
Abstract
We present a case of malignant melanoma in the middle ear in a 63-year-old woman who presented with severe pain on the right side of her face and head, tinnitus, photophobia, and hemorrhagic discharge from the right ear, as well as right facial nerve paralysis. After more than two years of conservative treatment for otitis media and sclerotic mastoiditis, a pathologically enlarged lymph node on the right side of the neck appears. It is removed, and the histopathological examination reveals that it is metastatic malignant melanoma. Imaging examinations reveal a tumoral lesion in the middle ear with bone infiltration. The right middle ear is operated on, and the tissue sent for testing reveals melanoma. The patient was treated with Nivolumab after the operation and is now in sustainably good condition.
Keywords
Introduction
The action of various tumorigenic factors significantly disrupts cell growth regulation. Tumors develop gradually as a result of these circumstances. Tumors are abnormal masses of tissue formed when cells divide too quickly or do not die when they should. Tumors can be as small as a nodule or as large as a mass, and they can appear almost anywhere in the body, depending on the type. Tumors can be classified as benign, premalignant, or malignant.1 –3 Malignant melanoma arises from melanocytes. Melanocytes typically reside in the epidermis and occasionally the dermis, although they can also be found in the head and neck mucosa. 4 Malignant melanoma is a type of cancer that usually affects the skin and accounts for approximately 65% of all skin cancer deaths. The incidence increases with age and disproportionately affects white people. One of the main causes of this melanoma is assumed to be exposure to the sun’s UV rays. 5 Malignant melanoma can also develop in the mucosa, that is, mucosal melanoma; however, this only occurs in 1.3% of all cases of the disease. In contrast, the head and neck region accounts for about 55% of all mucosal melanomas. 6 The mucous membrane of the nose and paranasal sinuses are the most commonly affected regions, followed by the mucous membrane of the oral cavity. 7 To our knowledge, there have only been a handful of cases of melanoma that have been localized to the middle ear. It is often diagnosed in its advanced stages due to the hidden location and symptomatology associated with this region.
Case Report
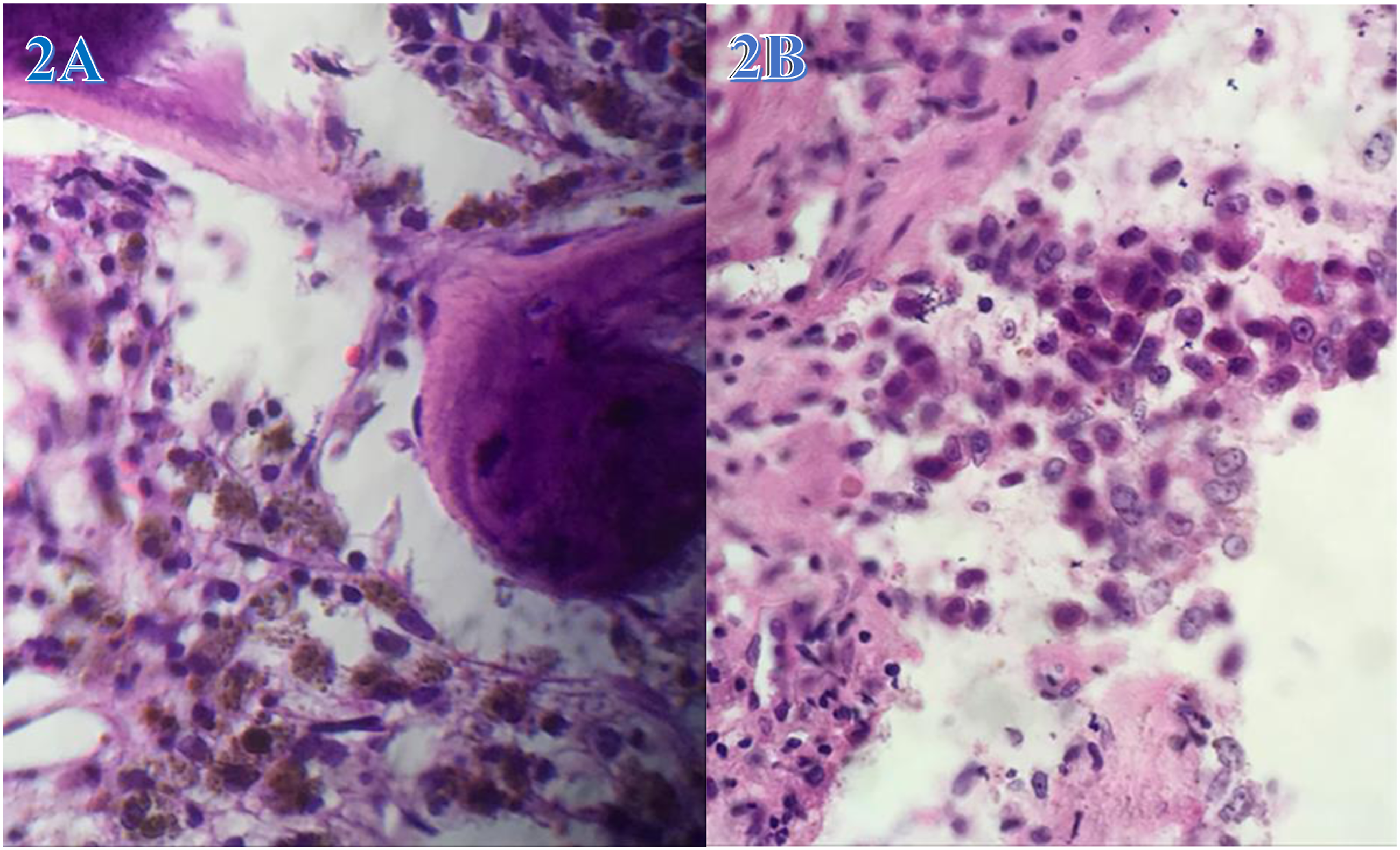
The 63-year-old patient arrived at the clinics with a severe headache, right-sided facial pain, photophobia, and right ear ringing. Clinical examination revealed redness and swelling of the right ear’s external canal, and computer tomography (CT) revealed chronic right mastoiditis (Figures 1A). The patient had conservative care for several days, including corticosteroids and antibiotics. Three months later, she returned with the same signs and symptoms, but this time she also had right facial nerve paresis, hearing loss, and sporadic right ear discharge. A second CT of the temporal bones reveals mastoiditis with sclerotic alterations on the same side and otitis media of the right middle ear. On an otoscopic examination, a swollen tympanic membrane is described as bleeding in the lower posterior quadrant and black in appearance. The patient was advised to undergo surgery, but because this type of operation cannot be carried out locally, she is urged to travel abroad for treatment, which she has chosen not to do. After six months, the patient is examined at a different clinic for the same concerns, and a CT cerebral angiography is done (Figures 1B). Once more, it was determined to treat the symptoms of otitis and mastoiditis; however, this time, it was suspected for glomus tympanicus and glomus jugularis with partial bone destruction. A few months later, the patient experienced a painless lymph node at level IIB on the right side of the neck, with dimensions of 30 × 18 mm. These were also confirmed by CT scans (Figures 1C). After two weeks of antibiotic therapy, ultrasound did not reveal lymph node shrinkage. The right tympanic membrane is seen by otoscopy to be retracted, black, and devoid of reflexes. After the brown to black lymph node was excised, histopathology discovered melanoma malignum metastaticum in the lymphonodorum. The head and neck are also subjected to a magnetic resonance scan, which identifies a solid mass in the petrous bone with a diameter of 25 × 20 mm (Figures 1D). While the other findings were within physiological limits, the positron emission tomography-computed tomography (PET-CT) showed higher metabolic activity in the right middle ear region (SUVmax 3.98) (Figures 1E). Six months later, the patient has a surgical intervention: a right retroauricular craniotomy with extirpation-assisted cum neuronavigatorem. The histopathological findings confirm the presence of malignant melanoma that had infiltrated a portion of the petrous bone (Figures 2A and 2B). One month after surgery, the patient begins immunotherapy (Nivolumab) treatment for 6 cycles, which she tolerates well. On the last posttherapy assessment, a CT of the head, neck, and thorax revealed no pathological findings (not presented). The patient’s clinical state is good right now, but she complains of persistent ringing in her right ear and sporadic dizziness. The patient will be followed up regularly in accordance with the malignant melanoma protocol. The chronic right mastoiditis revealed by computer tomography. A: The mastoid cells on the right in this CT image of the head have irregular ventilation, reduced size, and pathological content, indicating chronic mastoiditis. B: CT angiography of the carotid artery and jugular veins shows the widest right jugular vein up to the jugular bulb. In this case, we are dealing with jugular glomus with surrounding bone destruction. C: A pathologically enlarged lymph node with dimensions of 3–4 cm can be seen on the right side of the neck in this CT view. D: In this magnetic resonance image, a solid mass with a diameter of 25 × 20 mm is seen in the petrous bone, with the sigmoid sinus displaced medially. E: A tumor mass in the middle ear is shown in PET-CT. Histopathology of the malignant melanoma. A: Cells with pigment in their cytoplasm infiltrate the bone marrow. B: Malignant epithelioid cell sheets with moderate nuclear pleomorphism and prominent nucleoli.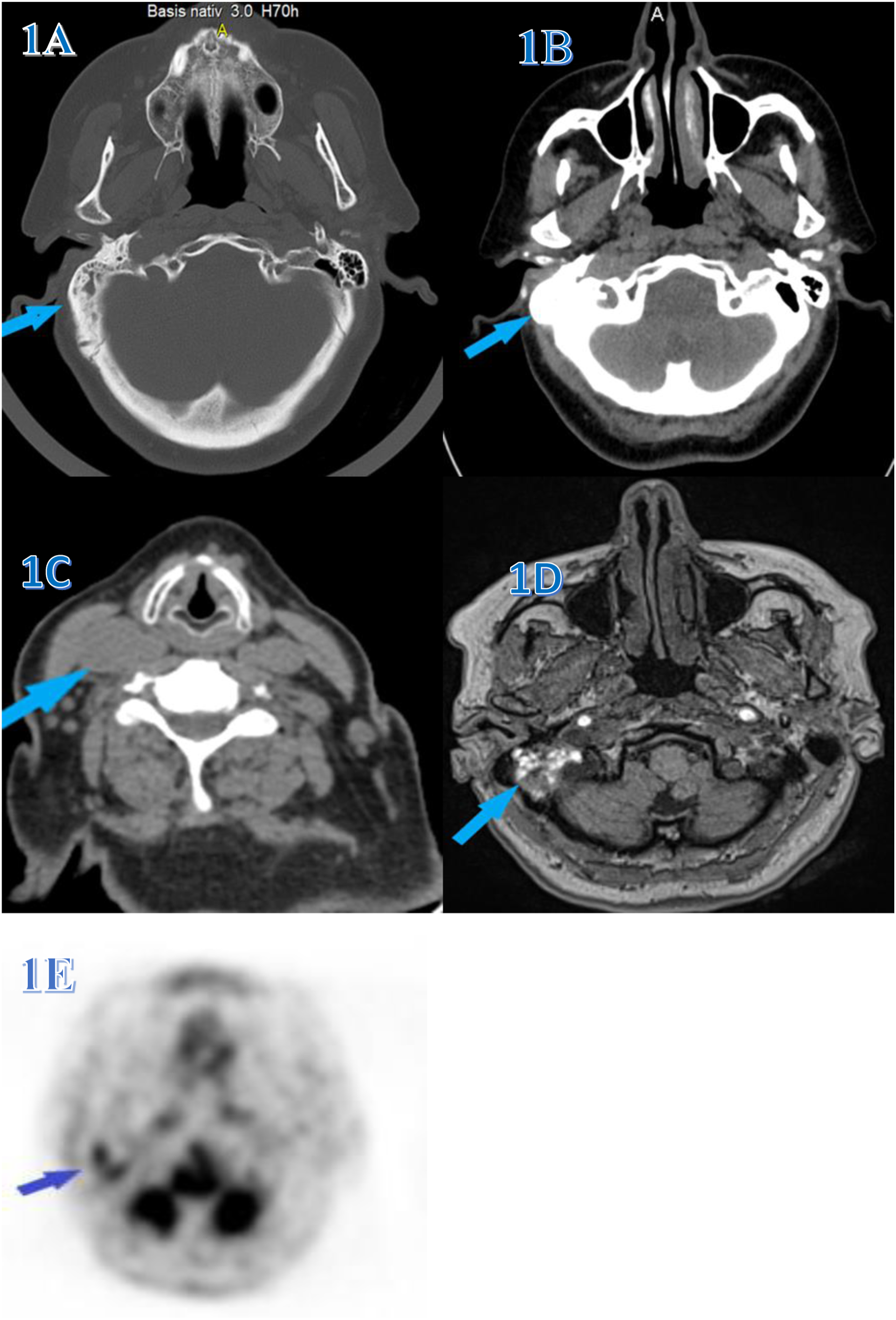
Discussion
People between the ages of 60 and 80 are frequently affected by mucosal melanoma of the head and neck, with a small male predominance. 6 Otorrhea (50%) hearing fullness (40%) and hearing loss (30%) are the 3 most common symptoms of patients with primary middle ear melanoma. 8 Surgical resection is crucial in the management of malignant melanomas, although it is not always feasible due to the location of the tumor. In certain reports, postoperative radiotherapy has been described as effective in enhancing local control in mucosal melanoma, although this has not yet been demonstrated. 9 Less than 10% of mucosal melanomas have been shown to harbor mutations in the proto-oncogenes BRAF and NRAS. In a recent study, Nivolumab and Ipilimumab were given to 30 Japanese patients with mucosal melanoma, and the overall response rate was only around 43%. 10 When melanoma develops in unexpected places, like the middle ear, it is more challenging to diagnose, which frequently leads to a delayed diagnosis and advanced stages of the disease. Middle ear primary malignant melanoma can spread to the lungs, liver, intraparotid, abdomen, and skin metastases. 11 Because of this, in the cases published thus far, the survival rate in patients with melanoma of the middle ear has been poor; only half of the cases have exceeded the eight-month survival rate. 12 In our case, the delay in diagnosis was caused in part by treating the patient for symptoms of otitis media and mastoiditis with sclerotic changes, as well as the country’s inability to perform surgical intervention. These were the primary reasons for making the diagnosis after more than 2 years of symptomatic treatment. Melanoma was discovered only after it had spread to the lymph nodes in the neck. In our case, CT and magnetic resonance provided more accurate results than PET-CT. In other reports, CT and magnetic resonance imaging have been described as the main imaging methods for diagnosing melanoma of the middle ear, especially when the disease infiltrates bone. 13 The importance of a clinical examination with an otoscope should not be underestimated. Several times during the clinical examination, the tympanic membrane was reported as swollen, bloody, and dark-looking, but these changes were attributed to otitis media, mastoiditis, and a glomus tumor of the middle ear.
In conclusion, we report a case of malignant melanoma of the middle ear as a rare disease with a poor prognosis. Early diagnosis and treatment allow the patient to live a longer life. In addition to other diseases, malignant melanoma should be considered in the differential diagnosis when presenting symptoms such as constant pain in the ear and mastoid region, blood flow from the ear, swelling, redness, or dark color of the tympanic membrane, and loss of hearing in one ear.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
The design, data analysis and initial manuscript is done by F. S.; M. S. has participate in the study design and revision of the manuscript; B. L. and B. S. participated in data collection.
Ethical Approval
The study has been carried out in compliance with the Code of Ethics of the Helsinki Declaration, as well as the ethical approval from Ethic committee of the University Clinical Center of Kosovo (no. 913/2).
Informed Consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.