
Abstract
Background
To investigate the outcomes of using the residual thyroid cartilage for laryngeal function reconstruction in early glottic laryngeal carcinoma.
Methods
From March 2017 to June 2022, 21 patients with glottic carcinoma who underwent laryngeal function reconstruction were analyzed retrospectively. The operation was performed under general anesthesia. Reconstruction of ipsilateral hemilarynx defect by downward movement of ipsilateral residual thyroid cartilage plate. During the follow-up period, the laryngeal function and tumor recurrence were evaluated.
Results
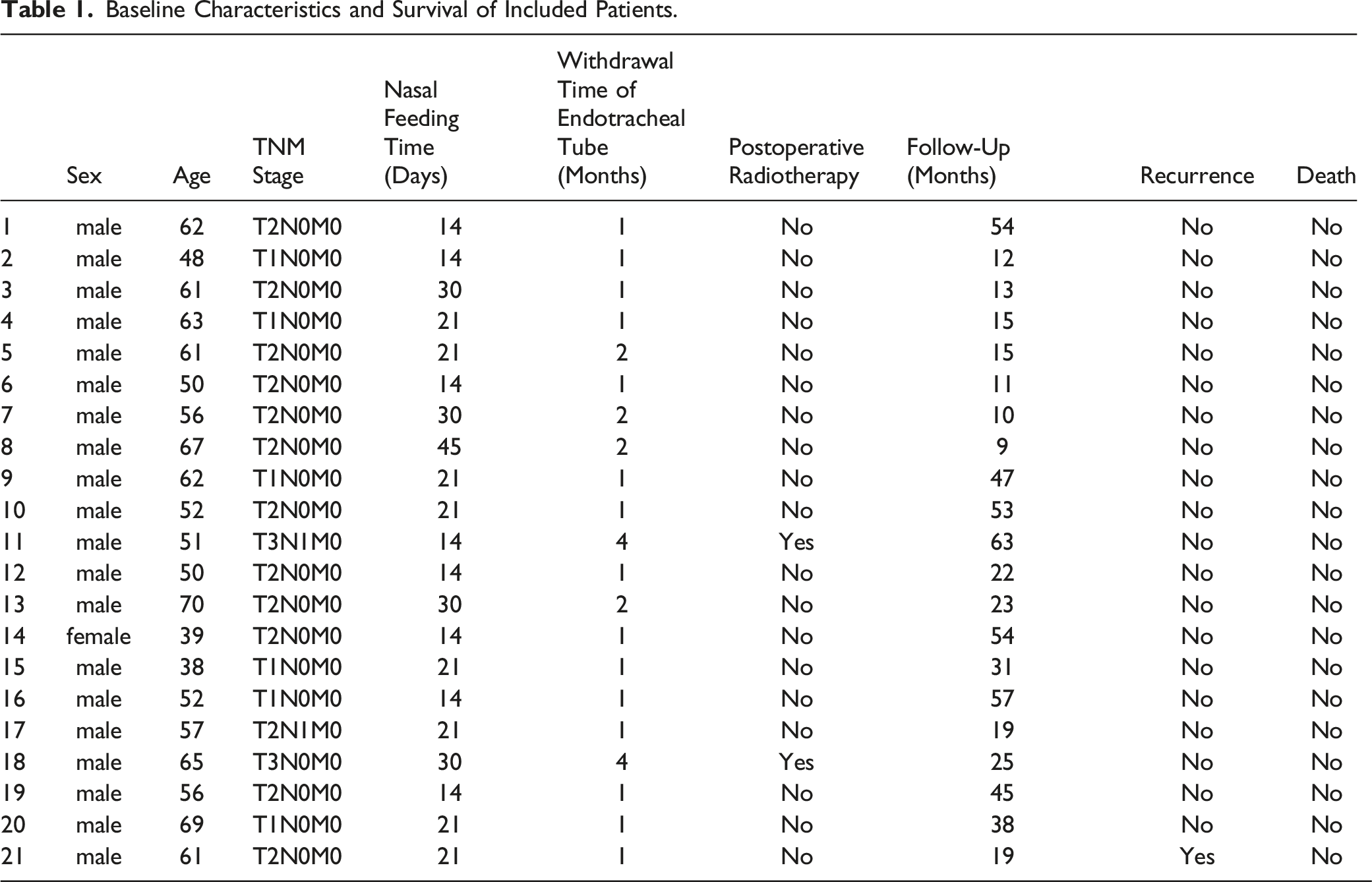
otally 20 male patients and 1 female patient were enrolled in this study. Of the 20 initial primary tumors, there were 6 patients with T1N0M0 stage, 12 ones with T2N0M0 stage, 1 with T1N1M0 stage, 1 with T3N0M0 stage, and 1 with T2N1M0 stage. The patient with recurrent tumor was T3N1M0 stage. The follow-up time ranged from 9 to 63 months. All patients were healed by first intention after surgery. All patients without laryngeal stenosis were removed from tracheotomy tube. So far, all patients have good laryngeal function. One patient relapsed at the last follow-up.
Conclusion
It is safe to repair hemilarynx defect with residual thyroid cartilage plate on the affected side, and it is an important choice for laryngeal function reconstruction after vertical partial laryngectomy.
Introduction
Vertical partial laryngectomy is the basic surgical method for unilateral lesion of glottic carcinoma. 1 Traditionally, it involves excision of the soft tissue of the affected vocal cord area and most or all of the ipsilateral thyroid cartilage plate. The defect can be repaired by various methods, including the use of epiglottis and band muscles to repair the lateral hemilarynx defect. 2 Previous studies have reported the use of a localized platysma myocutaneous flap or supraclavicular flap to repair the hemilaryngenal defect. 3 Patients with epiglottis pull-down repair would have obvious cough and poor pronunciation. Due to the lack of bone support in banded myofascial flap repair, a few patients will suffer laryngeal stenosis, and the extubation rate is relatively low. 4
According to our previous experience with patients who underwent various vertical laryngectomy, we found that patients with T1-2, even in some patients with T3 laryngeal carcinoma, the affected thyroid cartilage plate was pathologically free of tumor invasion or involvement, especially above the ventricular zone level. 5 In order to ensure the safety of tumor resection, we attempted to preserve the upper part of the affected thyroid cartilage plate as the framework of the larynx to reconstruct the postoperative defect of the affected half larynx. 5
In this study, we tried to explore the effectiveness of vertical partial laryngectomy with partial preservation of the affected thyroid cartilage plate in patients with glottic carcinoma.
Methods
Patients
Retrospective analysis of 21 patients with glottic squamous cell carcinoma treated in our hospital retrospectively analyzed. This study was approved by the Ethics Committee of our hospital.
Surgical Procedure
All operations were performed through oral intubation under general anesthesia. A transverse incision was made at the cricothyroid level, and the length of the incision was determined by whether neck lymph node dissection was performed at the same time. All T2 patients underwent selective ipsilateral grade II–III cervical lymph node dissection, and these lymph nodes were sent for intraoperative rapid pathological examination. The incision length was extended transversely from the anterior border of the sternocleidomastoid muscle on the healthy side to the mastoid apex level on the affected side. In the T1 patients, the incision was performed along the cricothyroid incision level and a transverse extension between the anterior margin levels of bilateral sternocleidomastoid muscles.
After skin incision, lift the flap along the deep surface of platysma, up to hyoid level and down to the lower edge of cricoid cartilage. If selective neck lymph node dissection is performed on the affected side, the flap is separated to the level of digastric muscle at the lower edge of submandibular gland and down to the level of supraclavicular on the same side. The anatomy of the ipsilateral grade II–III region is first used for intraoperative pathology. Then, the larynx is exposed by separating the bilateral banded muscles along the white line in front of the neck. The anterior laryngeal lymph nodes, pyramidal lobe of thyroid gland, and adipose connective tissue were also removed for pathology. Exposed cricothyroid membrane and bilateral cricothyroid muscles (Figure 1). (A). Separate the bilateral sternohyoid muscle along the anterior midline of the neck to expose the larynx. The cricothyroid membrane and cricothyroid muscle can be clearly displayed after resection of anterior laryngeal tissues, including thyroid vertebral lobe, anterior laryngeal lymph nodes and connective tissue; (B). the schematic diagram of the procedure.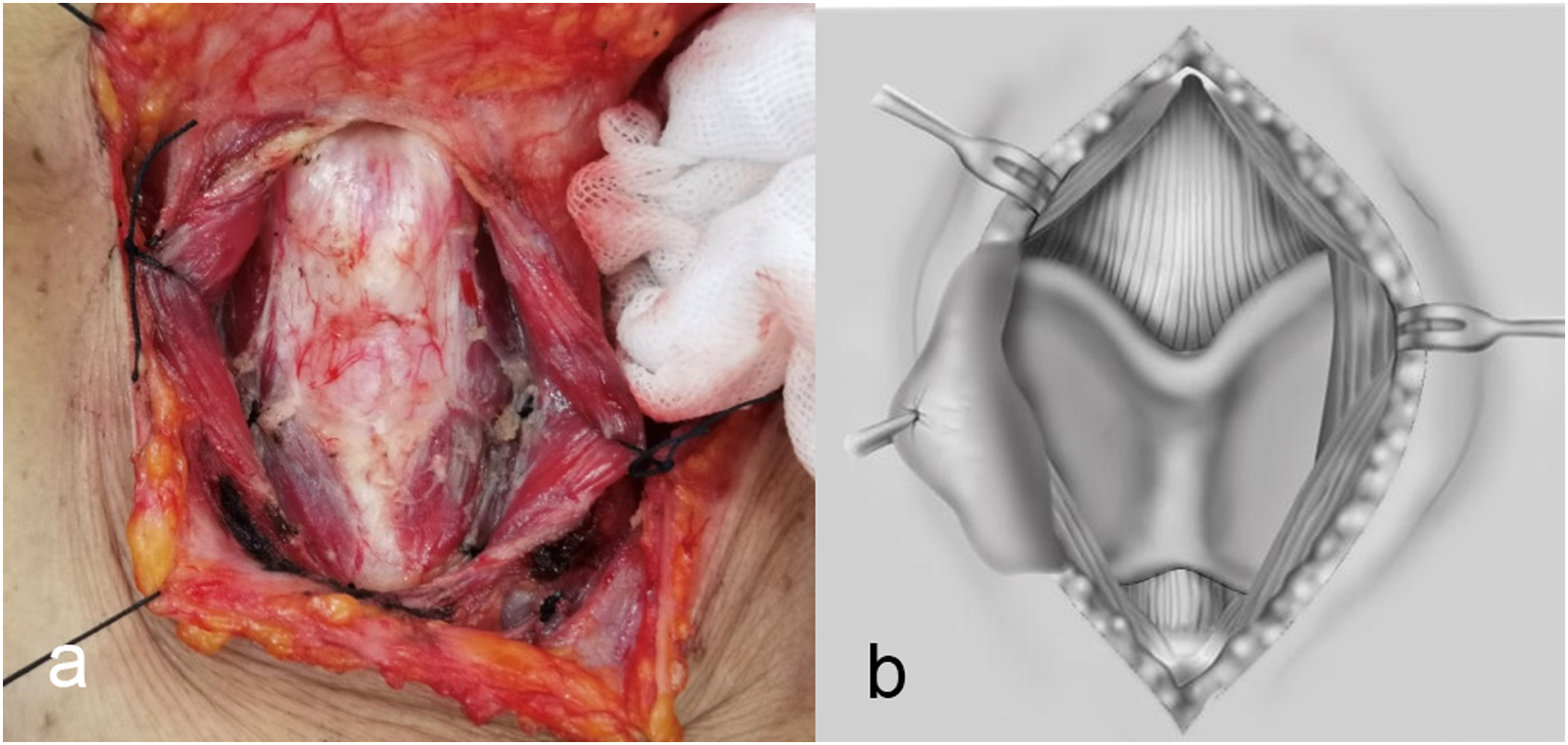
The location of the longitudinally laryngotomy and cricothyroid membrane incision on the healthy side of the thyroid cartilage plate were selected according to the extent of the laryngoscopic lesion, especially the involvement of the anterior commisure and contralateral vocal fold lesions (Figure 2). (A). according to preoperative laryngoscope and CT, mark the longitudinal and transverse incision range of thyroid cartilage of larynx; (B). the schematic diagram of the procedure.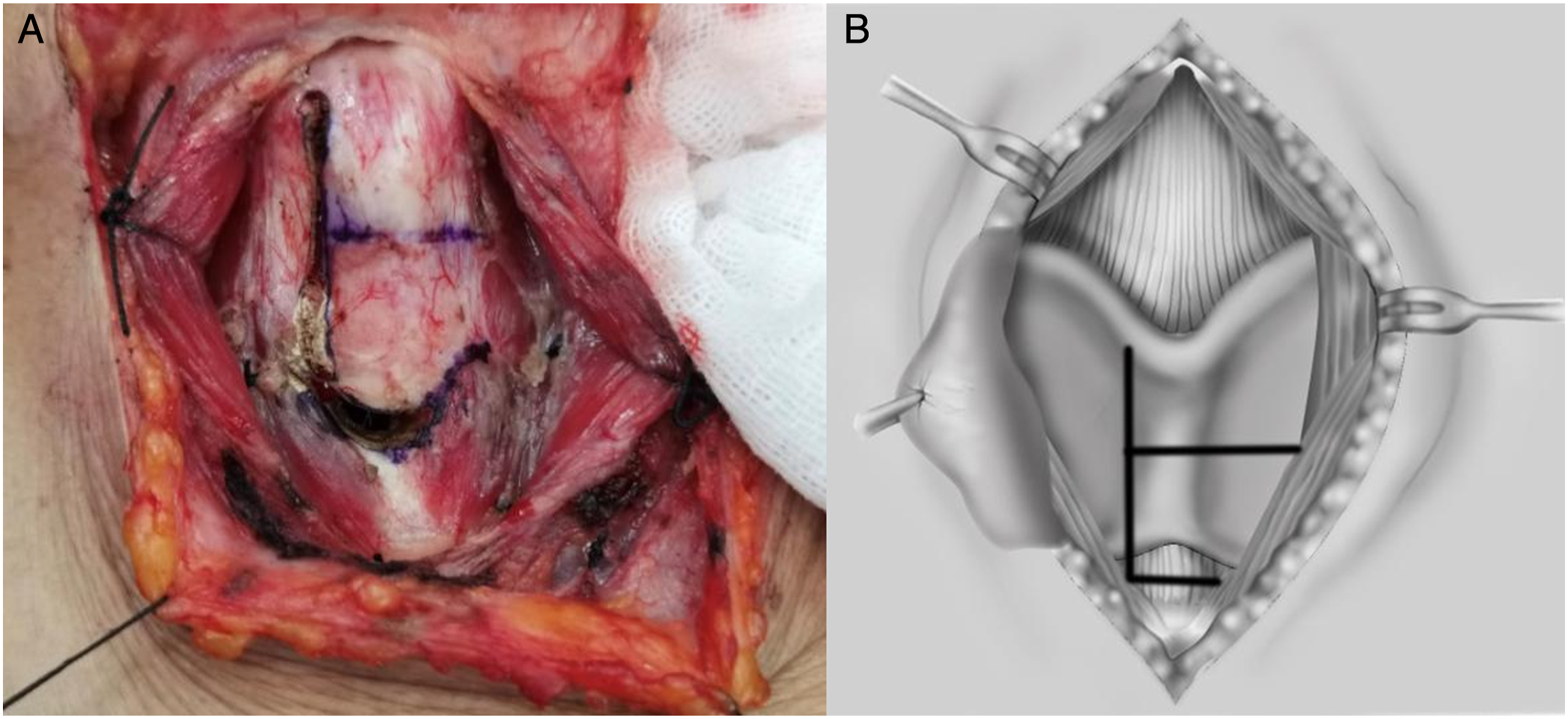
According to the degree of anterior cruciate injury under laryngoscope, healthy vocal cords can be cut within a safe range of 5 mm. The cricothyroid membrane under the vocal cords was also cut, and bilateral thyroid cartilage plates were retracted to expose the laryngeal cavity. Malignant lesions are exposed (Figure 3). (A). The thyroid cartilage plate of the healthy side splits longitudinally, exposing the laryngeal cavity, and the lesion of the affected glottis can be seen; (B). the schematic diagram of the procedure.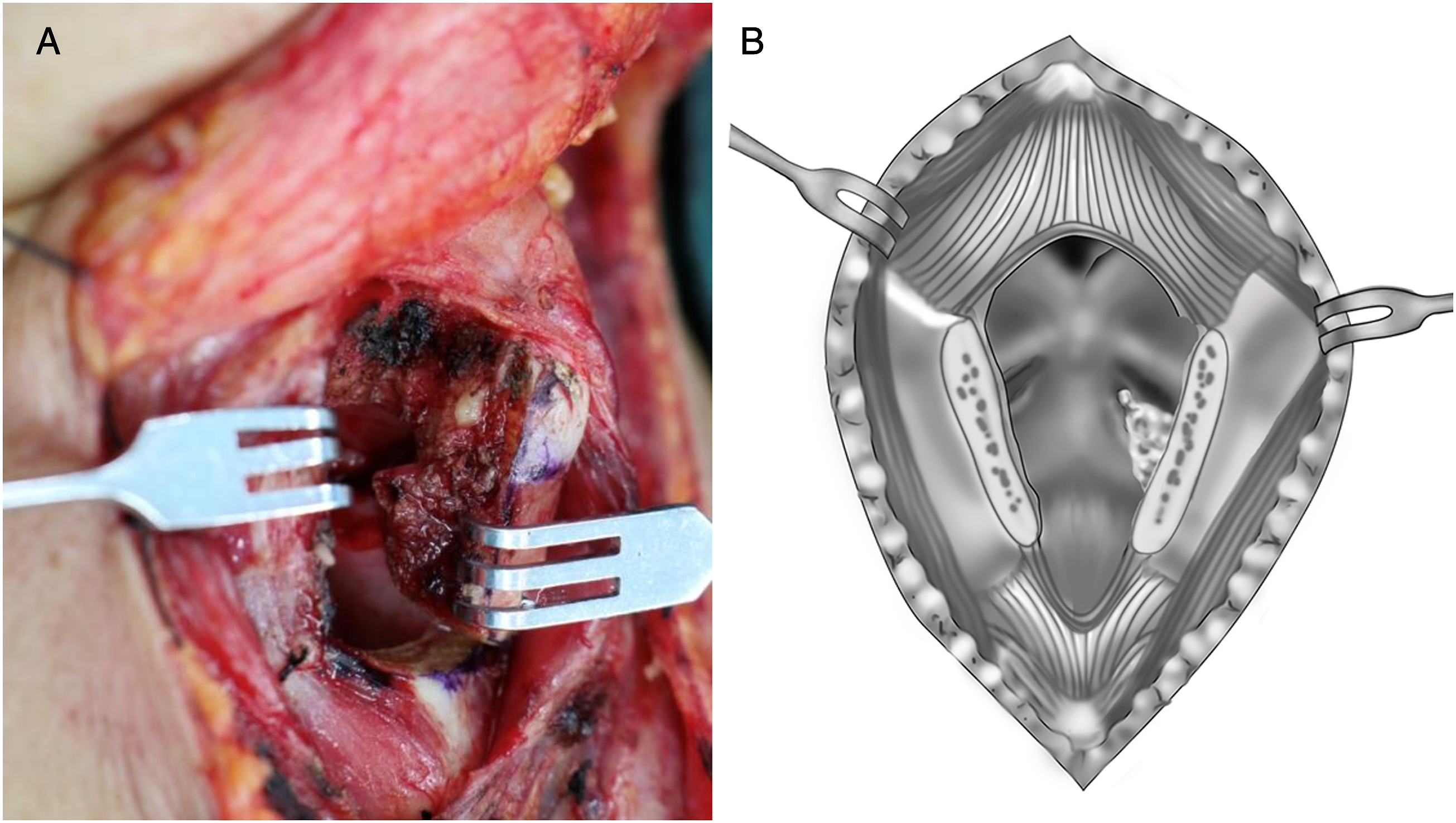
The affected thyroid cartilage plate was dissected transversely along the level of the affected ventricular zone. The inferior thyroid cartilage angle was transected horizontally to protect the recurrent laryngeal nerve on the affected side. vocal cords, paraventricular space, laryngeal chamber and some ventricular areas, and the proximal half of the inferior thyroid cartilage on the affected side were removed to ensure a safety margin of 3–5 mm (Figure 4). (A). The Gross specimen was showed during the operation, the lesion of the affected glottis along the 5 mm safe margin, together with the lower part of the affected thyroid cartilage plate. (B). The visual field of the affected side of the posterior laryngeal defect.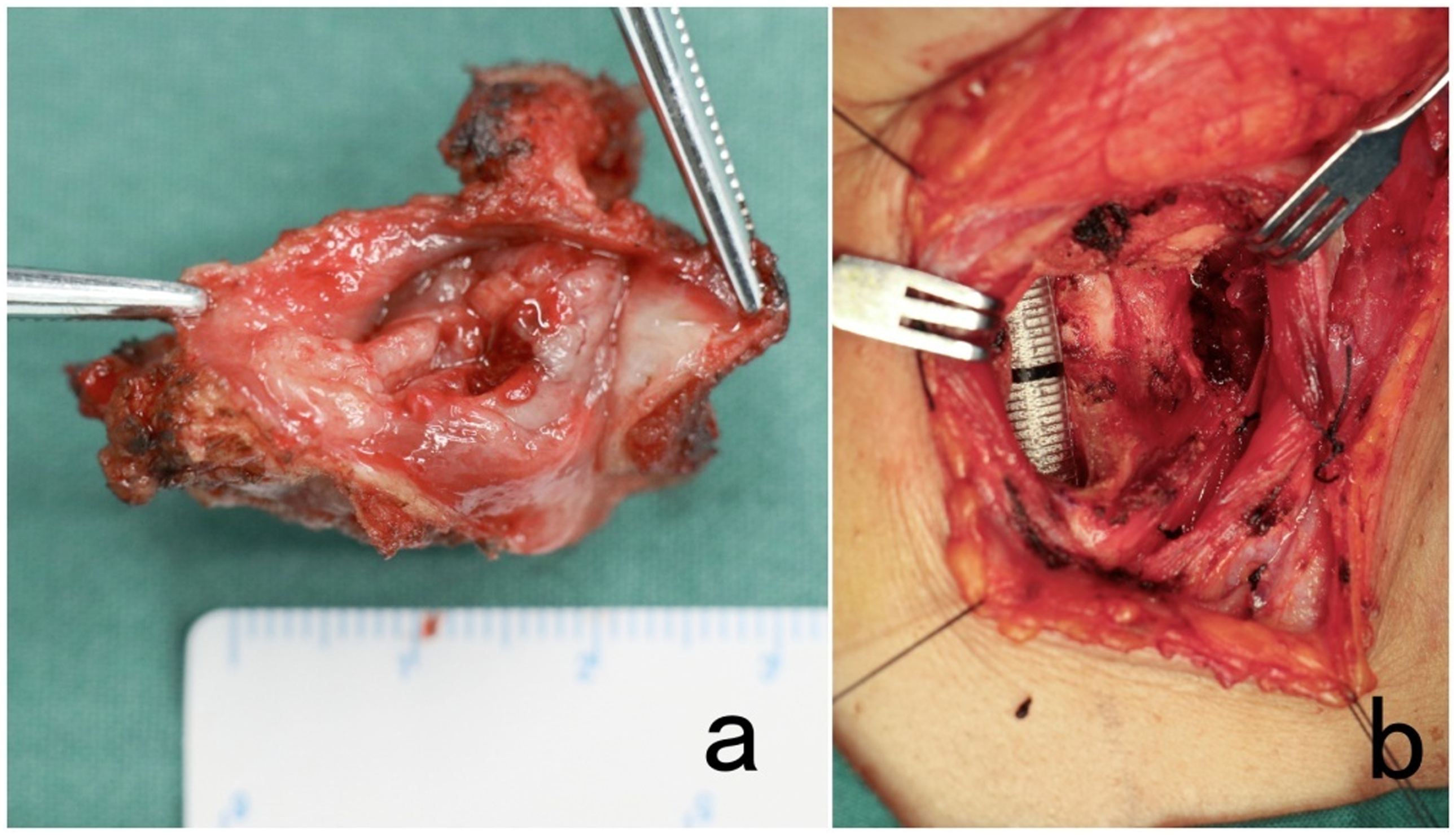
The edge of the incision was preserved during the operation. After the pathology turns negative quickly, thoroughly wash the wound and stop bleeding, and then the residual part of the ventricular band submucosa on the affected side was free pulled down, partially covering the residual cartilage wound with 3-0 suture to the inferior incision margin. In the same way, close the healthy ventricle and the posterior segment of the remaining vocal cords. The upper one-half of the residual thyroid cartilage plate on the affected side was appropriately dissociated and pulled down, then closed with 2-0 absorbable suture with the cricoid cartilage to reconstruct the hemilarynx. The laryngeal cavity was closed by suturing the thyroid cartilage plate (Figure 5). The anterior wall of larynx was strengthened with bilateral banded muscles. And after hemostasis and irrigation, the surgical cavity was closed and the drainage tube was placed. Routine preventive tracheotomy was performed. (A). The affected side is the left side, and the tumor does not involve the upper thyroid cartilage plate. After the tumor of the thyroid cartilage is removed, the remaining normal thyroid cartilage from the upper half is pulled down and sutured with the contralateral ring cartilage to reconstruct the laryngeal cavity of the patient; (B). the schematic diagram of the procedure.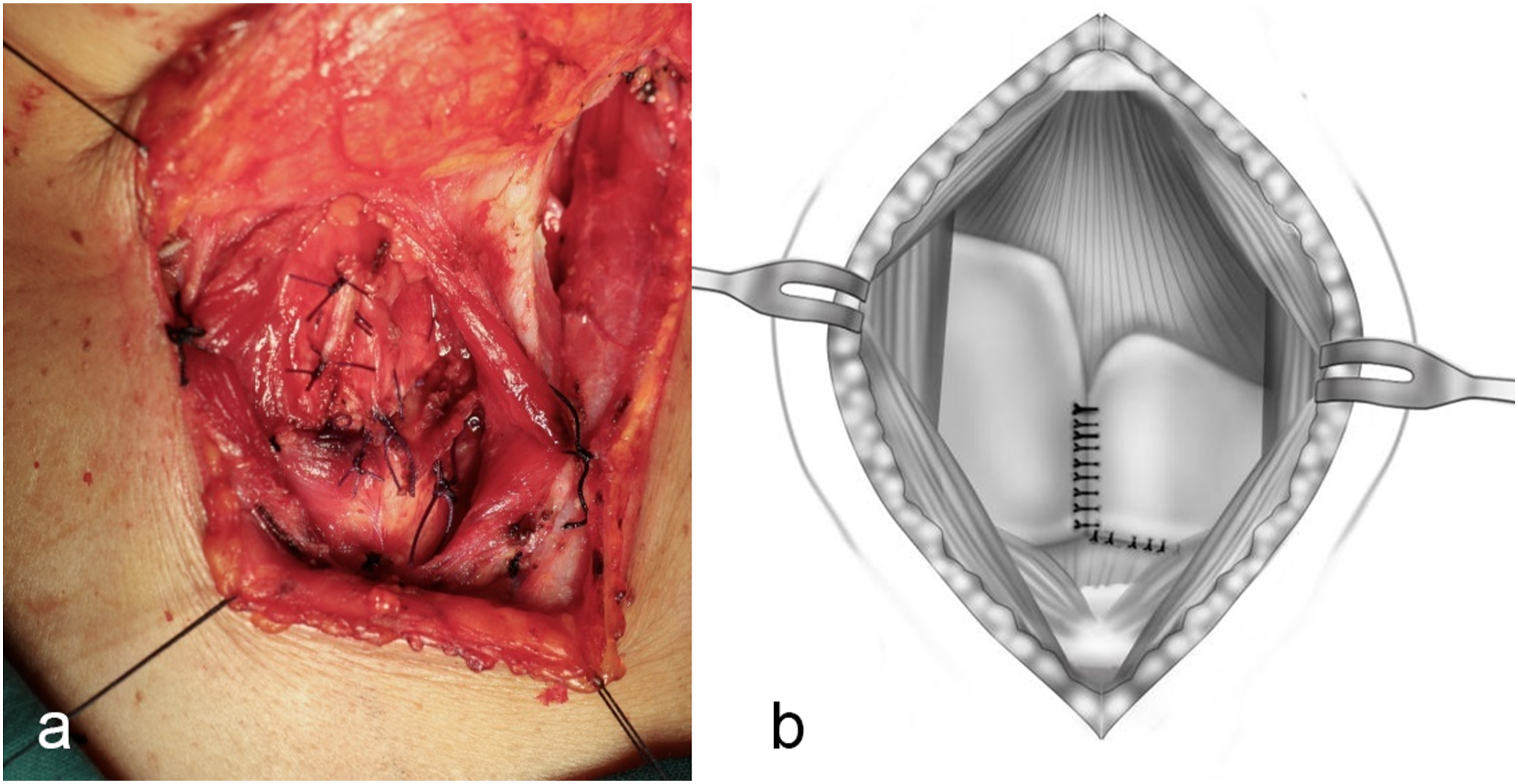
Statistical Method
SPSS software 26.0 was used for statistical analysis. The measurement data of normal distribution in this study is expressed as the average standard deviation.
Results
A total of 20 male patients and 1 female patient participated in this study. Among the 20 primary tumors, there were 6 cases of T1N0M0, 12 cases of T2N0M0, 1 case of T1N1M0, 1 case of T3NM0, and 1 case of T2N1M0. Patients with recurrent tumor are in T3N1M0 stage. The follow-up time was 9–63 months.
All patients were glottic laryngeal carcinoma, including 20 cases of primary laryngeal carcinoma and 1 case of recurrent laryngeal carcinoma. Of these 20 patients with primary laryngeal carcinoma, 19 patients are scheduled to undergo surgery with self-supporting laryngoscope. Because the lesion can’t be completely exposed under the laryngoscope, and the safety margin is insufficient, the open laryngeal surgery was changed. One patient with primary laryngeal carcinoma was unable to raise his head excessively due to internal fixation after cervical trauma, so he underwent open laryngectomy directly. Patients with recurrence after laser surgery also underwent direct open laryngeal surgery.
The average hospital stay is 7–10 days. The nasogastric tube was removed 10 ∼ 45 days after operation. Tracheotomy intubation was blocked 7 days after operation and removed 14 days to 2 months later. No laryngeal stenosis occurred. Postoperative radiotherapy was performed in 2 cases (1 lymph node metastasis, 1 T3 lesion and poorly differentiated squamous cell carcinoma). The remaining 19 patients did not receive postoperative radiotherapy.
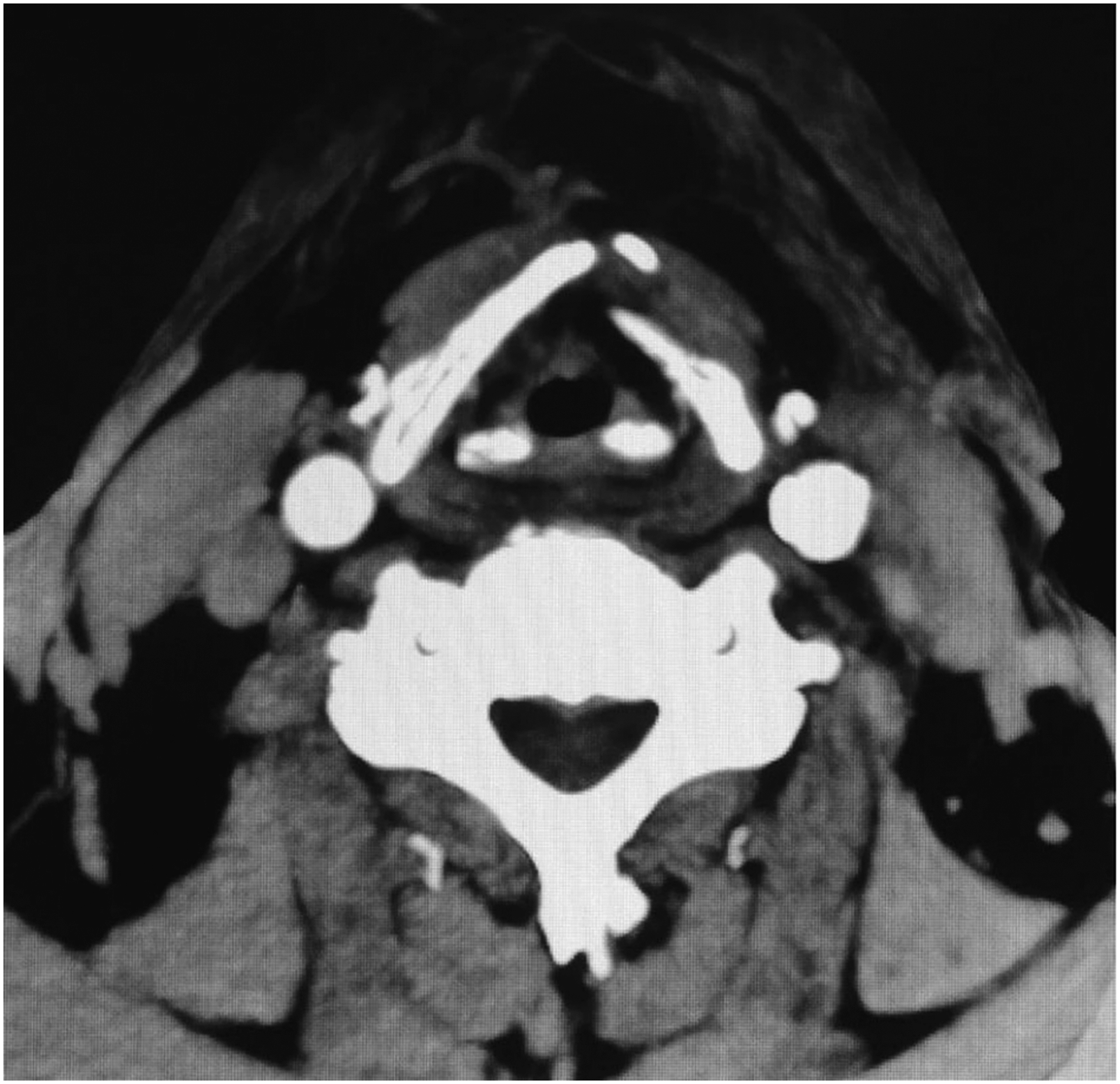
Postoperative laryngoscopy was performed every 3–6 months (Figure 6). Laryngeal enhancement computed tomography (CT) was performed 6 months after surgery (Figure 7). A laryngoscopic review was performed every 6 months, and CT review was conducted every year. All patients were with good laryngeal function so far. Only one patient experienced subglottic recurrence one year later, and a total laryngectomy was performed. (A, B). The reconstructed glottis was shown under laryngoscope after operation, (C, D). no tumor recurrence was found under narrow-band laryngoscope. CT after reconstruction of the left half larynx shows the shape of the left remaining thyroid cartilage after reconstruction of the left half larynx frame.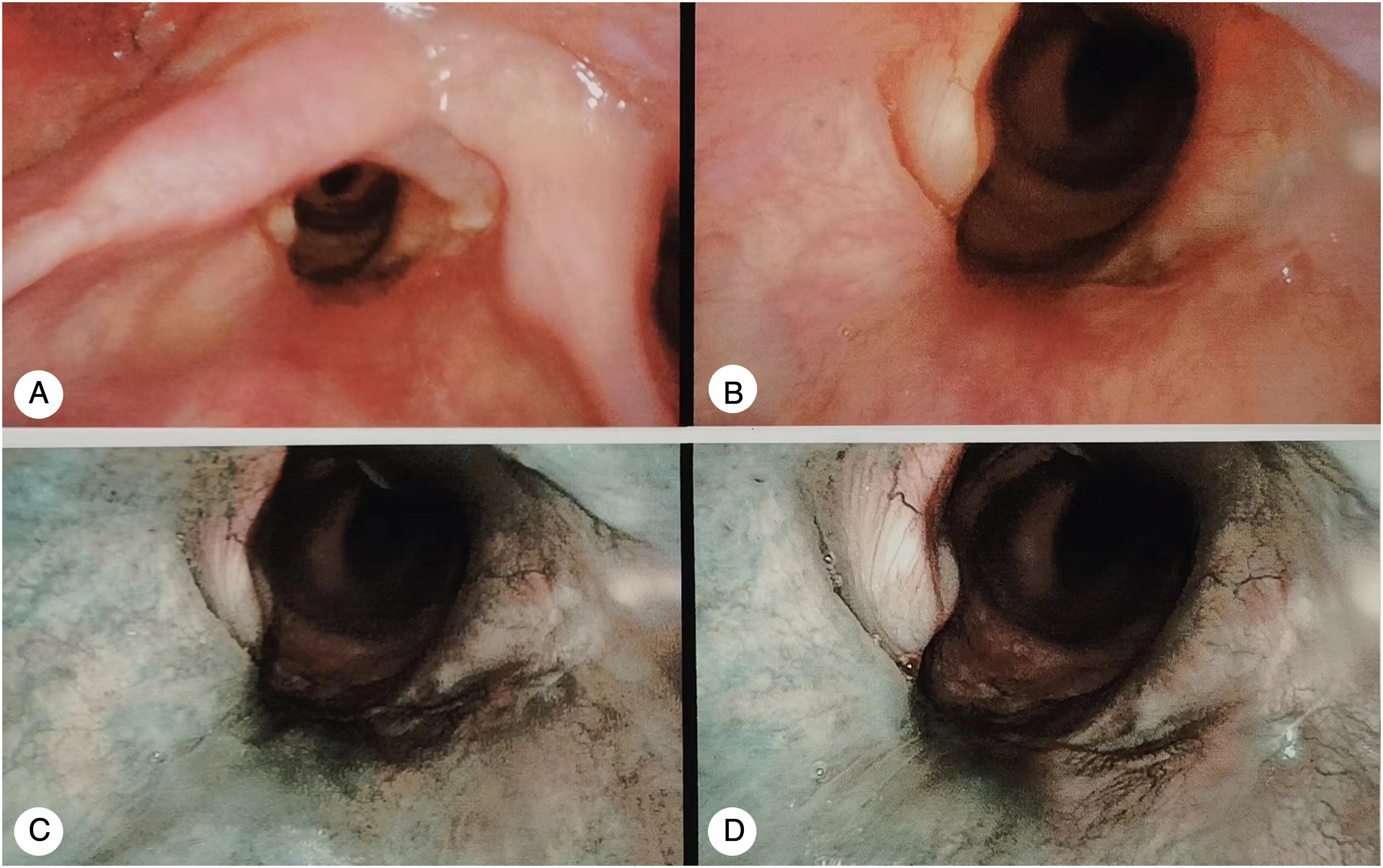
Discussion
With the development of medical technology, the goal of laryngeal cancer treatment is not only to achieve an ideal cure rate, but also to achieve the best functional prognosis. Radiation therapy has become the standard treatment for early laryngeal cancer. However, due to the medical and social background in China, radiotherapy is not always suitable for early laryngeal cancer, and surgery is the main treatment. Especially for patients with early glottic cancer, most patients in China use laser or plasma minimally invasive surgery under self-retaining laryngoscope to remove glottic cancer. The structure of larynx is preserved, and tracheotomy is not needed after operation. Patients recover quickly and have good pronunciation effect, which is the first choice for the treatment of early glottic cancer. 6 However, in clinical practice, some patients with glottic carcinoma, especially those with systemic complications, can’t be completely exposed under the laryngoscope, and the safety margin of minimally invasive surgery is insufficient. Therefore, these patients can choose open surgery or radiotherapy. 7
The open surgery for glottic laryngeal carcinoma with unilateral vocal cord lesions is the traditional vertical partial laryngectomy. The surgical resection includes a large part of the affected thyroid cartilage plate, vocal cord ventricular zone, and paraventricular structures on the affected side, and even the arytenoid cartilage. The hemilarynx defect of the affected side can be reconstructed by various methods, including pulling down epiglottis, ipsilateral banded muscles and local flaps, such as platysma myocutaneous flap. 8 Each type of repair is associated with certain advantages and disadvantages, such as the relatively poor quality of postoperative voice and heavy postoperative coughing in patients with epiglottis pull-down repair, the relatively high possibility of laryngeal stenosis with granulation scar after strap muscle repair, and the complicated The operation of skin flap repair is complicated and skin flap necrosis is easy to occur. In this study, the upper part of the remaining thyroid cartilage plate was used to reconstruct the laryngeal cavity. This surgical method is mainly for patients with T1–T2 glottic carcinoma. Most of these patients are not suitable for minimally invasive laryngeal support surgery. In this study, only T3 patients with no obvious thyroid cartilage invasion after imaging evaluation were strictly selected, but T4 patients were not selected. For patients with glottic laryngeal cancer at stage T3–T4, subtotal laryngectomy or total laryngectomy were the main surgical methods used.
According to our routine pathological observation of the thyroid cartilage plate on the affected side after vertical partial laryngectomy, most patients with T1–T2 and partial T3 glottic cancer have no tumor involvement or invasion of the thyroid cartilage plate. As shown in Figure 8, in order to reconstruct the rigid skeleton of the patient’s lateral hemilarynx and reduce laryngeal stenosis caused by postoperative hemilaryngeal collapse, we attempted to reconstruct the postoperative rigid hemilaryngeal defect by preserving the upper one-half of thyroid cartilage plate and moderately dissociating and pulling it down, which served as a cartilage scaffold of the larynx at the glottic level. The lower one-half of the thyroid cartilage plate on the affected side was excised, along with the paraglottic structures of the affected vocal cord and tumor, without affecting the safety of tumor removal. The reason we chose to use the top half of the thyroid cartilage was because using the bottom half of the thyroid cartilage might be much more dangerous than the top half, because cancer might increase the likelihood of cartilage erosion. Routine Conventional postoperative pathology ensures the safety of the surgical margin in conventional hemilaryngectomy, where the thyroid cartilage plate at the level of the vocal cords is completely removed. Theoretically, patients with partial involvement of the inner thyroid cartilage plate can also undergo safe resection.9,10 (A). The Gross specimen was showed after partial laryngectomy. (B, C). the tumor lesion was adjacent to thyroid cartilage plate, but no cartilage invasion was found under the microscope.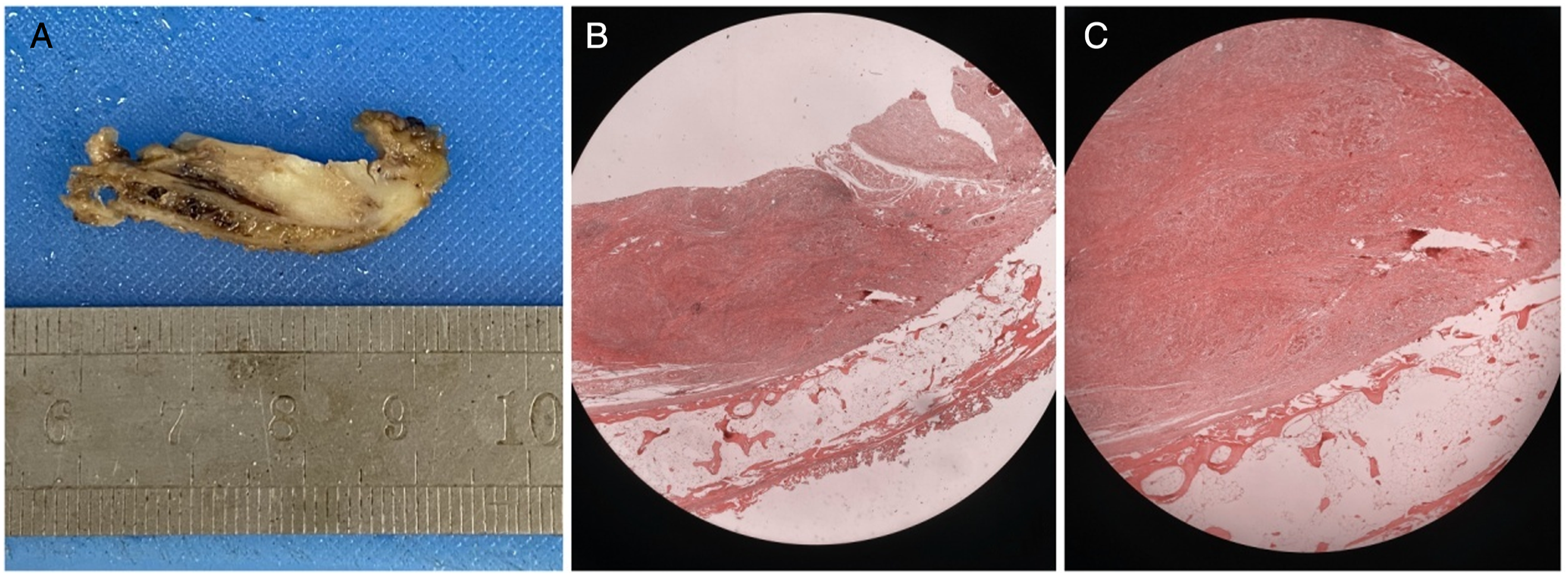
At the same time, the anterior commisure was removed along with the bilateral thyroid cartilage plate union through a 4-mm split in the median line of the healthy side of the larynx, ensuring safe resection of tumors with unilateral lesions involving the anterior comissure. The approach of healthy lateral ventricles of larynx makes use of the anatomical weakness of the lateral wall of larynx to quickly and accurately enter the laryngeal cavity, which is beneficial to observe the lesions in healthy vocal cords and keep the normal vocal cord structure. In our cohort, 21 patients could achieve a postoperative pathological safety margin of >5 mm, and no patients with tumor involvement of the cartilage were observed in consecutive sections of the tumor surface of the thyroid cartilage plate at the affected vocal cord level. In patients with lesions near the arytenoid cartilage, part or even all of the arytenoid cartilage is removed. In patients with anterior communication injuries, anterior communication is completely removed together with the anterior part of contralateral vocal cords and cartilage plates.
Baseline Characteristics and Survival of Included Patients.
This research also has some limitations. Firstly, there were unavoidable biases due to its retrospective nature. Secondly, it was an observational study without control cases resulting limited validity. Thirdly, it was a small sample study. Thus, all results should be interpreted cautiously, and it should be verified by prospective analysis in the future.
Conclusion
The improved vertical partial laryngectomy uses the residual thyroid cartilage plate pulled down from the affected side to repair the residual larynx, which ensures the maximum retention and improvement of laryngeal function. It is safe and effective for T1–T2 and selective T3 glottic cancer patients who are not suitable for minimally invasive surgery with laryngoscope.
Footnotes
Authors’ Contributions
PD L and ZG H contributed to the conception and design of the study; JZ, ZY, XH C, and XJ C performed the experiments, collected and analyzed data; PD L and ZG H wrote the manuscript; PD L and ZG H revised the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the Ethics Committee of Beijing Tongren Hospital. Informed consent was obtained from all the study subjects before enrollment.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.