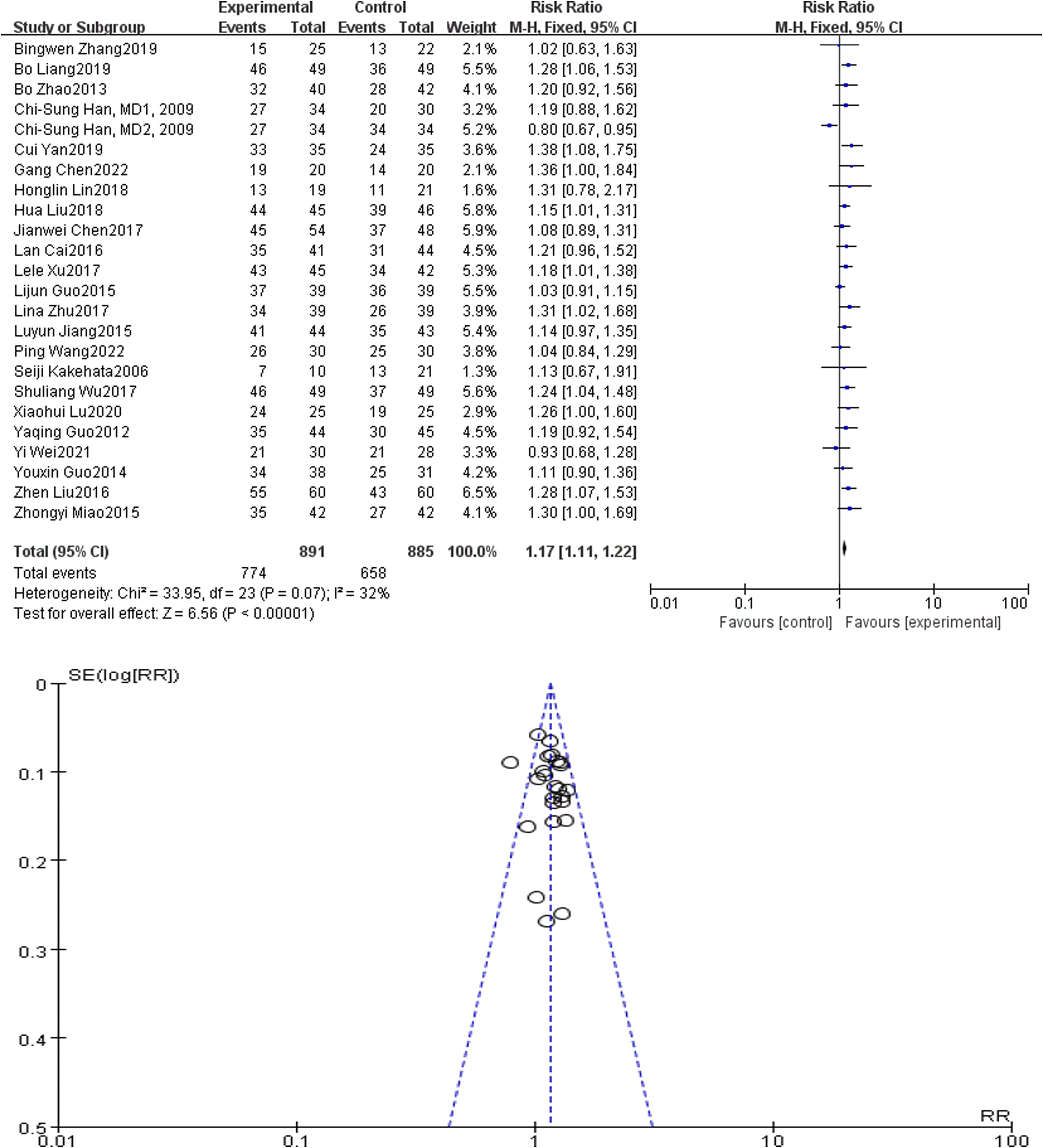
Comparison of PTA Appreciation
Nine articles (Figure 5) were included, all of which covered the total effective rate of treatment, including 342 cases in the local treatment group and 346 cases in the systemic hormone treatment group. P < 0.05, I2 = 74% for heterogeneity test, and random effect model analysis was used. The results showed that the difference in PTA increment after treatment between the local hormone treatment group and the systemic hormone treatment group was statistically significant, with RR = 6.60 CI = 3.07-10.14, P < 0.05. The local hormone treatment group was more effective than the systemic hormone treatment group in PTA increment. The funnel plot was symmetrical, indicating that the publication bias was small (Figure 5). Forest diagram and funnel diagram of PTA increment comparison between local and systemic steroids for diabetes sudden deafness.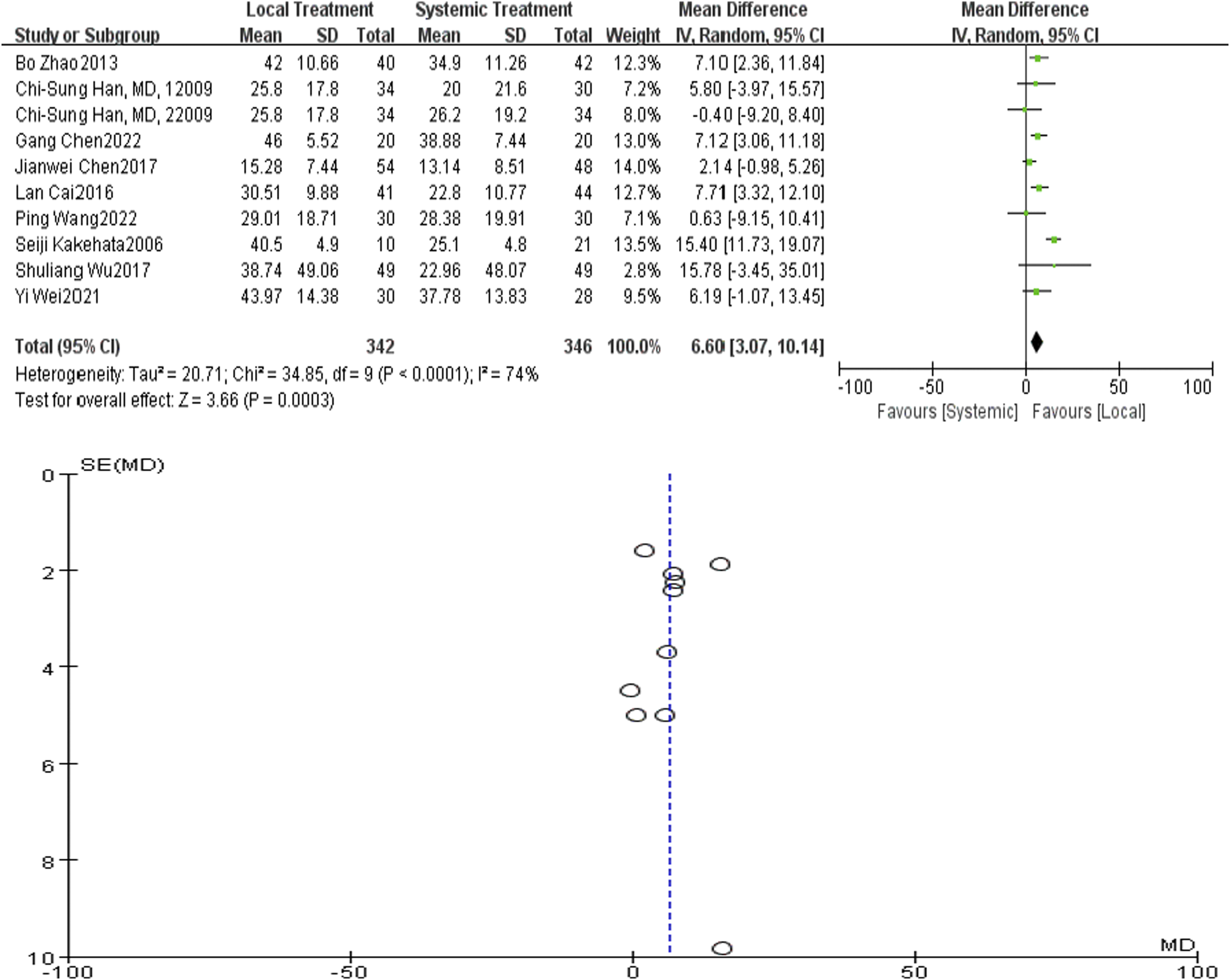
Subgroup Analysis
Comparison of Local and Systemic Steroids in the Treatment of Diabetic Sudden Deafness in Different Courses
They were grouped according to the course of disease in the general data, which was divided into 7 days and 14 days after onset. A total of 16 articles were included in the meta-analysis for different courses of disease, including 12 articles in 7 days, 4 articles in 14 days, and 1 article in 20 days. Study with different courses of disease (P = 0.01, I2 = 55%; P = 0.55, I2 = 0%), overall P = 0.05, I2 = 41%, so the fixed effect model was used. The results showed that there were significant differences in the efficacy of diabetic sudden deafness in patients with different courses of disease (P < 0.05), as shown in Figure 6. Forest map of comparison of local and systemic steroids for diabetes sudden deafness patients in different course of disease.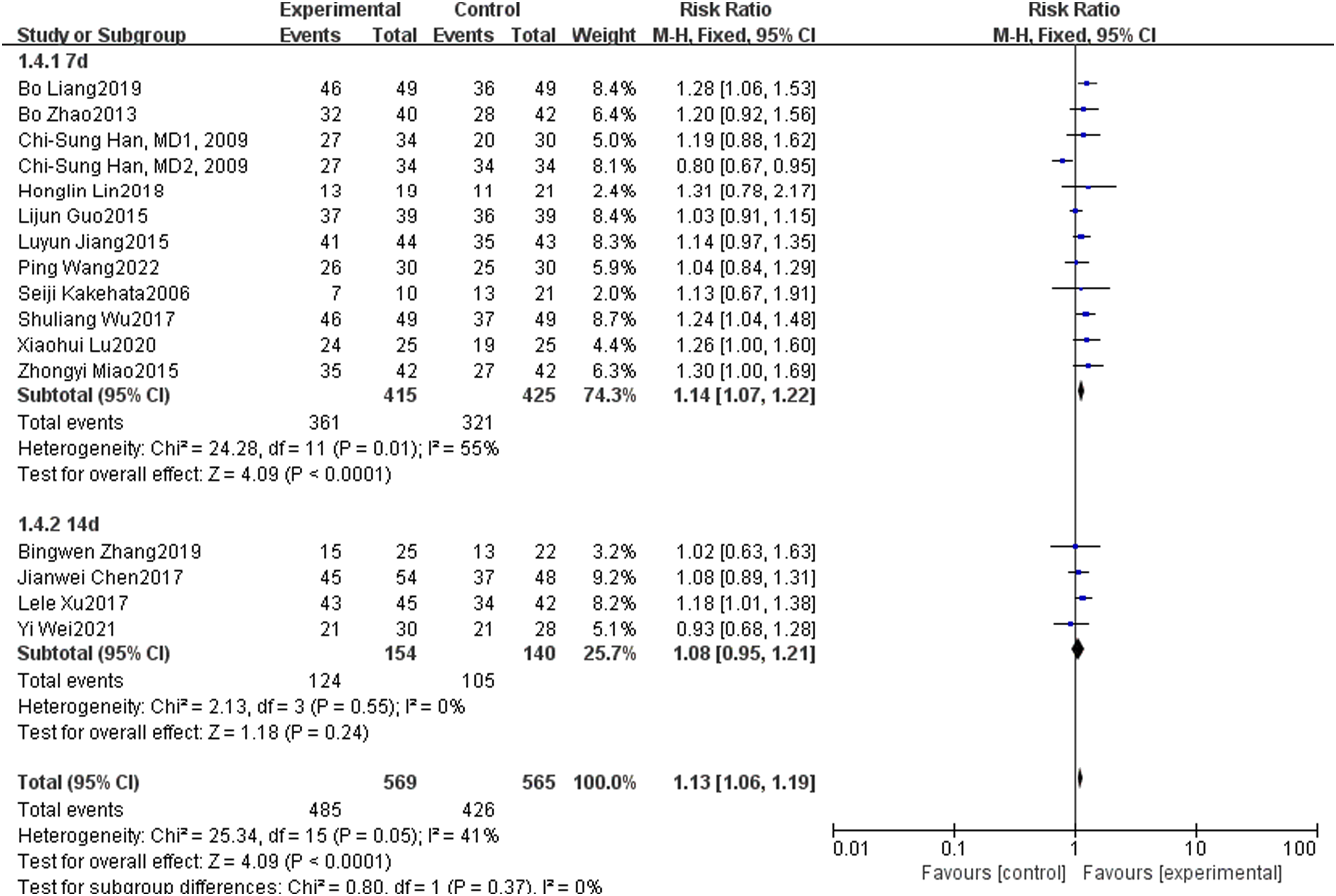
Comparison of Different Follow-Up Times for Patients with Diabetic Sudden Deafness Treated with Local and Systemic Steroids
The patients were grouped according to the follow-up time in general data, including 7-10 days, 14-15 days, and 20 days or more. A total of 23 articles were included in the meta-analysis with different follow-up times, including 8 articles with 7-10 days, 12 articles with 14 days, and 3 articles with more than 20 days. Study with different follow-up time (P = 0.95, I2 = 0%; P = 0.002, I2 = 62%; P = 0.92, I2 = 0%;), the overall P = 0.05, I2 = 35%, so the fixed effect model was used. The results showed that there were significant differences in the curative effects of sudden deafness among different follow-up times (P < 0.05). See Figure 7. Forest chart of comparison of local and systemic steroids treatment for diabetes sudden deafness patients in different follow-up time.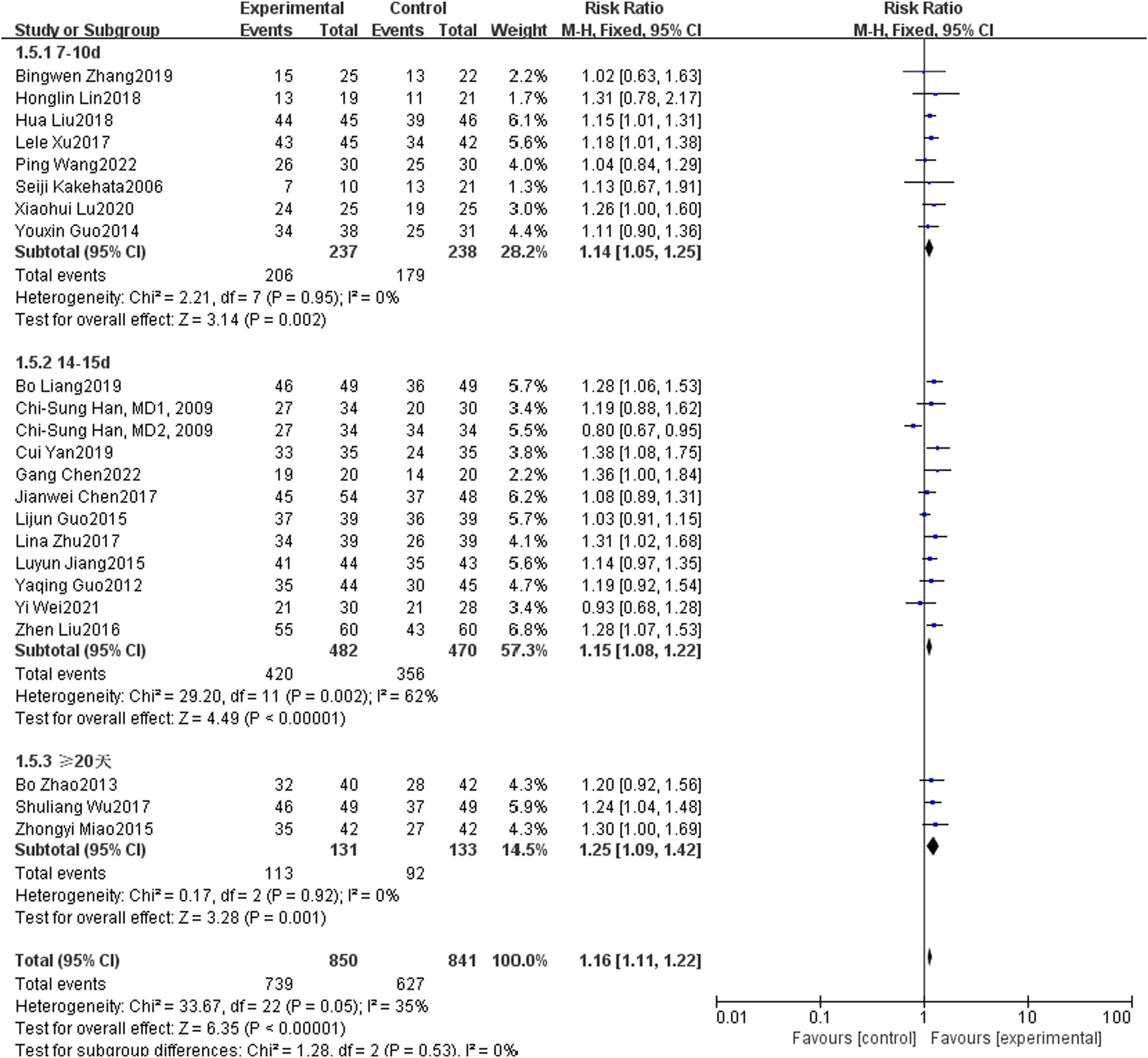
Comparison of Different Administration Routes of Local and Systemic Steroids for the Treatment of Diabetic Sudden Deafness
According to the different ways of local hormone administration in the general information, they were divided into the post-aural injection group and the tympanic injection group. A total of 23 articles were included in the meta-analysis for different follow-up times, including 5 articles in the post-aural injection group and 18 articles in the tympanic injection group. Study with different follow-up time (P = 0.51, I2 = 0%; P = 0.03, I2 = 42%), overall P = 0.07, I2 = 32%, so the fixed effect model was used. The results showed that there were significant differences in the efficacy of different hormone administration methods in the treatment of sudden deafness (P < 0.05). See Figure 8 Forest map of comparison between local and systemic steroids in the treatment of diabetes with sudden deafness in terms of different administration routes.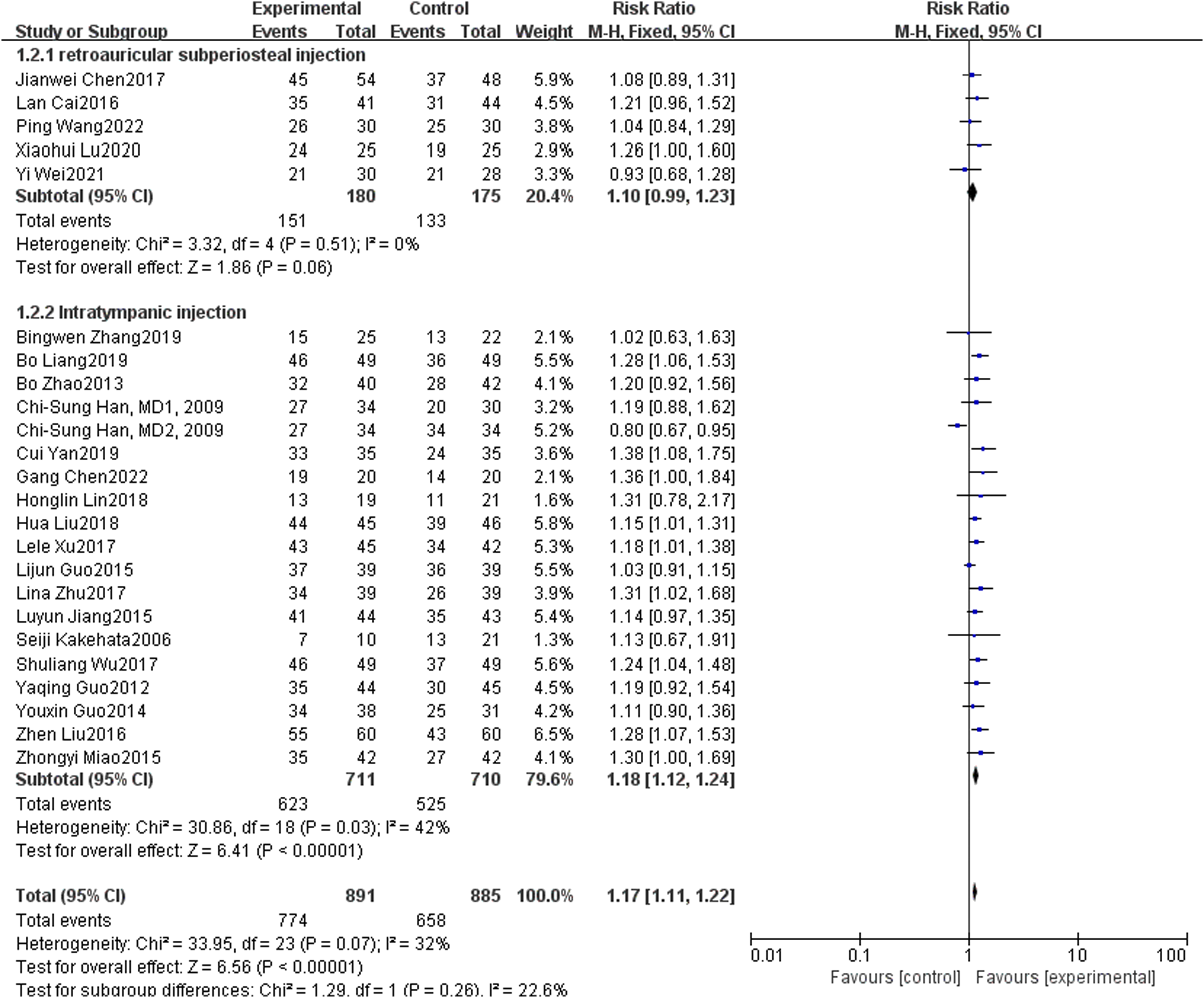
Comparison of Different Hormone Types between Local and Systemic Steroids for the Treatment of Diabetic Sudden Deafness
According to the different types of local hormones in the general Meta, they were divided into the dexamethasone group, methylprednisolone group, and budesonide group. A total of 22 articles were included in the meta-analysis at different follow-up times, including 8 articles in the dexamethasone group, 11 articles in the methylprednisolone group, and 3 articles in the budesonide group. Study with different follow-up times (P = 0.006, I2 = 63%; P = 0.38, I2 = 7%; P = 0.96, I2 = 0%), overall P = 0.07, I2 = 32%, so the fixed effect model was used. The results showed that there were significant differences in the efficacy of different kinds of hormones in the treatment of sudden deafness (P < 0.05). See Figure 9. Forest map of comparison of different hormone types between local and systemic steroid treatment for diabetes patients with sudden deafness.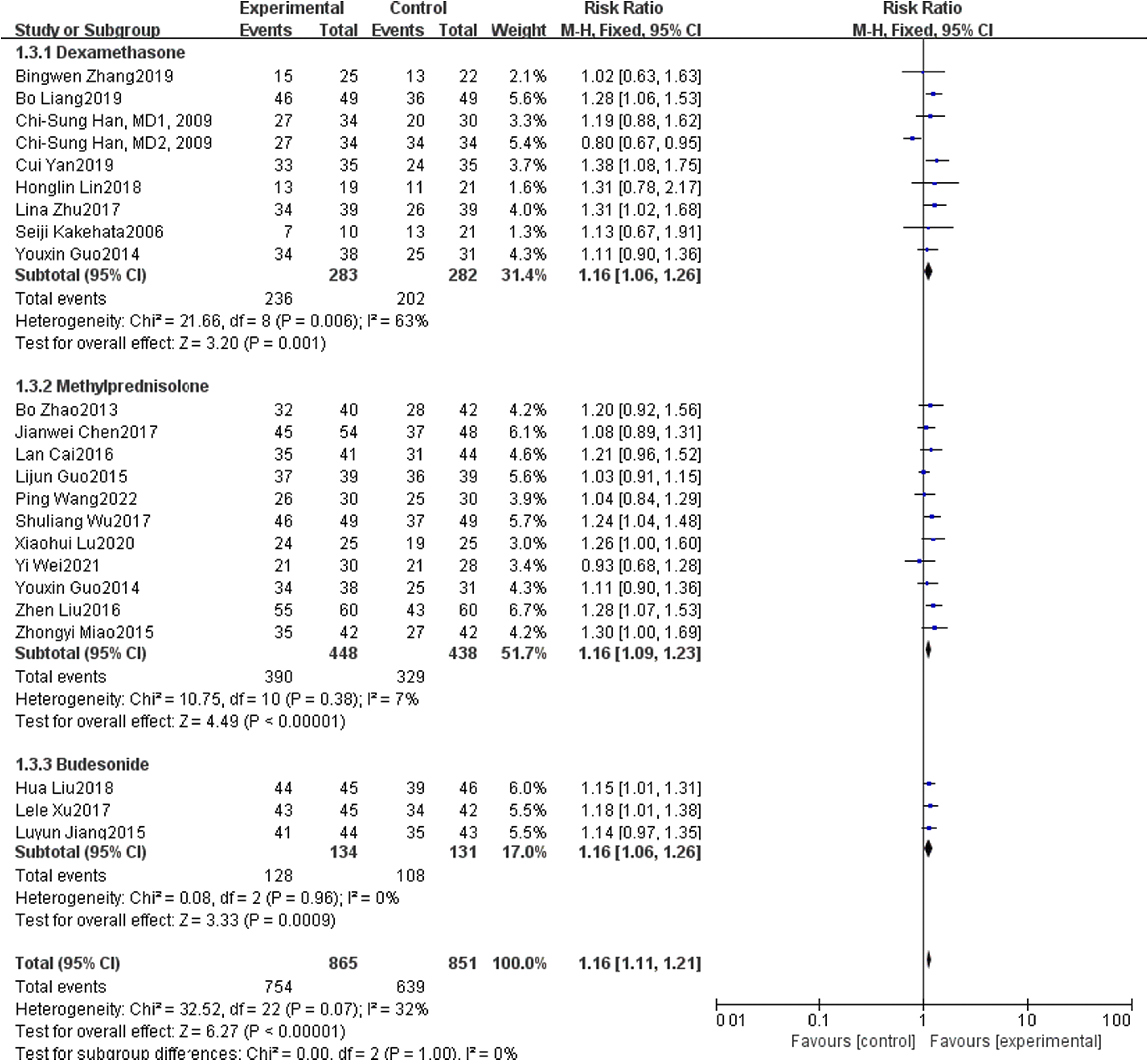
Safety
Nine articles reported the adverse reactions of local hormones, mainly including slight pain behind ears, ear itching, and transient vertigo. In the observation group, there were 29 cases of ear pain and 9 cases of ear itching. 12 cases of transient vertigo; 1 case had ear paralysis, 1 case had insomnia and emotional disorder; there were 4 cases of middle ear infection and 3 cases of tympanic membrane perforation. There were 5 cases with abnormal blood glucose and 1 case with elevated blood pressure. Adverse reactions to systemic hormone therapy have been reported in 6 articles, including 22 cases of abnormal blood glucose and 5 cases of ear paralysis; there were 5 cases of ear pain, 5 cases of otitis media, 3 cases of elevated blood pressure, 2 cases of gastric ulcer, and 2 cases of insomnia and emotional change.
Sensitivity Analysis
A sensitivity analysis was performed on selected studies to identify outliers that affected the overall results (Figure 10). We also excluded studies with a high risk of bias, and there were no substantial changes in the results. Sensitivity analysis.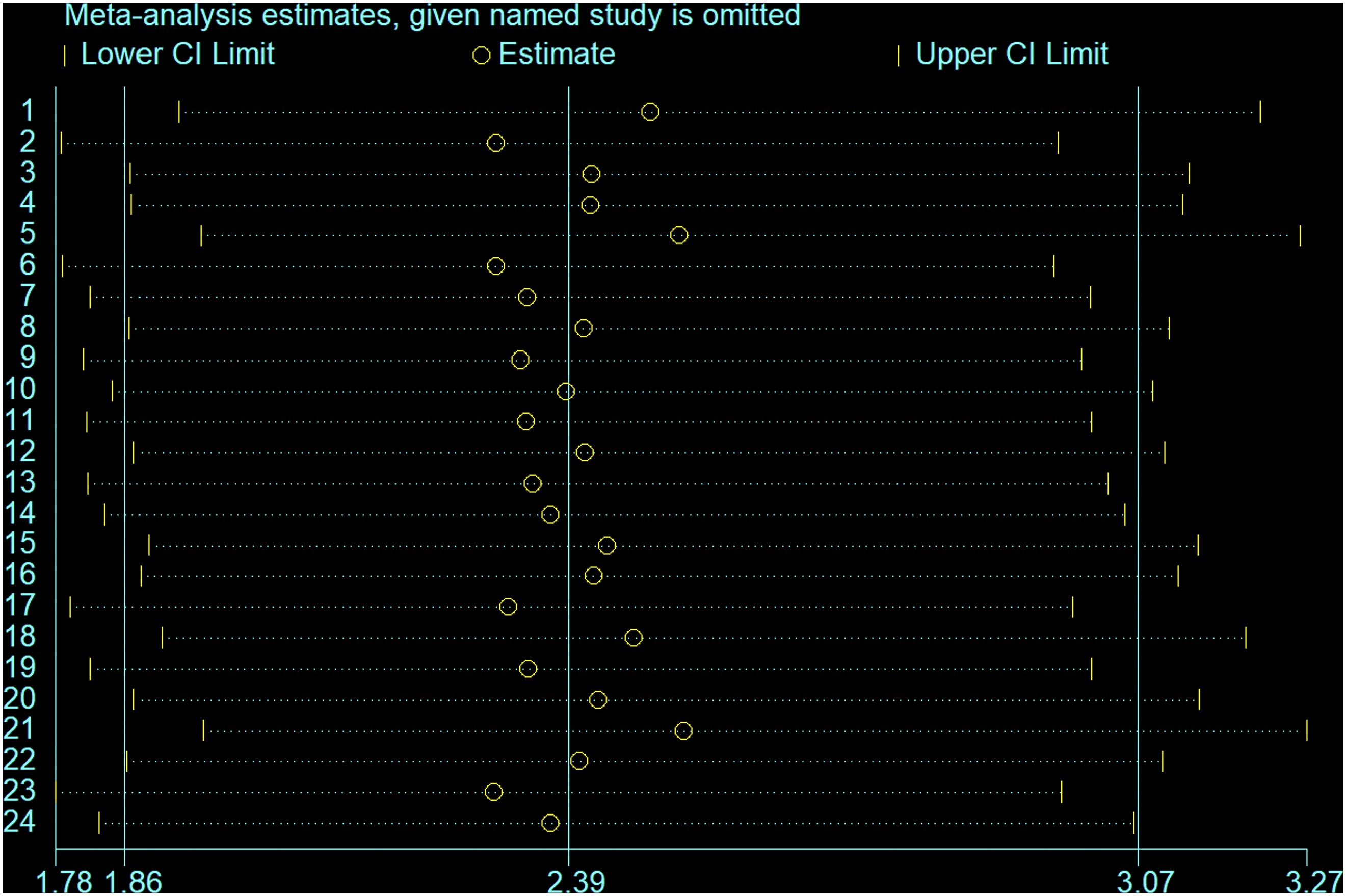
Discussion
ISSNHL patients with diabetes is a common sudden disease in otorhinolaryngology. The first-line therapy for diabetic sudden deafness is still the combination of steroids, nutritional nerves and drugs to improve circulation. Systemic steroid therapy is unable to avoid the blood labyrinth barrier of the inner ear, resulting in incurable or unsatisfactory results in some patients. However, local steroid therapy is favored by some doctors because it can avoid the side effects of systemic hormone administration. However, its efficacy is still controversial. There are many methods for local administration, including intratympanic injection, intratympanic administration after tympanotomy, postauricular subchondral injection, and intratympanic injection through eustachian tube. Intratympanic administration is a relatively recommended method in worldwide diagnostic and therapeutic guidelines. Post-aural injection has gradually become a research focus in the field of otology in China due to its advantages of minimal invasion, safety and high efficiency, and it was also taken as a supplementary treatment in the 2015 guidelines for the diagnosis and treatment of sudden deafness in China. Yang Xiao qi et al. 34 studied the treatment of sensorineural hearing loss by injecting compound betamethasone behind the ear for the first time, and confirmed that retroauricular administration can effectively treat intractable low-frequency sensorineural hearing loss. Li Jing jing Yu Li sheng, et al. 35 observed the drug administration after ear using magnetic resonance imaging, and the results showed that: the drug administration after ear can promote the drug to enter the inner ear. Compared with systemic administration, it is possible that the local action time of the inner ear is longer, and the total amount of drug is larger. It is easier for the drug to enter the internal lymph after post-aural injection, and finally it acts on the inner ear against the concentration gradient of internal lymph. Li Yu ming et al. 36 showed that tympanic injection and auricular injection were both effective methods for the treatment of diabetic sudden deafness, and the combined application had better effect. Therefore, local injection of glucocorticoids is effective and worthy of attention in the treatment of diabetic sudden deafness.
This study is the first to evaluate the efficiency, safety, and PTA improvement rate of local steroids and systemic steroids in the treatment of diabetic sudden deafness. This meta-analysis suggests that topical steroid therapy may be more effective in terms of efficiency and PTA appreciation. We also performed a subgroup study based on the efficiency and safety of several factors. First, we performed a subgroup analysis on the duration of the disease course, and the results showed that the shorter the course of the disease, the better the efficacy. Therefore, patients with diabetic sudden deafness need early treatment in order to obtain a better therapeutic effect. The second was a subgroup analysis of the different steroid dosing classes, which showed that methylprednisolone was the most effective topical steroid, followed by dexamethasone and budesonide suspension. This was related to the fact that methylprednisolone could pass through the round window membrane more effectively than dexamethasone, 37 with a shorter onset time and longer maintenance time. The third subgroup analysis was conducted on different steroid administration routes, and the results showed that steroid intratympanic injection was superior to auricular acupoint injection in efficacy. This may be related to the fact that intratympanic injection directly affected the inner ear and the concentration of the drug was higher. Fourth, subgroup analysis is performed for different follow-up times. The results show that the longer the follow-up time is, the higher the total effective rate will be. Therefore, local steroid administration for patients with diabetic sudden deafness can be used for supplementary treatment for patients with systemic steroid administration failure.
In terms of safety, topical steroids are more suitable for patients with contraindications to glucocorticoids, such as diabetes and gastric ulcers, because they avoid the side effects of systemic administration. The results of this meta-analysis showed that topical steroid administration had the following advantages over systemic steroid administration in the treatment of diabetic sudden deafness: blood glucose fluctuation was small, and other adverse reactions such as auricular pain, ear fullness, auricular itching, auricular paralysis, vertigo, and tympanic membrane perforation were also less. As the most common adverse reactions of intratympanic injection such as tympanic membrane perforation and vertigo were avoided by auricular acupoint injection, the safety of auricular injection was superior to that of intratympanic injection.
At present, scholars have conducted a large number of studies on the treatment of diabetic sudden deafness patients by local steroid administration and systemic steroid administration. However, due to the lack of high quality evidence-based medicine, various treatment methods and their efficacy still cannot be confirmed. The conclusions of the comparative studies on systemic application of steroids and local injection therapy are inconsistent, and the results of different Meta-analyses are also contradictory. Ying Li et al. 38 performed a meta-analysis and found that posterior auricular acupoint injection of glucocorticoids might be the most effective treatment, thus providing an evidence-based basis for hormone treatment in patients with sudden deafness of full-frequency and high-frequency descent pattern. A meta-analysis by Ting Yang et al. 39 found that topical steroids appeared to be superior to systemic steroid administration for the initial treatment of ISSNHL, especially in patients with contraindications for systemic steroids. Per capita studies by Mirian 40 and Mirsalehi 41 showed that there was no statistical difference between the efficacy of intratympanic corticosteroid injection and systemic approach in improving the hearing results of patients with ISSNHL. However, these meta-analyses failed to distinguish the diabetic patients from the general patients, so there was a certain heterogeneity, and no more detailed evaluation was conducted on the patients with diabetic sudden deafness in terms of effectiveness and safety. Therefore, we do not recommend steroid therapy for patients with diabetic sudden deafness. At present, no meta-analysis has been conducted on the effectiveness and safety of steroid treatment for patients with diabetic sudden deafness. Therefore, for the first time, we conducted a meta-analysis on the total effective rate, average meta improvement, different course of disease, different administration route, different hormones, different follow-up time and other indicators of local steroid and systemic steroid treatment for patients with diabetic sudden deafness, in order to provide a more detailed evidence-based medicine basis for clinical treatment of this disease.
Advantages
This is the first meta-analysis of local and systemic steroids for the treatment of diabetic sudden deafness, and a meta-analysis of its effectiveness, safety, meta appreciation rate and related subgroups (route of administration, type of steroid, onset time, and follow-up time). A total of 1777 patients were included in the 8 databases retrieved, including 885 cases in the observation group after local steroid administration and 894 cases in the control group after systemic steroid administration. The sample size was large, and the literature retrieval was comprehensive.
Limitations
This systematic evaluation clarified the effectiveness and safety of local steroids in the treatment of diabetic sudden deafness, but there were still some limitations, such as the small sample size and low quality of the included original literature materials, slightly insufficient experimental design, whether it was a randomized controlled study or not even listed in some articles, incomplete outcome data, etc. Although it has been clarified that intratympanic injection and postauricular injection of steroids are effective for the treatment of diabetic sudden deafness, there are still many problems to be solved, such as which drug is the best in safety, whether there is difference in curative effects due to different injection intervals, and whether different courses of diabetes and different initial blood glucose levels of diabetes affect curative effects, all of which need further subgroup analysis. Although the subgroup analysis in this paper indicates that tympanic injection is more effective than post-aural injection, it is a conclusion based on local and systemic comparison that the efficacy of post-aural injection is compared with that of systemic, tympanic injection and systemic injection, and the efficacy of retroauricular and tympanic injection is not directly compared. The last limitation is that articles about post-aural injection are all from China. This is because there are many studies on the treatment of sudden deafness by post-aural injection in China. We closely screened the literature of countries all over the world, and finally only some high quality literature from China. This is the objective limitation of this article. Compared with systemic administration, auricular injection has the advantages of less adverse reaction, early peak arrival time, high local drug concentration, and low systemic circulating blood drug concentration. Diao Tong xiang and Yu Li sheng et al. 42 showed that the possible route of post-aural injection was that the tracer firstly passed through local circulation and infiltration into the sigmoid sinus, and then entered the perilymph through the venation relationship between the sigmoid sinus and the endolymphatic sac, and finally acted on the inner ear against the concentration gradient of perilymph. Therefore, such a study should be conducted in all countries in the world in the future, so as to help us understand more clearly whether post-aural injection is effective for the treatment of sudden deafness, and which is better, post-aural injection or local injection. In order to further improve the effective rate and quality of life of patients with diabetic sudden deafness, further large-sample, multi-center and high quality RCTs are needed to provide a more reliable basis for clinical diagnosis and treatment.
Conclusion
The meta-analysis indicates that local steroid therapy is effective and safer in the treatment of ISSNHL patients with diabetes. The hormone methylprednisolone has the highest effective rate. The shorter the course of the disease is, the longer the follow-up time is, the higher the total effective rate is. Tympanic injection is more effective than post-aural injection. However, multi-center randomized controlled trial is needed to further clarify this mechanism and confirm our current findings.
Supplemental Material
Supplemental Material - Local vs Systemic Use of Steroids for Sudden Deafness with Diabetes: A Systematic Review and Meta-Analysis
Supplemental Material for Local vs Systemic Use of Steroids for Sudden Deafness with Diabetes: A Systematic Review and Meta-Analysis by Huanhuan Wang, Zhixiang Zhao, and Songyue Chen in Ear, Nose & Throat Journal
Footnotes
Author Contributions
Huanhuan Wang and Zhixiang Zhao designed the study and supervised the overall project. Songyue Chen and Huanhuan Wang participated in collecting and analysis. Huanhuan Wang and Zhixiang Zhao provided the statistical analysis and wrote the manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study does not involve animal and human participants. Our data are extracted from published papers that had received ethical approval, So previous researchers had helped us obtain qualified ethical approval and we did not need to apply for ethical approval again.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author. Data sharing not applicable to this article as no datasets were generated or analyzed during current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.