
Abstract

Significance statement
Obstructive laryngeal neoplasms represent a potential emergency, requiring urgent evaluation and possible intervention to avert airway compromise. While the most common laryngeal lesions include papilloma and malignant squamous cell carcinoma, other neoplasms may also present as a supraglottic or glottic mass. Primary laryngeal lymphomas represent less than 1% of all laryngeal tumors. 1 This case describes the evaluation and management of a rare, recurrent Mantle Cell Lymphoma of the supraglottis.
Main text
A 71-year-old Hispanic male, former smoker, with a history of diabetes mellitus presented to laryngology clinic with several months of progressive dysphagia, dysphonia, and dry cough. For several months he had experienced recurrent bouts of choking on his saliva while sleeping. Three years prior, he had been diagnosed with diffuse Stage IV Mantle Cell Lymphoma (MCL) (Ki67 20%) and received treatment with six cycles of Bendamustine and Rituximab. His previous cancer did not occur in the larynx. Surveillance PET/CT three months after completing treatment showed a complete response to therapy. (Figure 1C). A) Preoperative fiberoptic laryngoscopy revealing 2 cm left supraglottic lesion. B) Postoperative visit after CO2 laser resection. Fibrinous exudate and more patent airway appreciated. C) PET-CT 18 months prior to presentation, after previous treatment. D) PET-CT at time of presentation with supraglottic hypermetabolic mass.
In-office flexible laryngoscopy was performed, which revealed a 2 cm, submucosal, non-ulcerated mass effacing the left aryepiglottic fold and false vocal fold. (Figure 1A). A flexible endoscopic evaluation of swallow (FEES) was performed, which revealed trace residue in the vallecula and pyriform sinuses (Yale Pharyngeal Residue Severity = 2 and 2, respectively), without penetration of residue into the airway (Penetration-Aspiration Scale = 1). A PET/CT revealed a hypermetabolic supraglottic mass, suspicious for laryngeal recurrence of lymphoma. (Figure 1D).
Given the patient’s bothersome and progressive symptoms, operative intervention was offered, consisting of biopsy and mass debulking with CO2 laser. Intraoperatively, a carbon dioxide (CO2) laser was used to resect the portions of the mass overlying the glottic inlet until the true vocal cords could be seen. Specimen was sent for pathology and the procedure was concluded. There were no complications. The patient was monitored overnight after surgery and discharged the following morning.
Postoperatively, the patient’s voice demonstrated improved clarity and range. He reported improvement in dysphagia and resolution of choking episodes. Post operative endoscopy revealed a defect along the left false vocal cord and supraglottis with fibrinous exudate. (Figure 1B). Repeat FEES revealed mild residue in the vallecula and trace residue in the pyriform sinuses (Yale Pharyngeal Residue Severity = 3 and 2, respectively), without penetration of residue into the airway (Penetration-Aspiration Scale = 1).
Final operative pathology with flow cytometric analysis showed 62–66% CD5(+)/CD10(−) kappa-restricted monotypic B-cell population, consistent with recurrent MCL. (Figures 2A-2D). The patient was referred to his oncologist for additional systemic therapy. Composite photomicrographs of supraglottic mass. A) The mass is composed of diffuse infiltrate of monotonous small to medium sized atypical lymphoid cells (H& E, 400× magnification). Reactive epithelium is only present focally (inset. H&E, 200×); B–D. The atypical lymphoid cells are diffusely positive for CD20 (B, 400×) and CD5(C, 400×) in comparison to CD3(Inset, 400×) and BCL1 (D, 400×).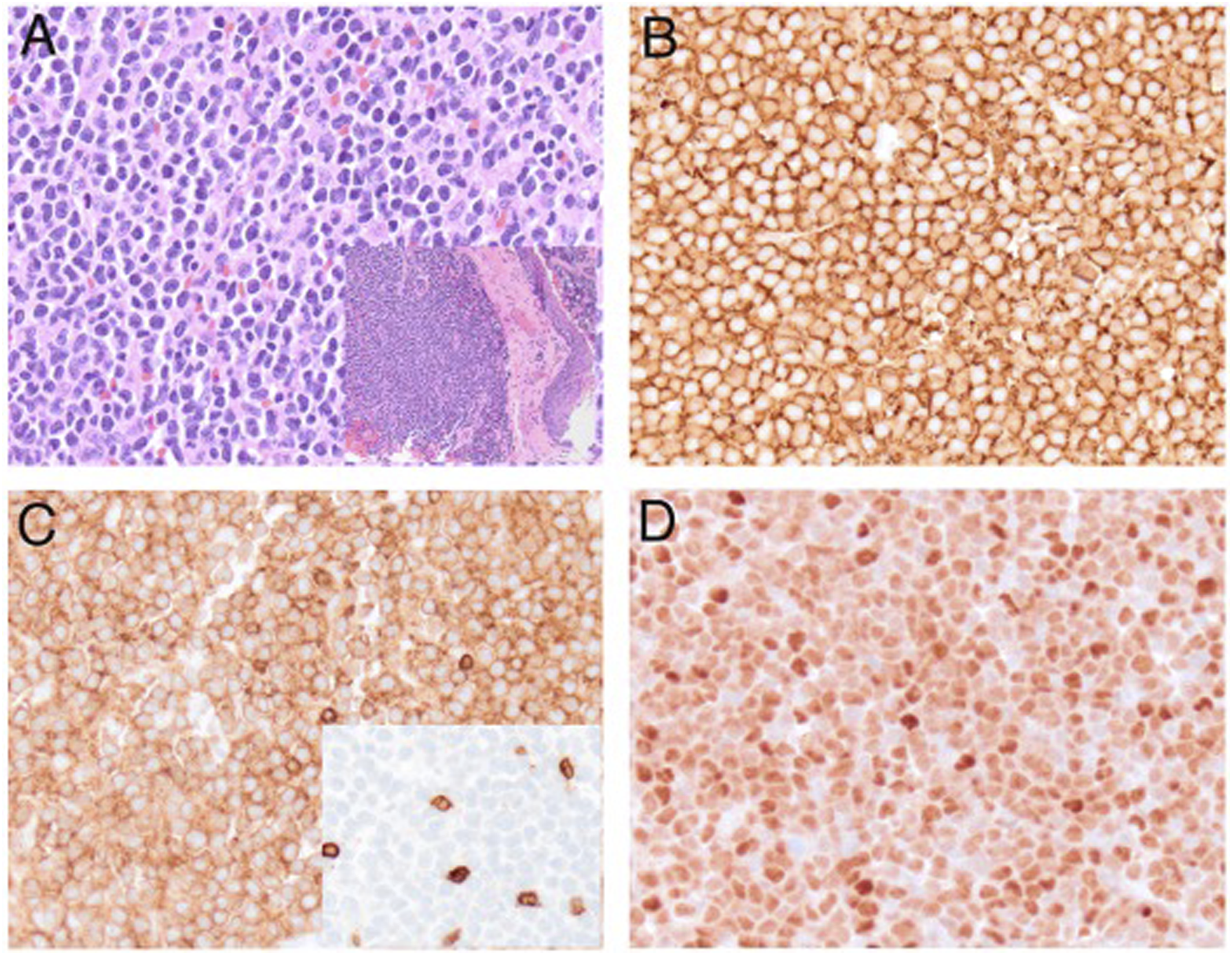
Laryngeal lymphomas are rare, representing about 1% of all laryngeal tumors. 1 Typical symptoms of laryngeal lymphoma include progressive dysphonia and dysphagia, with or without B-symptoms, such as fevers, chills, weight loss, and fatigue. Laryngoscopy may show a smooth or polypoid, non-ulcerated tumor located in the supraglottic structures, such as epiglottis or aryepiglottic folds. This location preference is thought to be related to a greater concentration of follicular lymphatic tissue compared to the glottis or subglottis. 2 On presentation, an estimated 25% of patients will have regional lymph node involvement. 1 Imaging with CT or MRI shows a contrast-enhancing homogenous tumor, while FDG-PET imaging demonstrates high metabolic uptake. 3
Mantle cell lymphoma (MCL) is a rare subtype of B-cell non-Hodgkin lymphoma, characterized by an overexpression of cyclin D1. With an estimated incidence of 1 per 200,000 persons, MCL is more common in males and in the 7th decade of life.4-6 There has only been one reported case of systemic MCL recurring in the larynx. 7 A recent review by Breen et al. identified 10 patients with primary or secondary laryngeal MCL. Within this cohort, 2-year and 5-year overall survival of Mantle cell lymphoma of the Head and Neck, including the larynx, was 83% [78–87%] and 63% [57–69%], respectively. 5 For extranodal MCL in the Head and Neck (all subsites), age and Ann Arbor Staging (III and IV) were significant predictors of overall survival.
Standard treatment of laryngeal lymphoma includes systemic chemotherapeutic agents and immunotherapy, primarily rituximab and bendamustaine. Response to chemotherapy is often robust and surgical excision is typically not needed. As in the above reported case, conservative biopsy with limited surgical resection may be employed to relieve acute airway obstruction with good results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.