
Abstract
Objective
To analyze the clinical characteristics of differentiated thyroid cancer (DTC) patients with nasolacrimal duct obstruction (NLDO) after Iodine-131 (131I) therapy and provide guidance for clinical decision-making.
Methods
Thirty-one DTC patients with NLDO were retrospectively enrolled from the Nuclear Medicine Department of Shanxi Bethune Hospital during follow-up of 131I therapy between June 2018 and March 2021. Eight hundred and seventy-one thyroid cancer patients during this period without NLDO after 131I therapy were enrolled as the control group. Clinical characteristics, including sex, age, dose, anti-thyroglobulin antibodies (TGAb), and metastatic lesions, were analyzed by χ2 test and logistic multifactor regression.
Results
In the NLDO group and without NLDO group, there were statistically significant differences in gender, age, dose, and whether there was metastasis. Among the NLDO group, the proportion of women, age >55 years old, dose >5.55 GBq, and the presence of metastasis was higher, and the difference was statistically significant; There was no significant difference in the proportion of TGAb positive and negative patients based on 131I therapy (χ2 = 0.27, P = .782).Multivariate logistic regression analysis showed that sex (2.59), age (1.45), dose (2.36), and metastatic lesions (1.93) were all statistically significant influential factors of NLDO after iodine therapy. Significant differences were found in the incidence of NLDO between the number of treatment courses (χ2 = 23.541, P < .001). Prevalence rate of repeat radioiodine therapy (2 times or 3 times and more) is higher than 1 time.
Conclusion
Women patients over 55 who had metastatic lesions, and received a dose >5.55 GBq, were more likely to have NLDO. When determining therapeutic doses of 131I, doctors should weigh multiple factors and then give appropriate dosage and suggest that high risk populations be referred for appropriate ophthalmic surgical consultation, for timely diagnosis and therapy.
Keywords
Introduction
Thyroid cancer accounts for 3.6% of the world's malignant tumors and its incidence is increasing year by year. Since the 1940s, Iodine-131 (131I) therapy has been used as adjuvant therapy following thyroid cancer surgery. 1 The first dose of 131I for thyroid cancer patients can reach 1.11–7.4 GBq and many further rounds may follow, depending on the patient’s condition, leading to 131I accumulation. Multiple and high dose 131I has potential chronic side effects, such as chronic sialopathy, dry mouth, dry eye, chronic conjunctivitis, obstruction of parotid and/or nasolacrimal ducts, infertility, pulmonary fibrosis, myelodysplasia, and rare second primary malignant tumors.2-4 Estimates based on studies put the number of patients suffering ocular complications at 23% and nasolacrimal duct obstruction (NLDO) may have a causal relationship with iodine therapy and related clinical characteristics. The current study aims to analyze clinical characteristics of patients with NLDO after 131I therapy for differentiated thyroid cancer (DTC), to provide guidance for clinical decision-making.
Materials and methods
Research participants and grouping
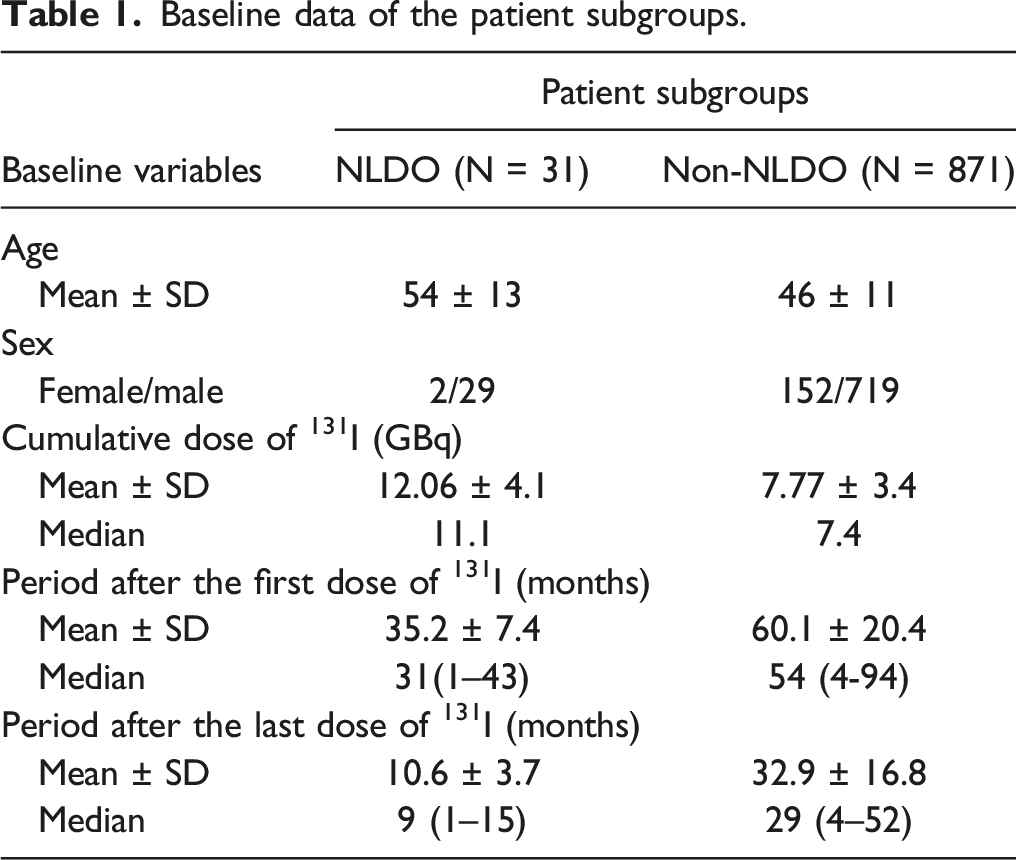
1. Patients: Between June 2018 and March 2021, 31 patients having thyroid cancer with NLDO (the symptom is lacrimation) were selected during follow-up of 131I therapy in the Department of Nuclear Medicine, Shanxi Bethune Hospital. The male to female ratio was 1:14.5 and mean age of onset was 54 ± 13 years (range: 17–71 years). During this period 871 patients with thyroid cancer and without NLDO were all enrolled. The male to female ratio was 1:4.7 and the mean age of onset was 46 ± 11 years (range 16–78 years). Demographic characteristics of the material obtained are shown in Table 1. Baseline data of the patient subgroups.
Patients with and without NLDO symptoms were subdivided into ≤55 years and >55 years old. Groupings were also subdivided by iodine dosage into those receiving ≤5.55 GBq and those receiving >5.5 GBq. Following 131I therapy, whole-body imaging was performed to evaluate the presence of metastatic lesions. 2. Exclusion criteria were as follows: allergy, nasal cavity/sinus problems, or facial trauma. Patients using contact lenses, autoimmune diseases, medications that may cause tear discharge syndrome, and all eye diseases were also excluded from the study. 3. All the patients were diagnosed with NLDO based on lacrimation by an ophthalmologist, according to the following criteria: lacrimal duct irrigation indicating complete obstruction of the lacrimal passage, all flushing fluid flowed back from the upper/lower lacrimal ducts, and the obstruction site was located in the nasolacrimal duct, with or without sticky or purulent secretion. Other secondary factors were excluded. The doctor in charge of lacrimal duct recanalization was not aware of the cumulative dose of radioactive iodine or of the patients’ clinical characteristics. 4. The Institutional Review Board (IRB) approved the experiment.
Methods
1. TGAb values were determined by electrochemiluminescence immunoassay (Roche) with a detection range of 10–4000 Ku/L. The upper limit of TGAb normal range is 115 Ku/L. If the upper limit of the normal range was exceeded, TGAb was positive. 2. After therapy, 131I-whole body scan (WBS) was performed: 1) All patients completed the 131I-WBS and neck-chest Single-Photon Emission Computed Tomography/Computed Tomography (SPECT/CT) fusion imaging on the third day after oral ingestion of 131I (Atomic HighTech Co. Ltd., Guangzhou, China). After the 131I-WBS, a nuclear medicine specialist evaluated the images on the workstation immediately, to decide whether to add other parts of tomographic fusion imaging based on SPECT/CT fusion imaging of the neck and chest. 2) 131I-WBS and SPECT/CT acquisition: The Discovery NM/CT 670 dual probe SPECT/CT instrument (GE, USA) was used. The probe is equipped with a high energy and low-resolution parallel hole collimator. The photopeak was 364 keV, the wiNLDOw width was 20%, the matrix was set at 256 × 1024, and the imaging speed was 5 cm/min. 3) SPECT/CT tomographic fusion imaging: the acquisition parameters were as follows: tube voltage 140 kV, tube current 200 mA, slice thickness 375 mm, and matrices 512 × 512. JET stream workstation (GE Medical Systems) was applied to obtain the SPECT/CT fusion images. (3) Image analysis: radionuclide images (131I-WBS and SPECT/CT) were independently evaluated by two experienced nuclear medicine physicians blinded to the patients’ clinical conditions, with consensus of interpretation, using diagnostic software (Compass viewer H 4.0, Medivoly Technology Co. Ltd., Shanghai, China).
Statistical analysis
Clinical data and imaging features were examined. Normally distributed quantitative data is presented as X ± s with count data being described by constituent ratio. Chi square test was used to analyze count data. Logistic regression model was used to analyze related factors. Variables with statistical significance from univariate analysis were included in multivariate regression analysis. All data were analyzed by Statistical Product and Service Solutions (SPSS) version 23.0 for Windows (SPSS Chicago, IL, USA) software, with a P value <.05 being considered statistically significant.
Results
Thirty-one patients had NLDO and the bilateral to unilateral ratio was 3.4:1. Nineteen patients had metastases, 6 (19.4%) in the lung, 3 (9.7%) in bone, 1 (3.2%) in bone plus kidney, and 9 (29.0%) in the neck and/or mediastinal lymph nodes. No obvious metastasis was found in the remaining 12 cases. One patient (3.2%) received only one round of iodine therapy, 25 patients (80.6%) received two rounds, and 5 (16%) received three or more rounds of therapy. The mean cumulative dose of 131I was 12.06 GBq and the median cumulative dose was 11.1 GBq. Seven cases (22.6%) were TGAb positive and 24 (77.4%) were negative. The earliest onset of NLDO was more than 1 month after the first iodine therapy and the latest was more than 15 months after the second iodine therapy. Before the ophthalmology diagnosis was confirmed, 70% of the patients received at least one form of therapy, including warm compress, eye antibiotics, eye glucocorticoids, artificial tears and ointment, nasal glucocorticoids, or eye drops. Among the 871 cases of thyroid cancer after 131I therapy without NLDO, 3 cases (0.3%) had incomplete tumor resection, 21 (2.4%) had lung metastasis, 9 (1.0%) had bone metastasis, 184 (21.1%) had cervical and/or mediastinal lymph node metastasis, and no definite metastasis was found in the other 554 cases via therapeutic iodine scans. Two hundred and sixty-seven patients (30.7%) received one round of 131I therapy, 578 patients (66.4%) received two rounds, and 26 (2.9%) received three or more rounds of therapy. The average cumulative dose of 131I was 7.77 GBq and the median cumulative dose was 7.4 GBq. One hundred and fifty-seven (18.0%) patients were TGAb positive and 714 (82%) were negative.
Comparative analysis of nasolacrimal duct obstruction after 131I treatment for thyroid cancer under different clinical characteristics.
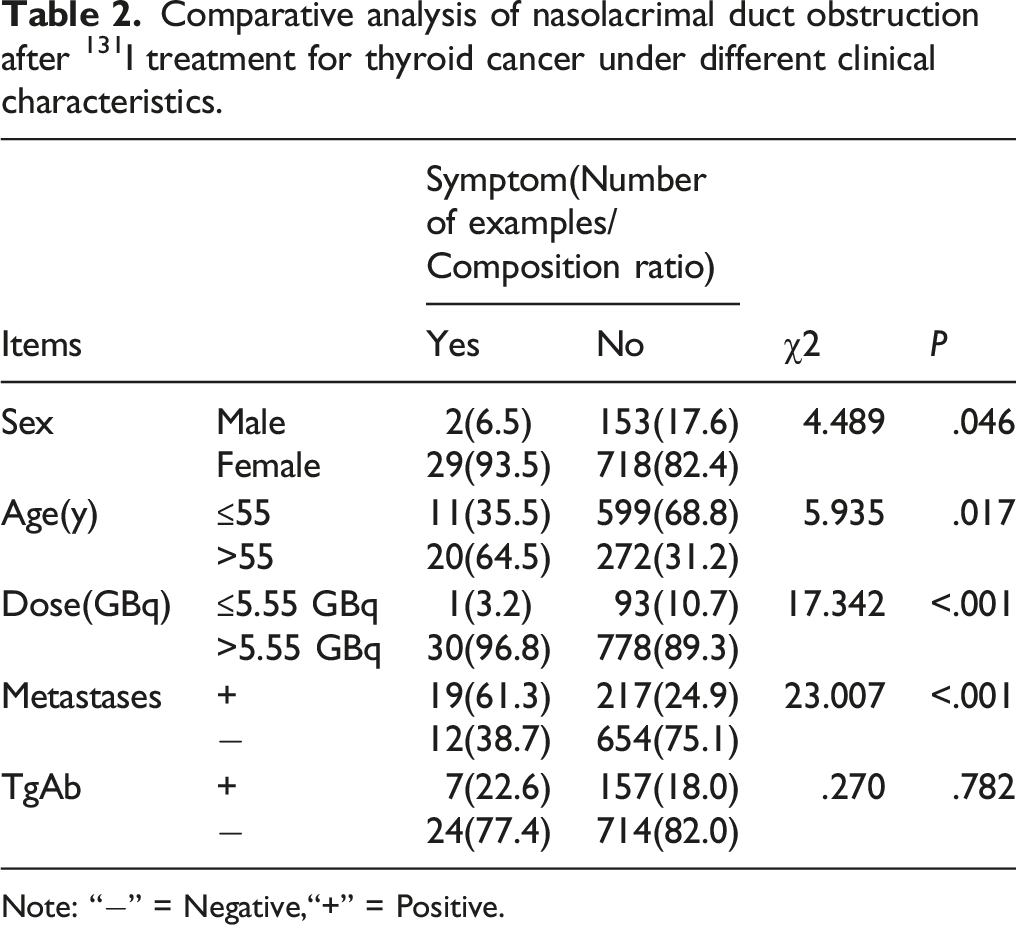
Note: “−” = Negative,“+” = Positive.
Multivariate logisitic regression analysis of nasolacrimal duct obstruction in patients with thyroid cancer after 131I treatment.

Comparative analysis of NLDO and non-NLDO under different clinical characteristics at the same dose of 131I.
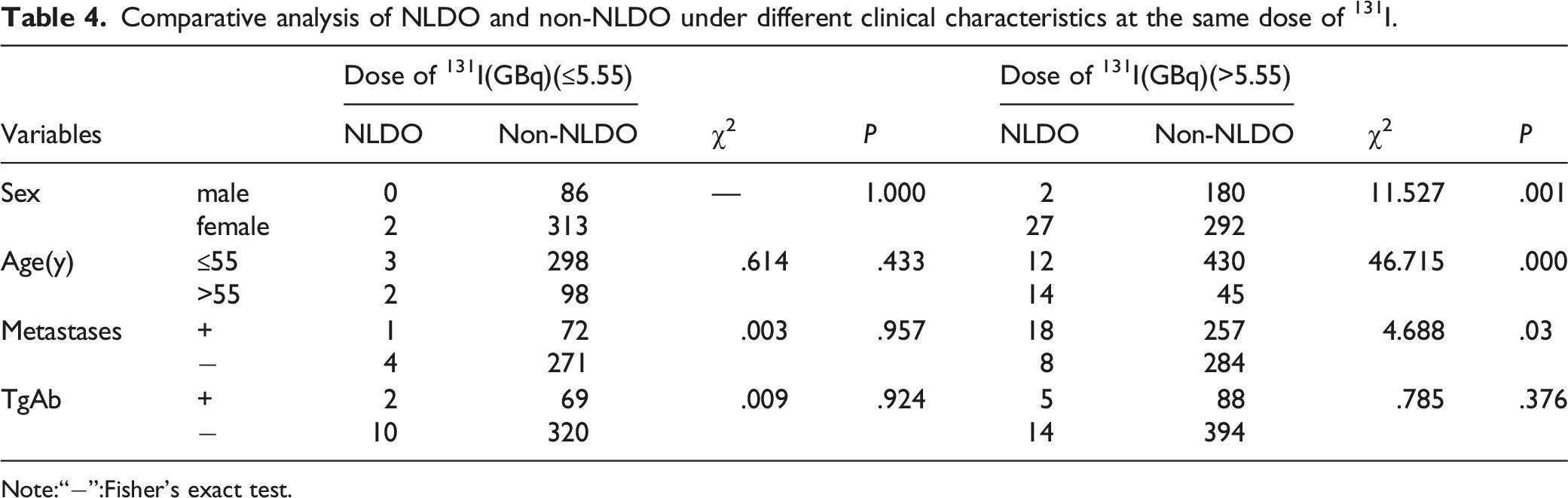
Note:“−”:Fisher’s exact test.
Comparative analysis of nasolacrimal duct obstruction after 131I treatment for thyroid cancer under different number of treatment courses.

Discussion
Radioiodine has been used to treat thyroid diseases for more than 70 years. Besides thyroid tissue itself, sweat and salivary glands and the nasal cavity also have the ability to uptake and store iodine through their sodium iodide transporters. Body fluids such as gastric juice, cerebrospinal fluid, breast milk, and fetal blood can also incorporate 131I leading to an impact of 131I therapy for DTC on gonadal function and reproductive health. As a result, the effects of 131I therapy have attracted a great deal of attention. 5
As early as 1968, Albrecht and Kreutzig6-10 reported salivary gland damage due to high-dose radioactive iodine radiation, leading to dry mouth syndrome and other long-term side effects. Since then, many studies have confirmed this finding and suggested acidic food and parotid gland massage to promote salivary secretion and reduce radiation damage. However, few studies have focused on the side effects of eye discomfort, the most common of which is NLDO. 11 A review 12 shows the incidence of NLDO is range from 2.2% to 18% following 131I therapy, in this study, it was 3.4%. Solans et al. 13 examined 79 patients after 131I therapy (.925–18.5 GBq) and found that 17.7% developed dry eye symptoms in the first year after therapy. There were also patients with epiphora, the most common cause of which was stenosis or obstruction of the lacrimal passage. The cause of epiphora in thyroid cancer patients is considered to be obstruction of the nasolacrimal duct. The lacrimal gland may secrete radioactive iodine, which directly contacts the lacrimal sac and nasolacrimal duct mucosa, resulting in chronic fibrosis of nasal mucosa, thereby causing NLDO. 14 Bakheet et al. 15 considered direct uptake by the nasolacrimal duct system to be more likely than indirect radiation through radioactive tears. They found that radioactive tear secretion began 15 minutes after oral 123I and reached a peak after about 60 minutes. During the first four hours, the total secretion was about 0.01% of the dose. The turnover rate of the lacrimal film system is about 12%–16%/min. Therefore, the main cause of NLDO is direct ingestion, with the effect of radioactive tears being small. Furthermore, hormone and metabolic disorders are also a potential cause of gland dysfunction.
The study of Solans et al showed that the original 10 patients identified with nasolacrimal drainage system obstruction had received a mean cumulative 131I activity of 12.27 ± 2.92 GBq. The mean individual activity was 6.66 ± 0.55 GBq, whereas the mean individual activity administered just before the onset of symptoms was 7.88 GBq. 6 additional patients who were treated with 131I for thyroid carcinoma identified with nasolacrimal drainage system obstruction, The average cumulative dose of 131I preceding symptoms was 19.43 GBq. The average treatment activity was 8.33 GBq, treatment activity immediately preceding symptom onset was 11.95 GBq. All 16 patients received doses significantly greater than 5.55 GBq. Burns et al. 16 have observed at cumulative activities of 5.55 GBq of 131I or higher that patients are at risk for clinically significant nasolacrimal drainage system obstructions; 4.6% of our patients who received radioiodine therapy have documented or suspected obstruction. This is consistent with the conclusion of this study that NLDO is more likely to occur when the cumulative dose of 131I >5.55 GBq. Ali et al. 17 found that no patient receiving 3.7 GBq had symptoms but 4% (2/50) of patients receiving more than 5.55 GBq had symptoms. High dose 131I is therefore associated with NLDO. In the current study, we found that 47.6% (30/63) of patients with and 52.4% (33/63) of patients without NLDO received more than 5.55 GBq. The NLDO incidence was 3.4% (1/29) and 96.6% (28/29). The constituent ratio of NLDO in the group receiving ≤5.55 GBq was significantly less than that in the group receiving >5.55 GBq, which is consistent with previous findings. The review 12 shows they are mostly bilateral and noted in patients who receive more than 150 mCi radioiodine. In this study, there are similar findings, it is 79.3% (23/29) of people have bilateral epiphora in more than 5.55 GBq group. Moreover, patients with Graves’ disease have been reported to have NLDO following 131I therapy.
In the current study, we found a higher proportion of women with NLDO than men. The incidence of thyroid cancer among women is 2 to 3 times higher than that among men. Positive metastatic lesions mean advanced stage, and a high dose of 131I is more likely to cause NLDO.
This study shows that people older than 55 are more likely to have NLDO, which is inconsistent with the view of Ju-Yeun Lee et al. 18 They believe that the reason for under 50 years are in higher risk of large for NLDO is based on the following two aspects: More active inflammatory reactions in the younger age group may have led to more severe obstruction of the nasolacrimal duct in their study Moreover, it is also postulated that the younger age group may feel more discomfort even with milder symptoms compared with the older age group, leading to a higher frequency of surgery. Patients over 55 years were also more likely to have increased family and social responsibilities, leading to greater psychological pressures, which may have rendered them more prone to physical dysfunction. 19 There have been some multivariate analyses that have concluded that the 131I dose was the only cause of obstruction, but these analyses discounted age, gender, and other factors. Thus, it is difficult to exclude the impact of bias in these contrary findings.
Vasily D.Yartsev et al. 20 showed that severe tearing considered to be a probable sign of NLDO occurs patients after single-dose and patients after repeated radioiodine therapy (8.8% vs 23.9%), the conclusion is consistent with this study; in the current study, we found that the prevalence rate of repeat radioiodine therapy (2 times or 3 times and more) is 4.1% and 16.1% vs 0.4%. Vasily D.Yartsev et al. think since from the histopathological point of view, alteration is followed by the induction of reparative processes that do not always result in fibrosis. At the same time, repeated alterations can contribute to the chronicity of inflammatory process and make a greater contribution to the damage to mucous glands of nasolacrimal duct and to fibrosis induction than the strength of administered dose.
In many cases, DTC has an indolent course and a generally favorable prognosis. However, recurrences may occur in up to 20% of DTC patients, with 10% of them having a fatal outcome (i.e., overall mortality of 65% at 5 years and 75% at 10 years). 21 The quality of life of some patients of this type will be seriously affected so that they will not give priority to the occurrence of NLDO symptoms. Therefore as a major issue, quite a few patients were that of metastasis whose life expectancy and other morbidities would defer NLDO. In the non-NLDO group, one case placed an endotracheal tube who had incomplete tumor resection, 2 patients with bone metastasis have severe bone pain symptoms. Whether these obvious discomfort symptoms will cover up the occurrence of NLDO is a question worthy of consideration, which is also the deficiency of this experiment. It needs to carry out more detailed follow-up for this group of people.
Conclusion
131I therapy may increase the incidence of nasolacrimal drainage system obstruction, especially repeat radioiodine therapy. For female patients over 55 years with metastases, when receiving a dose >5.55 GBq, doctors should be aware of this potential rare complication and multiple factors should be considered when determining appropriate dosages. To reduce the incidence of NLDO, it is suggested that high risk populations are referred for appropriate ophthalmic surgical consultation, for timely diagnosis and therapy.
Footnotes
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted with approval from the Ethics Committee of Shanxi Bethune Hospital (No: YXLL-2022-027). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Data availability
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.