
Abstract
Objective
To characterize the correlative factors for types of tracheobronchial foreign bodies (TFBs) encountered in children.
Methods
All included patients diagnosed with TFB underwent rigid bronchoscopy as the first surgery in the Children’s Hospital of Chongqing Medical University. The data of 1026 patients aged 0–18 years were retrospectively collected between February 2019 and January 2022.
Results
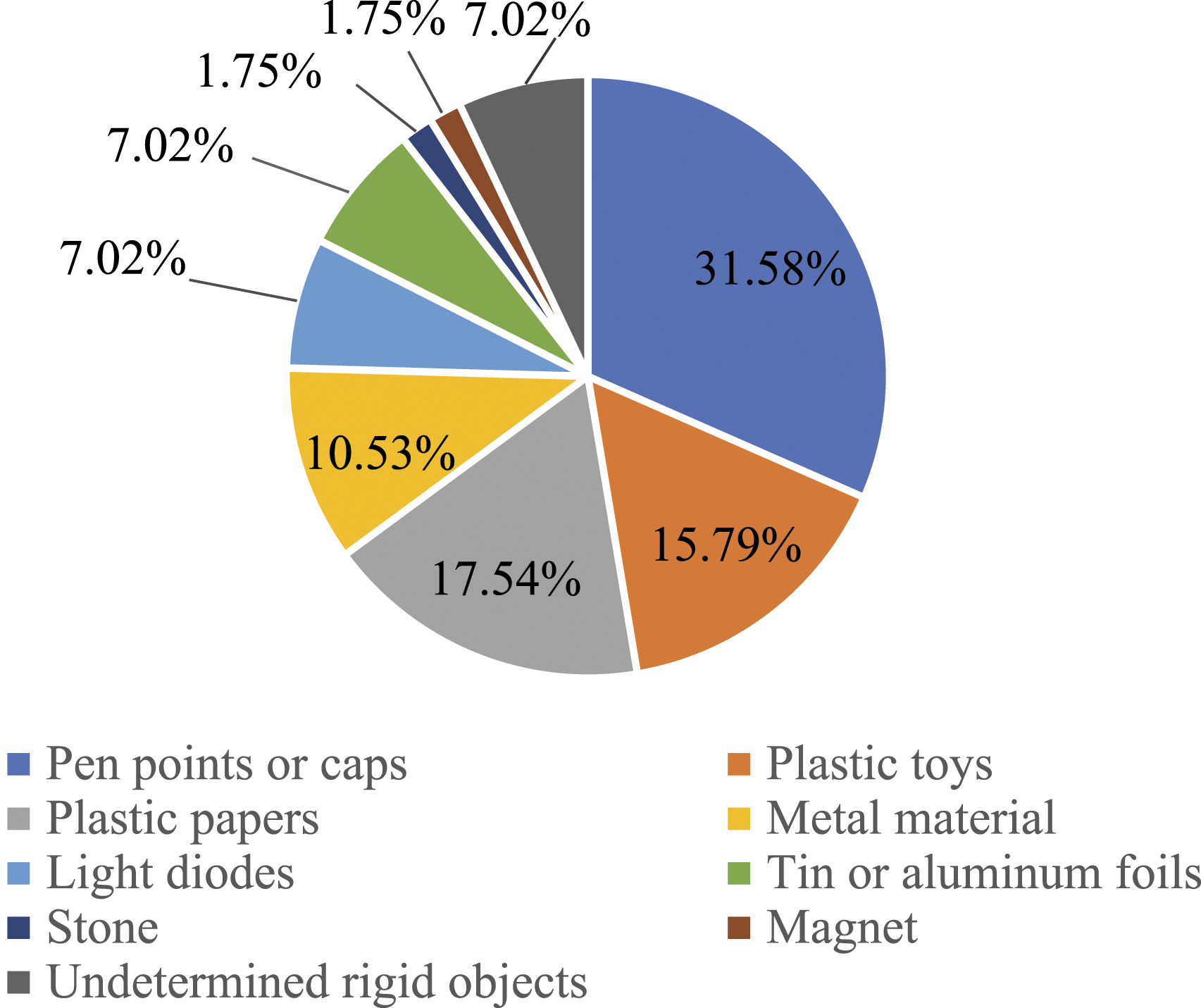
About 94.44% of the children with TFB had organic FBs, among which, peanuts were the most common FBs, followed by melon seeds and walnuts. The most common inorganic FBs included pen points or caps, plastic toys, and plastic papers. As compared to the children with organic FBs, those with inorganic FBs consisted of a higher proportion of children aged ≥3 years old, a time before surgery of >7 days, dyspnea, FBs size of >10 mm, longer operation time, more than two operation procedures, and atelectasis. On the other hand, the proportion of children with aspiration history, cough, and obstructive emphysema in the inorganic FB group was lower as compared to the organic FBs (P< .05).
Conclusions
The related factors related to the patient’s characteristics, symptoms, operation situations, and preoperative complications can be predicted based on the identification of FB type.
Introduction
Tracheobronchial foreign body (TFB) is a common critical disease in children. About 80% of TFB occurs among children with age ranging from 1 to 3 years and the peak TFB incidence occur in the 1–2 years age group.1-3 The most effective treatment for its removal is surgical intervention. Rigid bronchoscopy is a widely accepted standard procedure for the removal of TFBs in children.4,5 If not timely and effectively treated, it can cause serious complications, such as pneumonia, emphysema, atelectasis, bronchiectasis, and even respiratory and cardiac arrest.6-8 The severity of TFB risk depends largely on the nature and degree of obstruction determined by the location of FB. 9 Although several previous large-sample epidemiological studies were conducted on TFBs, only a few studies focused on the factors related to the location of TFBs.7,9 Moreover, studies on the related factors of TFB types are also lacking.
FBs can be classically divided into organic objects, such as peanuts, melon seeds, beans, fruits, and bones, and inorganic objects, such as pen points, pen caps, plastic paper, and plastic toys.2,10-12 In our previous study, we analyzed the clinical characteristics of 1328 children with FBs, 13 but did not focus on their types. Therefore, this study aimed to further analyze the specific types of organic and inorganic FBs while focusing on the correlative factors of the different types of FBs. The data on children with TFB were retrospectively collected from the Children’s Hospital of Chongqing Medical University, which providing services mainly for a large catchment population in southwest China.
Materials and Methods
Study Design and Data Collection
All the TFB patients aged <18 years, who underwent rigid bronchoscopy at the Children’s Hospital of Chongqing Medical University between February 2019 and January 2022 were retrospectively reviewed. Given the retrospective nature of the study, the data collected from the medical records were analyzed without obtaining consent from the patients. However, for rigid bronchoscopy, written informed consent was obtained from the patients or their guardians before performing it. The Medical Ethics Committee of the Children’s Hospital of Chongqing Medical University approved the study protocol.
TFB was confirmed by direct observation during bronchoscopy. Only those patients were collected from the department of Otolaryngology and thoracic Surgery, in whom rigid bronchoscopy was the first bronchoscopy performed. If the first procedure was not rigid bronchoscopy or TFB was not the primary cause of hospitalization, the patient was excluded from the study.
Study Methods
The data extracted from the medical records of TFB patients were as follows: age; gender; residential area (urban or rural); history of FB aspiration; a time before the first surgery; hospitalization time; clinical symptoms, such as coughing, wheezing/laryngeal stridor/laryngeal noise, fever, and dyspnea; endoscopic findings, such as type, diameter, and location of FB, and granulation tissue; surgery duration; and preoperative complications.
The time before the first surgery was defined as the time elapsed between the occurrence of the aspiration event, if witnessed, or from the onset of symptoms to the time of first surgery in the hospital. Chest computed tomography (CT) findings referred to the CT examination performed before the first attempt of removing TFB using rigid bronchoscopy. The surgery duration was defined as the operation time of the first rigid bronchoscopy.
Statistical Analyses
SPSS v23 statistical software (IBM, Armonk, NY, USA) was used for the data processing and analysis. The chi-squared test and Fisher’s exact test were used for the differential analysis of correlative categorical variables between organic FBs and inorganic FBs. A P-value <.05 was considered statistically significant for all the analyses.
Results
Type of TFBs
Among the total 1026 children with TFBs, 969 children (94.44%) had organic FBs, while 57 children (5.56%) had inorganic FBs. Peanuts were the most observed FBs, accounting for 47.88% of the organic FBs, followed by melon seeds and walnuts. The most observed inorganic FBs included pen points or caps, plastic papers, and plastic toys (Figures 1 and 2). Organic FBs in the children (n = 969). Inorganic FBs in the children (n = 57).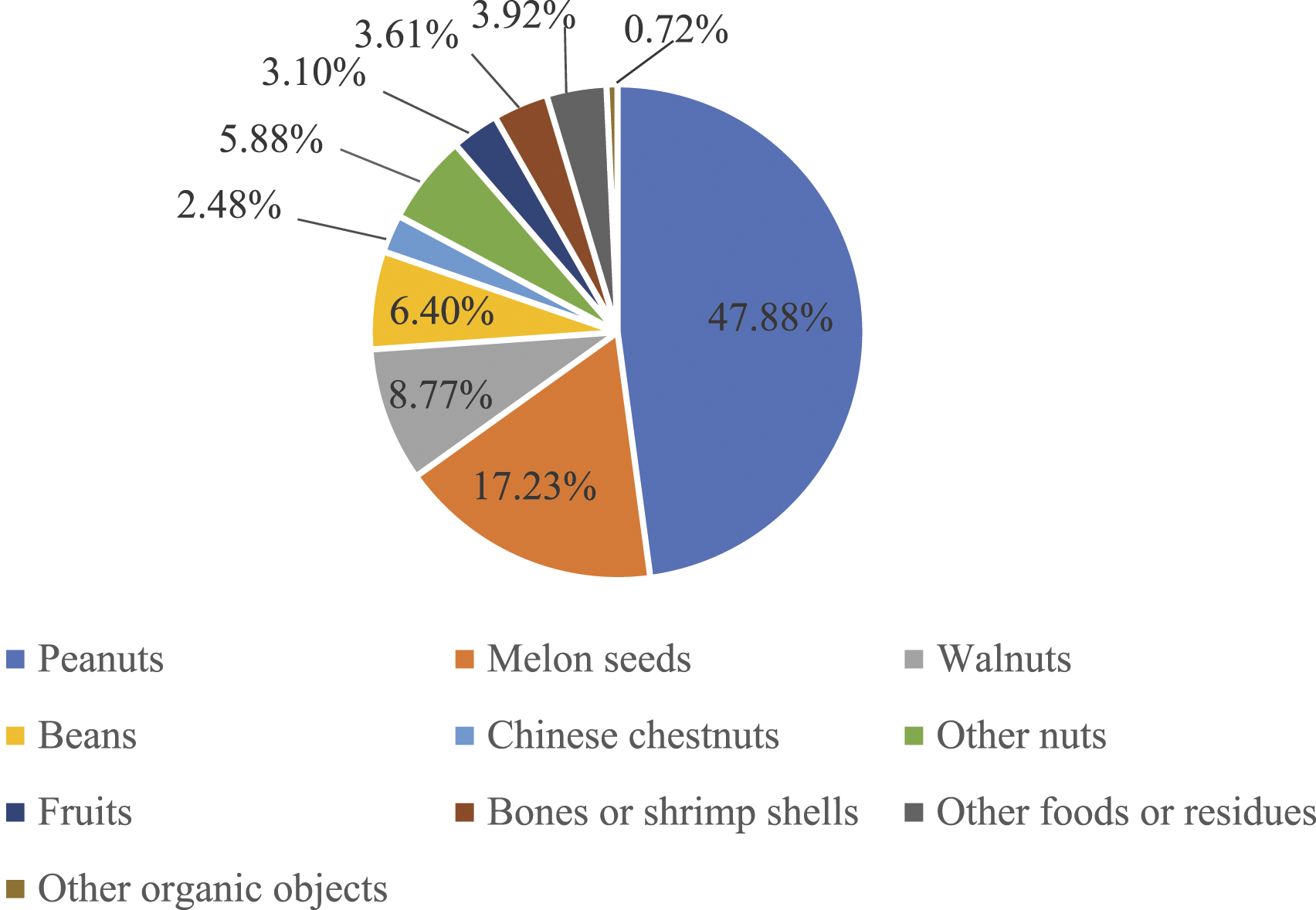
Results of Correlative Factors Analysis for the Type of TFBs
The Analysis of the Patients’ Characteristics and Symptoms in Different Type of Foreign Bodies (n = 1026).
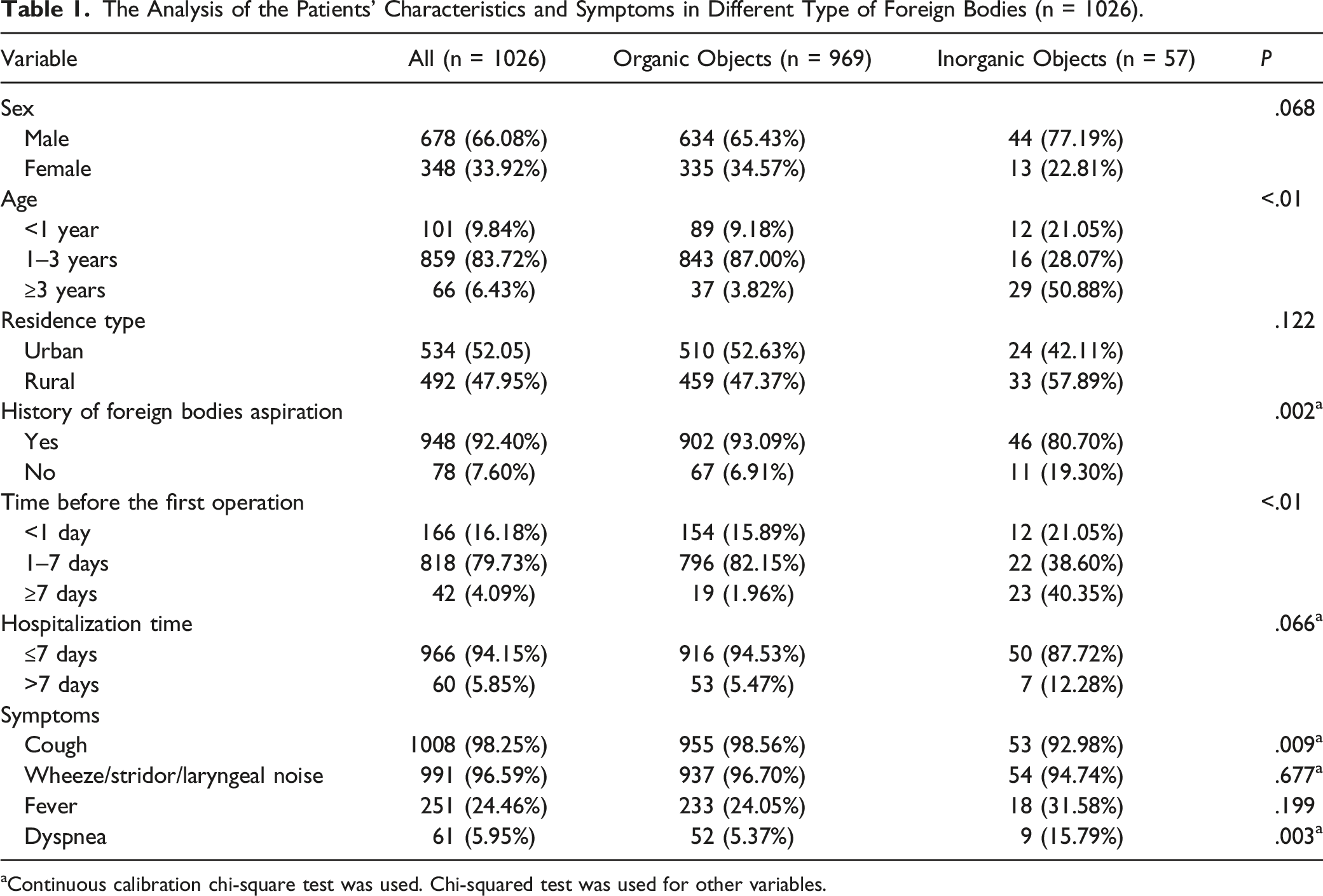
aContinuous calibration chi-square test was used. Chi-squared test was used for other variables.
The Analysis of the Preoperative Complications and Endoscopic Findings in Different Type of Foreign Bodies (n = 1026).
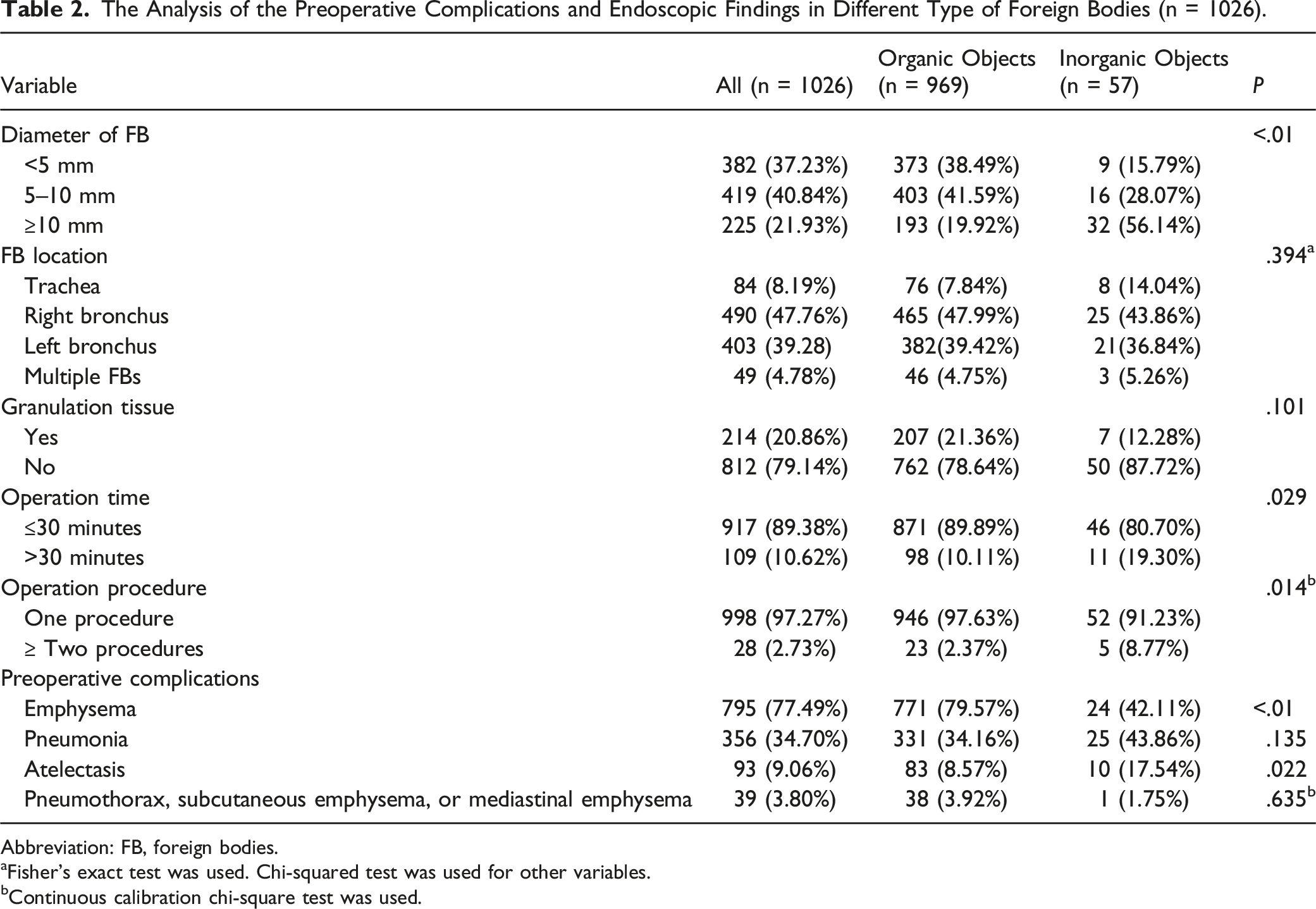
Abbreviation: FB, foreign bodies.
aFisher’s exact test was used. Chi-squared test was used for other variables.
bContinuous calibration chi-square test was used.
Discussion
This study showed that most of the children with FB were below 3 years old (93.57%), and the ratio of male to female was 1.95:1. The most common symptoms included cough (98.25%) and wheezing (96.59%), and FB was more likely to occur in right bronchus (47.76%). Obstructive emphysema and pneumonia were the most common complications. These finding about clinical features are similar to those observed in most previous epidemiological studies.2,3,7,10-13
The study found that the organic FBs were much higher compared to the inorganic FBs, accounting for 94.44% of the total FBs. This result was consistent with the previous studies, which reported that the proportion of organic FBs was 61–97.6%.2,10-15 The organic FB mainly included nuts, among which, peanuts were the most common, accounting for more than 40% of all the FBs. This result was consistent with the findings of most of the other studies at home and abroad.2,10,12,16-18 However, few studies reported the melon seeds as the most common FBs in other countries.3,19 This might be related to the dietary habits of different regions. Metal and plastic products were the most common inorganic FBs, which was consistent with the previous studies.2,3,10,16,19
This study further analyzed the clinical features, operation situation, and preoperative complications between the organic and inorganic FBs. As compared to the children having organic FBs, those having inorganic FBs had a higher proportion of children aged ≥3 years old, >7 days before the first operation, dyspnea, >10 mm FBs diameter, longer operation time, more than two surgical procedures, and atelectasis. On the other hand, the proportion of children with aspiration history, cough, and obstructive emphysema in the inorganic FB group was lower than those in the organic FB group.
The study showed that the proportion of organic FBs was higher than that of the inorganic FBs in all the age groups. The proportion of inorganic FBs in the children aged ≥3 years old was 50.88%, which was much higher than that in the children aged <1 year old and 1–3 years old. On the other hand, the proportion of organic FBs in children aged 1–3 years old was 87.00%, which was much higher than that in children aged <1 year old and ≥3 years old. This might be due to the absence of teeth, immaturity of the wallowing mechanism, eating when laughing or crying in the children aged <3 years old and the tendency of younger children to explore the environment through their mouths.18,20 Furthermore, the children aged ≥3 years were more likely to aspirate while playing with pen caps and other small toys in their mouths.21,22 However, another study showed that the proportion of inorganic FBs in the children aged <1 year old was higher than that in the children aged 1–3 years and ≥3 years old. 19 Therefore, more studies are needed in the future to explore the differences in the types of FBs in children of different ages.
The history of FB aspiration was the most important basis for the diagnosis of TFB. 1 The majority (92.39%) of children with FBs had a history of FB aspiration, which was consistent with the previous studies.3,18,23 This study also showed that the proportion of children with aspiration history in the organic FB group was significantly higher than that in the inorganic FB group (93.09% vs 80.70%). In addition, the proportion of children with visit time before surgery >7 days in the organic FB group was statistically less than that in the inorganic FB group. Zhou et al 24 also reported that the visit time for TFBs was correlated with the type of FBs. This might be because the most organics FBs (96.18% in this study) occurred among children <3 years old, who were often under the direct supervision of guardians all day long and could be witnessed aspirating an FB. Even if not witnessed aspirating an FB, their guardians might notice the symptoms of FBs aspiration, resulting in their timely treatment. However, the inorganic FBs were observed in more proportion of children (50.88% in this study) > 3 years old. These children were less likely to be witnessed aspirating an FB because they play alone without the direct supervision of guardians. Moreover, older children might not readily report the event to their guardians due to the fear of being scolded, even if they feel uncomfortable. These reasons might decrease reporting the history of FB aspiration and prolong the time before the first operation in the children aged ≥3 years.
Coughing is the most common symptom of TFB. The proportion of children with cough in previous studies was 70%-97.57%.10,16,18-20,25 In this study, 98.25% of the children had a cough, among which, the proportion of those with organic FBs was higher than that of the inorganic FBs. This might be due to the faster mucosa inflammatory action of organic FB, causing cough, while the inorganic FBs remain asymptomatic for a long time except in some asphyxia cases.26,27 In addition, the proportion of children with dyspnea was higher in the inorganic FB group as compared to the organic Fb group (15.79% vs 5.37%). This might be due to the higher proportion of FBs with a size >10 mm diameter among the inorganic FBs and location in the trachea as compared to that among the organic FBs, which made the inorganic FB more likely cause dyspnea.1,25
The current study showed that the proportion of FBs with a size >10 mm diameter among the inorganic FBs was higher compared to that among the organic FBs (56.14% vs 19.92%), while the proportion of FBs with a size <5 mm and 5–10 mm diameter among the inorganic FBs was significantly lower as compared to that among the organic FBs. This might be due to the type of FB because the most inorganic FBs are plastic and metal products with large diameters, such as pen tips, pen caps, and toys.2,3,10,16,19
According to the studies by Chen et al 11 and Li et al, 28 in this study, the longer operation time was defined as surgery of >30 min. This study showed that the proportion of longer operation time in the inorganic FB group was higher as compared to that in the organic FB group (19.30% vs 10.11%). In addition, the study also found that the proportion of ≥2 surgeries in the inorganic FB groups was significantly higher than that in the organic FB group (8.77% vs 2.37%). This might be due to the special nature of the most organic FBs, such as pen caps magnets and screws. These special FBs caused mechanical injury to the tracheobronchial mucosa and easily obscured the operating field by inducing bleeding upon removal. Moreover, these FBs were difficult to gasp using common forceps and remove from the airway with unnecessary injury to the airway mucosa and vocal cords.1,22 Therefore, these special FBs required longer operation times and more than one procedure for their removal. In addition, the history of FB aspiration and the variance between urban and rural might cause delay in treatment, 16 which might act as a risk factor leading to longer operation time. 11 Moreover, the experience of the surgeon and complications are also risk factors for longer operation time. Our study also confirmed that the incidence of inorganic FBs was significantly higher than that of organic FBs in patients with no aspiration history, the time before the first operation ≥7 days, and complications of atelectasis. Moreover, there was no statistical difference in the variance between the urban and rural populations in the two groups. However, Chen et al 11 suggested that there was no statistical difference in the operation time of different FB types. Therefore, more related studies are needed to further clarify these results.
Organic matter mostly comes from plants. Zhong et al 29 demonstrated that the plant FBs could cause lower respiratory tract infections. Bajaj et al 30 reported that the organic FBs were known to cause more complications. However, this study showed that there was no statistical difference in pneumonia caused by the organic and inorganic FBs. This result was consistent with that of a study by Lee et al 12 Another study also confirmed that the type of FB did not show evidence associated with the development of intraoperative and long-term complications. 20 Surprisingly, the current study showed that the incidence of obstructive emphysema was significantly higher, while that of atelectasis was significantly lower in the organic FB group as compared to the inorganic FB group. However, a few previous studies explored the association between the type of FBs and complications of obstructive emphysema and atelectasis. This might be possibly due to the higher (twice) incidence of inorganic FBs as compared to that of the organic FBs occurring in the trachea, which caused a lower possibility of obstructive emphysema in the unilateral lung in the inorganic FB as compared to the organic FBs. Another possible reason might be the easy absorbance of water by organic FBs, thereby forming airway obstruction. 30 For atelectasis, the harmful substances released by some inorganic FBs, which are retained in the bronchi, might damage the bronchial wall more seriously, leading to edema and collapsing the bronchial wall, thereby resulting in atelectasis of the lung lobe. Moreover, this study showed a longer time before the treatment of inorganic FBs as well as a larger size of inorganic FBs. Once the obstruction was formed, the bronchus was blocked to a greater extent, leading to the inability of external air to enter the alveoli and resulting in atelectasis.
There were some limitations to this study. Although the number of patients was large, this was a single-centered retrospective study. In addition, the FBs were divided into only organic and inorganic FBs. Moreover, this study did not consider the effects of the specific types on the pathogenesis of TFBs. Finally, other than the types of FBs, other factors, such as the location of FBs, visit time, and retention time might also affect the operation time, operation procedure, and complications.20,24,31 Therefore, more studies are needed to explore these correlations in the future.
Conclusions
This study suggested that the age, history of FB aspiration, a time before the first operation, symptoms (cough and dyspnea), the diameter of FB, operation time, operation procedure, and preoperative complications (emphysema, atelectasis) among the children with organic FBs were statistically significantly different as compared to those of the children with inorganic FBs. Therefore, the related factors about the patients’ characteristics, symptoms, operation situations, and preoperative complications can be predicted based on the identification of FB type.
Footnotes
Author Contributions
Shuping Su collected data and wrote the manuscript, Hengci Zhang finished statistical analysis, Ling Xiao and Hongbing Yao checked statistical analysis and manuscript, and Ling Ding proposed ideas and finished project administration. All authors have contributed to, read, and approved this submitted manuscript in its current form.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Disclosure
Our manuscript hasn’t received prior publication and isn’t under consideration for publication elsewhere.