
Abstract
Objective
We aimed to determine the prognostic value of lymphovascular invasion (LVI) in pyriform sinus carcinoma (PSC) after primary surgery with adjuvant radiotherapy (RT) or concurrent chemoradiotherapy (CCRT).
Methods
Patients who underwent primary surgery at our institution between 2000 and 2018 were included in this study and retrospectively analyzed. The endpoints were locoregional recurrence (LRR), distant metastasis (DM), and disease-specific survival (DSS).
Results
We reviewed 117 patients with PSC. LVI was identified in 29 patients (24.8%). The 5-year LRR rate, DM rate, and DSS rate were 29.4%, 31.7%, and 45.9%, respectively. Tumors with LVI were associated with a significantly higher LRR (P = 0.002, HR 3.678, 95% CI 1.646-8.218) and DM (P = 0.003, HR 3.666, 95% CI 1.543-8.709) and a lower DSS (P = 0.001, HR 2.814, 95% CI 1.519–5.213) in multivariate analysis.
Conclusion
LVI is a significant predictor of poor prognosis in patients with PSC treated with surgery plus adjuvant RT/CCRT.
Introduction
Hypopharyngeal cancer is a subgroup of head and neck cancer with a relatively rare rate and poor prognosis.1,2 Recent evidence confirms that treatment with upfront surgery and adjuvant radiotherapy (RT) or concurrent chemoradiotherapy (CCRT) was associated with longer survival compared to those treated with primary RT/CCRT in patients with advanced hypopharyngeal cancer, which indicates that surgery remains the primary option for hypopharyngeal cancer.3–6 The 5-year survival rate of hypopharyngeal cancer after combined surgery with adjuvant RT/CCRT is reported to be 35%–66%.4,5,7 In 1987, Close et al. 8 reported that lymphatic invasion and/or vascular invasion correlated with local recurrence, neck recurrence, and distant metastasis (DM) in oral and oropharyngeal carcinoma. Since then, lymphovascular invasion (LVI) has been widely studied in head and neck cancers, especially in oral cancer, and has been found to be a predictor of lymph node metastasis (LNM) and prognosis.9,10 LVI is defined as the presence of tumor cells within definite endothelial-lined spaces, either lymphatic or blood vessels, detected by hematoxylin and eosin (H&E) staining or immunohistochemistry. 11 A few recent studies have analyzed the relationship between LVI and the prognoses of hypopharyngeal cancer. LVI was confirmed to be a negative predictor for poor disease-free survival and disease-specific survival (DSS) rate.12,13 Tumors originating from the pyriform sinus are the most frequent hypopharyngeal cancer.5,14 In our previous study, LVI was one of the predictors for recurrence free survival and disease-specific survival rate in patients with pyriform sinus carcinoma (PSC). 15 However, the relationship between LVI and tumor recurrence is still uncertain,16,17 and the influence of LVI on the recurrence of PSC needs further study.
We retrospectively reviewed a series of patients with PSC to further reveal the influence of LVI on tumor recurrence and prognosis.
Patients and Methods
Study Design and Patient Selection
This was a retrospective review of patients with PSC in our institute between 2001 and 2018. The inclusion criteria included a) primary tumor originating from the pyriform sinus, b. histopathological type of squamous cell carcinoma (SCC), and c. initial treatment with surgery and adjuvant RT or CCRT. The exclusion criteria included a. tumors invading the carotid sheath or prevertebral tissue (cT4b); b. distant lymph node or organ metastasis (M1); and c. incomplete clinicopathological data. Finally, a total of 117 patients were eligible for this retrospective study.
Treatment
The treatment plan and process for each patient were jointly determined by the surgeon and patient and were supervised by a multidisciplinary team. All patients initially underwent surgery. Forty-nine patients underwent laryngeal function-sparing surgery, and the other 68 patients underwent nonlaryngeal function-sparing surgery. A pectoralis major myocutaneous flap or submental island flap was used to repair noncircumferential defects. Free jejunum flaps were mostly used for peripheral pharyngeal defects, and pharyngogastric anastomosis was performed after total esophagectomy. Therapeutic neck dissection included levels Ⅱ to Ⅴ and elective neck dissection mostly included levels Ⅱ to Ⅳ. Ipsilateral central neck dissection was performed in 29 patients. Hemithyroidectomy was performed in 54 patients. All surgical specimens were paraffin embedded, sectioned, and HE stained. Postoperative RT or CCRT was performed within 4 to 8 weeks. The average total dosage of RT was 62.8 Gy (56–70). Cisplatin (100 mg/m2 every 3 weeks or 50 mg/m2 every week) was the commonly used concurrent chemotherapy.
Data Collection and Follow-Up
The pathological staging criteria were based on the AJCC 8th Edition TNM staging system. 18 The demographic features and pathological data were collected. The resected specimens of the primary tumor and dissected lymph nodes (LNs) were fixed with 10% buffered formalin and stained with hematoxylin-eosin. Then, the whole of the tumor specimen was histopathologically examined. Pathological data included: pT stage, pN stage, number of positive LNs, extranodal extension (ENE), pathological differentiation, surgical margin, LVI, perineural invasion (PNI), thyroid gland invasion (TGI), and adjuvant therapy. In detail, if the tumor cells infiltrate within endothelial-lined spaces, either lymphatic or blood vessels, detected by H&E staining or immunohistochemistry, LVI was diagnosed. 11 The pathological findings were reviewed by an experienced pathologist.
The patients were followed-up every 3 months during the first year, every 6 months from the second year and every year after 5 years. Every follow-up examination included fiber or electronic laryngoscopy, enhanced MRI or CT of the neck, ultrasonography, and chest X-ray or CT scan. If tumor recurrence of the mucosa was suspected, biopsy and pathological examination were performed. If tumor recurrence of the neck was suspected, biopsy or FNA (after 2012) was performed. The median follow-up time was 24 months (range, 6–196).
Statistical Analysis
SPSS v27.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Categorical variables were expressed as frequencies and proportions, which were compared by chi-square or Fisher’s exact test. Continuous variables were expressed as the mean ± SD and compared by t test. The endpoints of the current study were locoregional recurrence (LRR), DM, and DSS. Survival data were analyzed by means of the Kaplan–Meier method, and survival curves were compared using the log-rank test in univariate analysis. Cox regression analysis was used for multivariate analysis. All statistical tests were 2-sided, and P values less than 0.05 were defined as statistically significant.
Results
Clinicopathological Characteristics
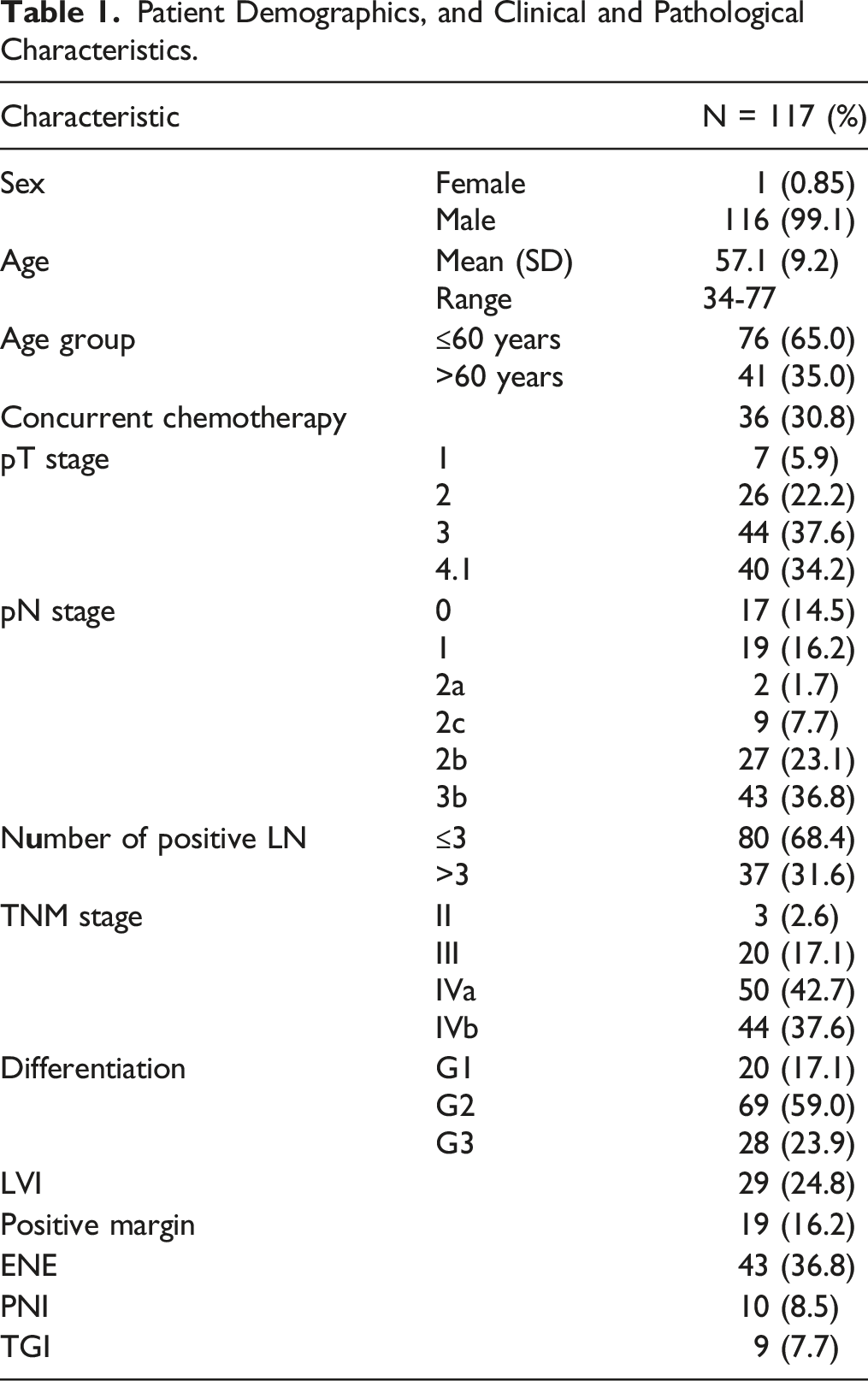
Patient Demographics, and Clinical and Pathological Characteristics.
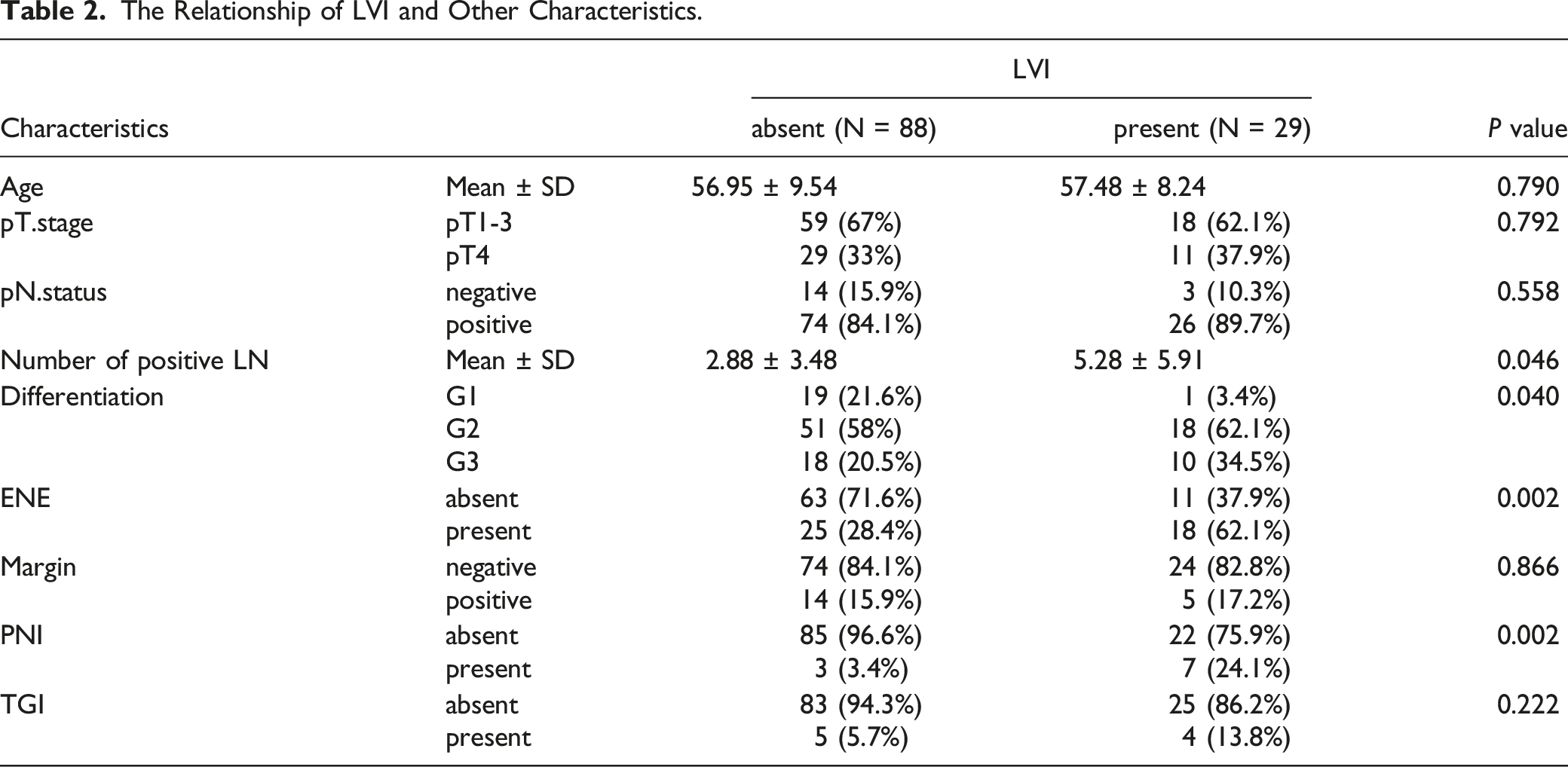
The Relationship of LVI and Other Characteristics.
Recurrence and Survival
At the end of follow-up, 44 patients experienced tumor recurrence, of whom 22 had LRR, 19 had distant metastases, and 3 had LRR with distant metastases. Forty-three patients died of tumor recurrence, and 8 patients died of other causes.
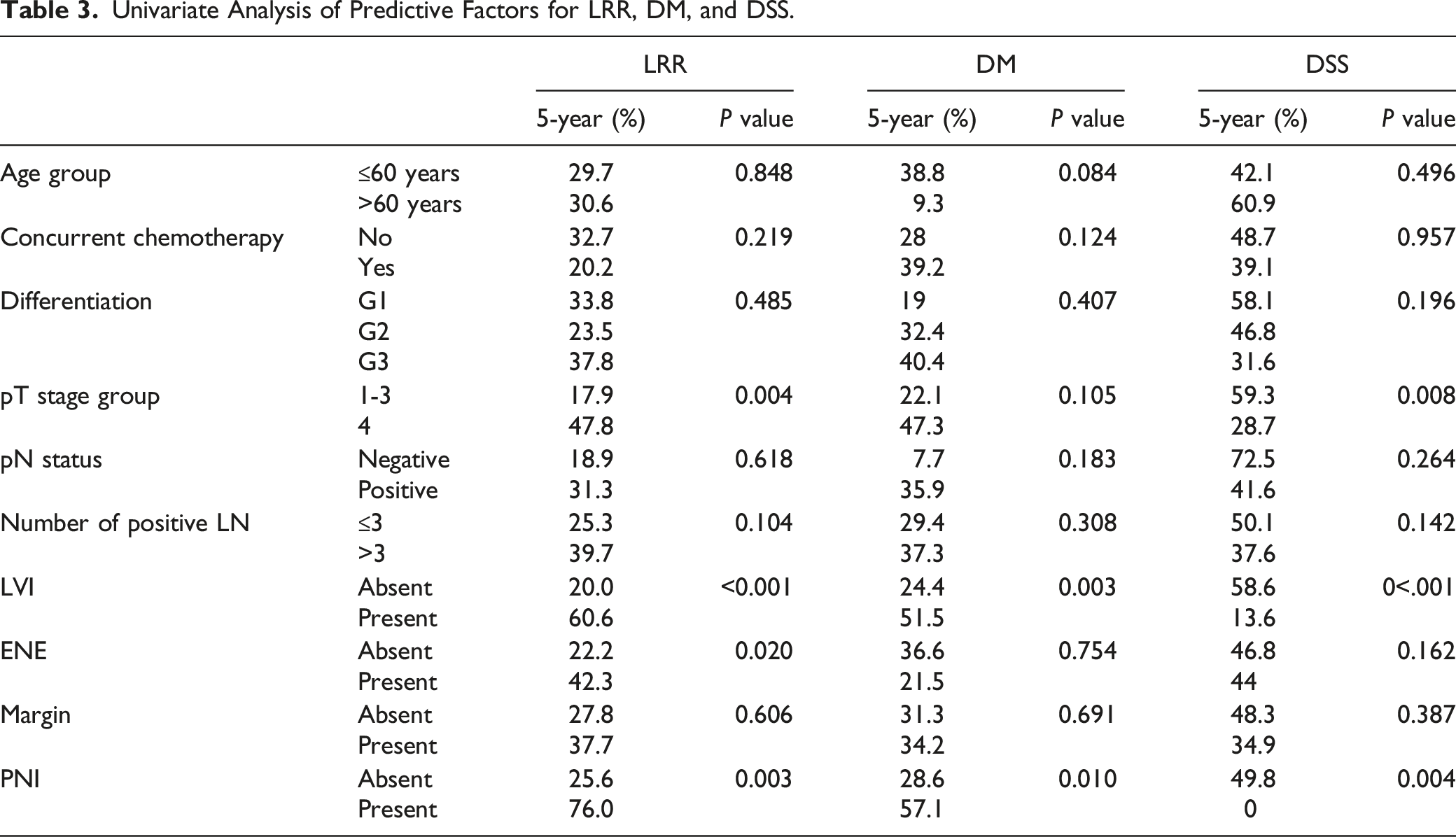
The 5-year LRR rate was 29.4%. Univariate analysis showed that pT stage, LVI, ENE, and PNI were significantly associated with a higher LRR rate. Multivariate analysis showed that pT stage (P = 0.004, HR 3.053, 95% CI 1.370–6.803) and LVI (P = 0.002, HR 3.678, 95% CI 1.646–8.218) (Figure 1A) were independent predictive factors for LRR. The 5-year DM rate was 31.7%. Univariate analysis showed that LVI and PNI were significantly associated with a higher DM rate. Multivariate analysis showed that only LVI (P = 0.003, HR 3.666, 95% CI 1.543–8.709) was an independent predictive factor for DM (Figure 1B). The 5-year DSS rate was 45.9%. Univariate analysis showed that pT stage, LVI and PNI were significantly associated with a poor DSS rate. Multivariate analysis showed that pT stage (P = 0.009, HR 2.243, 95% CI 1.227–4.098) and LVI (P = 0.001, HR 2.814, 95% CI 1.519–5.213) (Figure 1C) were independent predictive factors for DSS. Univariate and multivariate analyses of predictive factors for LRR, DM, and DSS are summarized in Table 3 and Table 4. Kaplan‒Meier curve of cumulative LRR rate (a), cumulative DM rate (b), and DSS rate (c) according to LVI status. Univariate Analysis of Predictive Factors for LRR, DM, and DSS. Multivariate Analysis of Predictive Factors for LRR, DM, and DSS.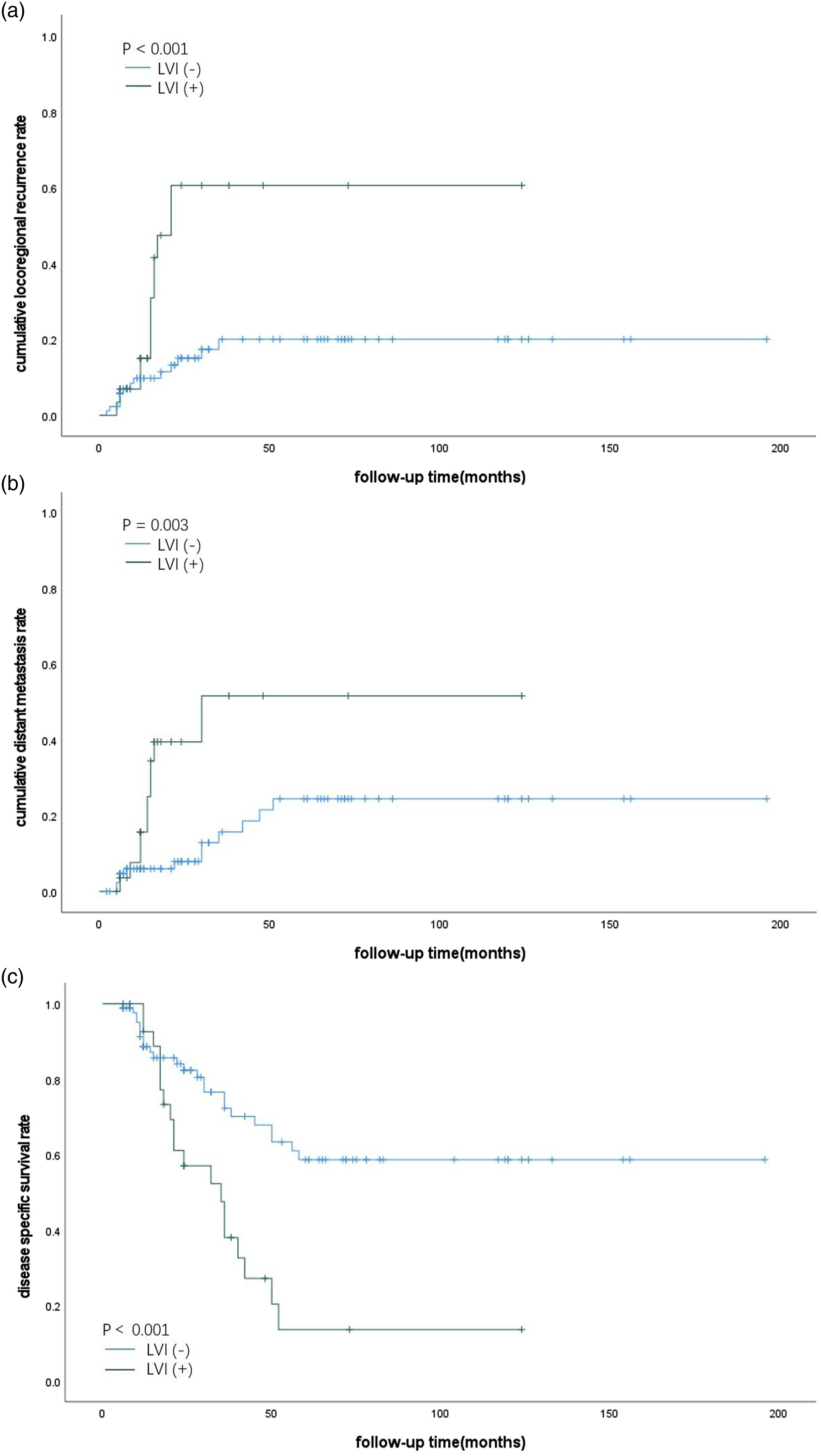

Of the 29 patients with LVI, 10 patients received adjuvant CCRT, and 19 received adjuvant RT. The 5-year LRR rate, 5-year DM rate, and 5-year DSS rate were 55.6% vs 62.4% (P = 0.429), 55% vs 52.3% (P = 0.351), and 14.8% vs 13.0% (P = 0.544), respectively. There was no difference between the 2 groups in terms of LRR rate, DM rate, and DSS rate.
Discussion
In this study, we demonstrated that LVI is a strong predictor for a higher LRR rate, DM rate, and a lower DSS rate in PSC patients who were treated with upfront surgery with adjuvant RT or CCRT.
Recurrence is common in hypopharyngeal cancer, and nearly half of patients experience recurrence within the first year after initial treatment,16,17 which is an important reason for the poor prognosis of hypopharyngeal carcinoma. Traditionally, widely recognized prognostic factors of hypopharyngeal carcinoma include pathological differentiation, T stage, N stage, ENE, number of metastatic LNs, surgical margin, and treatment modality. Primary surgery with postoperative RT/CCRT is currently considered to obtain a better prognosis than nonsurgical modalities.3–6 In the present study, all patients received surgery with postoperative RT or CCRT. The 5-year DSS was 45.9%, and multivariate analysis showed that pT4 stage and LVI were independent predictive factors for poor DSS. The 5-year DSS of patients with LVI + tumors were significantly lower than that of patients with LVI- tumors (13.6% and 58.6%, respectively). In a retrospective study, the 5-year OS rate and DSS rate of LVI + patients were 28.8 and 54.2%, respectively, which were lower than those of LVI- patients (66.7% and 76.6%, respectively), and the local recurrence rate and regional recurrence rate were 59.3% and 40.7% in the LVI + group, which were higher than 27.9% and 22.5% in the LVI − group (P < 0.000, P = 0.014). 12 Another study by Saito Y et al. 13 also confirmed that vascular invasion was a significant prognostic factor for overall survival, and this study included patients treated with both upfront and salvage surgery. However, studies focusing on the influence of LVI on the recurrence of PSC after surgery are still rare. In oral cancer, LVI is an independent negative prognostic factor associated with cervical LNM and locoregional recurrence 10 and DM 1. 19 In hypopharyngeal cancers, a study by Gang G et al. 12 did not reveal a significant association between LVI and DM, and the DM rates of patients with LVI + hypopharyngeal cancers and LVI− hypopharyngeal cancers were 18.6% and 12.6%, respectively, with no difference (P = 0.160). In our study, LRR and the DM rate were significantly higher in LVI + patients than in LVI- patients. LVI was an independent predictor for both LRR and DM.
LVI was correlated with poor differentiation, a greater number of metastatic LNs, ENE and PNI in the present study. Gang et al. revealed that the T stage, N stage, and histological tumor grade are independent risk factors for LVI of hypopharyngeal cancer. 12 The poor prognosis of patients with LVI + tumors may also be influenced by multifocal prognostic factors, such as poor tumor differentiation, LNM, and ENE. PNI was reported to be a prognostic factor for poor survival and local recurrence in patients with head and neck cancer.20,21 In our study, PNI was associated with a higher LRR rate and DM rate and lower DSS in univariate analysis; however, multivariate analysis did not reveal a statistically significant difference.
It is traditionally believed that adverse prognostic factors such as poor tumor differentiation, LNM, ENE, and positive surgical margins can be effectively controlled by adjuvant RT/CCRT. 22 For advanced-stage hypopharyngeal cancer patients (especially T3-4a and N2b-c), primary surgery followed by adjuvant (chemo-)radiotherapy provides better local and regional control but has little influence on the DM rate. 23 In our analysis, compared with RT, CCRT did not improve locoregional control or DSS. In the subgroup of patients with LVI + tumors, no difference was found between patients with adjuvant RT and those with CCRT in terms of LRR, DM, and DSS. In this situation, LVI may become a predictor of refractory tumors and lead to poor prognosis.
Given that this was a retrospective study with a small sample size, selection bias inevitably existed. This respective study only enrolled PSC patients who received surgery with adjuvant RT/CCRT, which minimized the impact of other confounding factors, such as treatment modalities, and the conclusion may be limited. In our previous study focusing on the relationship between LNR and survival, LVI was also found to be negatively associated with survival rate. 15 In the present study, we further analyzed the relationship between LVI and LRR and DM in PSC patients. We concluded that LVI is a strong predictor for tumor recurrence and decreased DSS, and early intervention and more effective treatment regimens are needed. Large samples and high-quality studies are needed to obtain a more reliable conclusion in the future.
Footnotes
Author Contributions
Hui Huang and Wensheng Liu contributed to conception and design of the study. Hui Huang organized the database and performed the statistical analysis. Hui Huang wrote sections of the manuscript. Hui Huang and Siyuan Xu prepared tables and figures. Jie Liu, Xiaolei Wang, and Shaoyan Liu contributed to manuscript revision. All authors read and approved the submitted version.
Declaration of Conflicting Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the institutional ethics committee.
Data Availability
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.