
Abstract
Tumoral calcinosis is a rare benign disease defined as calcium salt deposits in the periarticular soft tissue region. Tumoral calcinosis is rare in the neck and larynx. In this case, we described a 58-year-old man who had numerous calcified nodules in the larynx.
Intoduction
Tumoral calcinosis is a benign disease in which calcium is deposited in the periarticular soft tissues. 1 It is usually deposited around large joints, such as the shoulder, elbow, and hip, and occasionally occurs in the wrist and small joints of the hand. 2 It is rare in other areas. Tumor calcinosis in the larynx is rare, and reported cases are multiple lesions, secondary to chronic renal disease, and associated with the neck.3,4 Herein, we report the first case of primary solitary tumoral calcinosis in the larynx without involving the neck.
Case Report
A 58-year-old man without any chronic renal disease presented to the Otolaryngology Head and Neck Surgery clinic with a 10-day history of the neoplasm of false vocal cord. He had persistent hoarseness without dysphagia, dyspnea, cough, fever, or night sweats. No surface masses were found on physical examination. On flexible laryngoscopy, we found a hemangioma-like mass on the left side of the root of the laryngeal surface of the epiglottis, hypertrophy of the left false vocal fold and fullness of the laryngeal ventricle, mild edema of the left vocal folds, and good movement of the vocal folds (Figure 1). A hemangioma-like mass on the left side of the root of the laryngeal surface of the epiglottis, hypertrophy of the left false vocal fold and fullness of the laryngeal ventricle.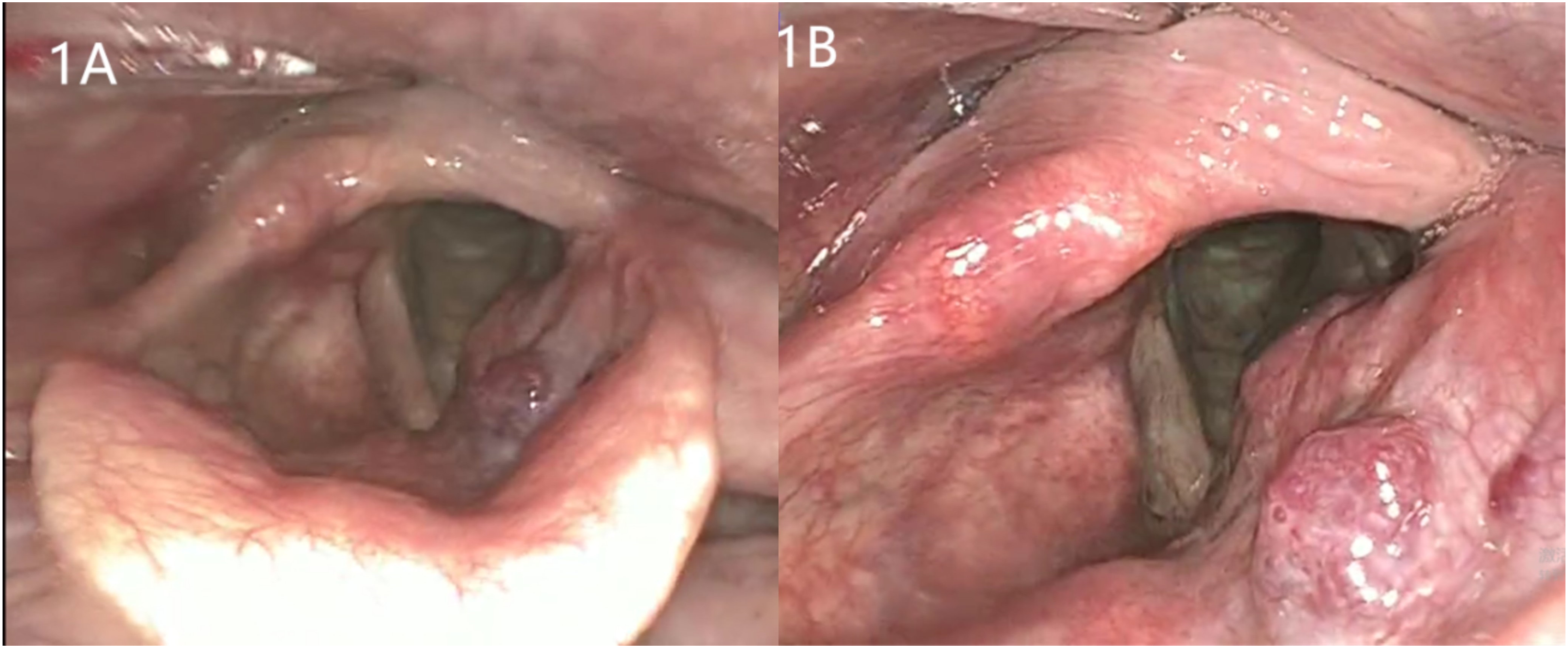
A computed tomography (CT) scan demonstrated soft tissue nodules in the left paraglottic space and pre-epiglottic space containing numerous small nodule-like calcifications. The mass showed mild enhancement in the venous phase of contrast-enhanced CT scans (Figure 2). Laboratory results showed that the levels of serum calcium, serum phosphorus, serum alkaline phosphatase, serum uric acid, parathyroid hormone (PTH), and blood lipids are within normal limits. The CT shows multiple small nodular calcifications in the soft tissue nodules, and the mass is confined to the soft tissue without invading the surrounding cartilage. (A) and (B) are axial CT images that show multiple small nodular calcifications in the left paraglottic space. (C) and (D) are sagittal and coronal CT images, respectively, showing the mass extending from the hyoid bone to the supraglottis and reaching the medial edge of the thyroid cartilage laterally.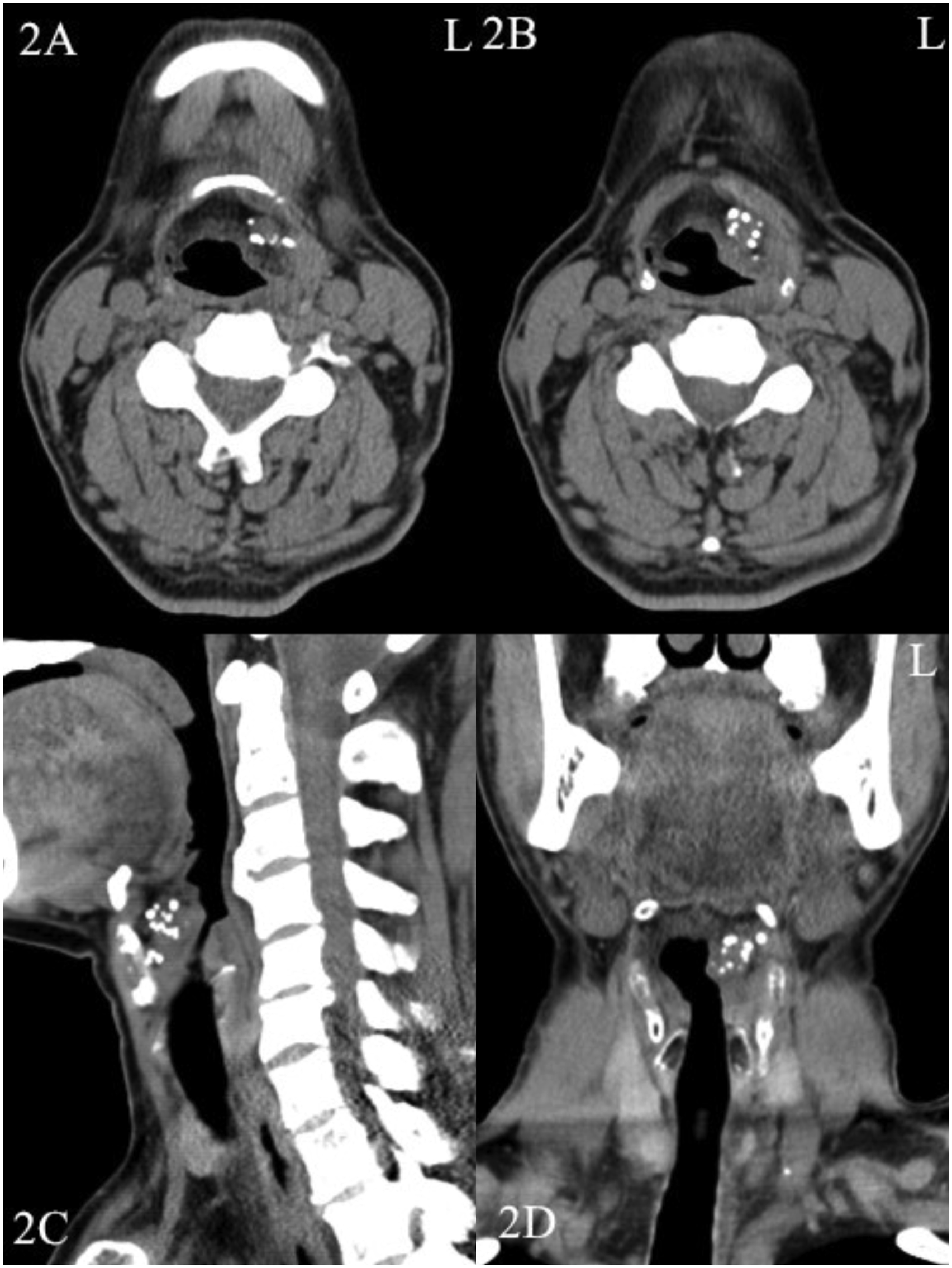
The laryngeal neoplasm was removed using microscopic low-temperature plasma radiofrequency ablation. Histopathological findings showed numerous calcified nodules of vitreous degeneration, transverse muscle and mucosal intrinsic glands with local lymphocytic infiltration, chronic mucositis with interstitial fibrous tissue hyperplasia and mucosal intrinsic glandular hyperplasia, and vascular hyperplasia and dilation (Figure 3). One month after surgery, the patient's hoarseness was still present with no other special discomfort. CT and fiberoptic laryngoscopy showed no new lesion. The patient's serum calcium, serum phosphorus, serum alkaline phosphatase, serum uric acid, parathyroid hormone (PTH), and lipids were all within the normal range. Histopathology (low magnification HE staining) showed chronic mucositis, interstitial fibrous hyperplasia with intrinsic glandular hyperplasia, numerous calcified nodules with glassy degeneration and local lymphoid infiltration.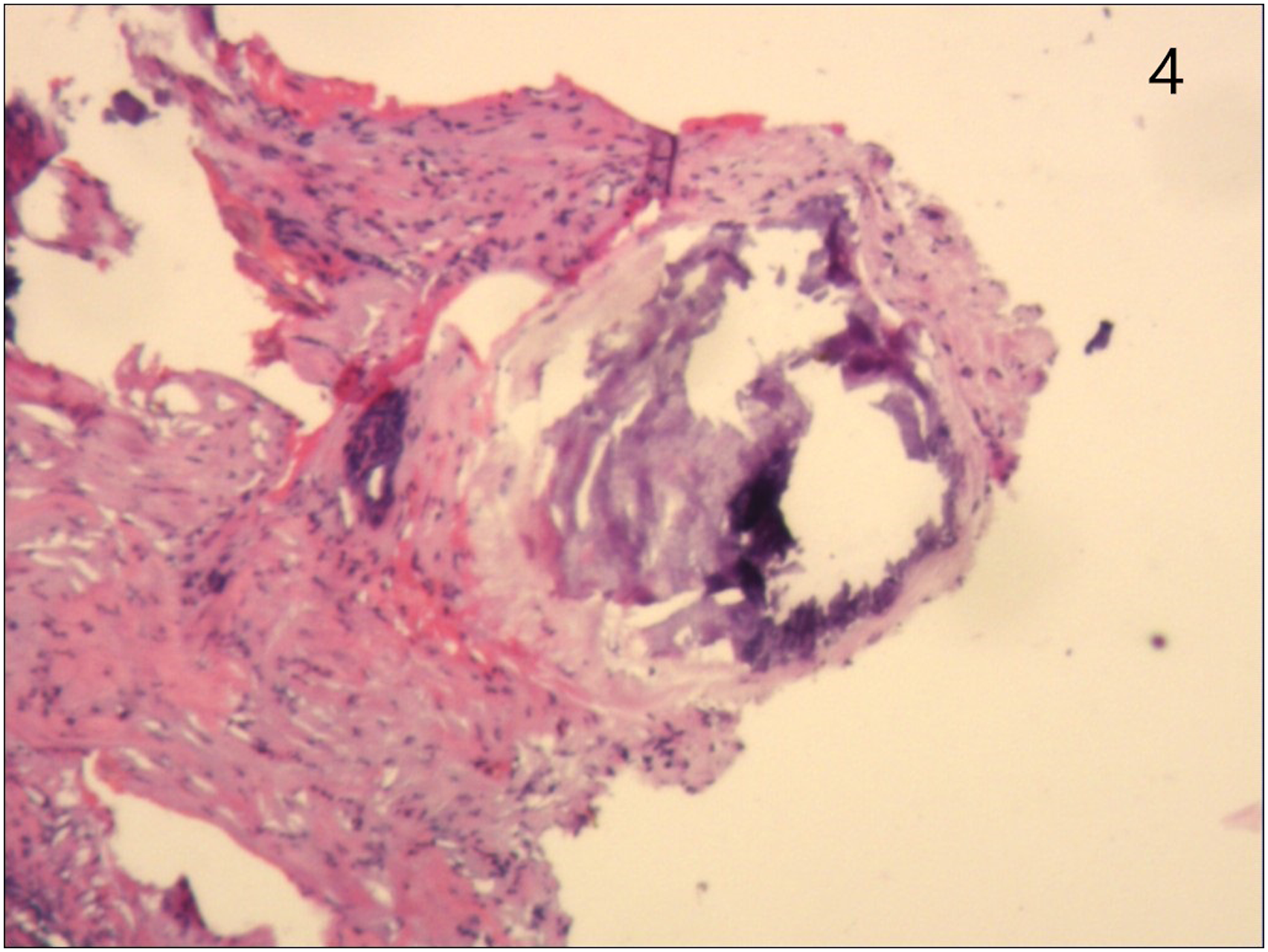
Discussion
Tumoral calcinosis is classified into 3 major categories according to the etiology: primary normophosphorus tumoral calcinosis, primary hyperphosphorus tumoral calcinosis, and secondary tumoral calcinosis. 5 Primary normophosphorus tumoral calcinosis refers to normal serum calcium and phosphorus without a history of soft tissue calcification-related disease. Primary hyperphosphorus tumoral calcinosis is defined by high serum phosphorus levels, normal serum calcium levels, and a lack of a history of soft tissue calcification-related disease. Secondary tumoral calcinosis is a disorder in which the patient has other conditions associated with soft tissue calcification. The specific pathogenesis of tumor-like calcium deposits is still unclear. It may be related to abnormalities in calcium, phosphorus, and cholesterol metabolism, immune dysfunction, genetics, and other factors. 6
The diagnosis of tumoral calcinosis is based on clinical symptoms, laboratory investigations, imaging, and pathological examinations. Any tumor-like calcium deposits around the joints are now considered tumoral calcinosis, regardless of the patient's age, gender, or disease history. 2 However, the reported cases so far include not only tumor-like calcium deposits around joints but also those in the neck, colon submucosa, etc.3,4,7 Therefore, we believe that tumor-like calcium deposits around joints are classical tumoral calcinosis, but tumor-like calcium deposits around non-joints (except teeth and bones) are also atypical tumoral calcinosis. Typical clinical manifestations of tumoral calcinosis are swelling and pain at the site of the mass, limitation of movement, etc. Abnormalities in laboratory tests, including serum calcium, serum phosphorus, serum alkaline phosphatase, serum uric acid, etc., can indicate tumoral calcinosis. Imaging examinations include X-ray, CT, and MRI, etc., and tumoral calcinosis has different features on different imaging examinations. The imaging features of tumoral calcinosis on CT are lobulated, nodular, and mass-like foci of calcification. 8 The histological manifestation of tumoral calcinosis consists of two phases: the active phase and the inactive phase. 2 The active phase is characterized by central calcified granules surrounded by an infiltration of inflammatory cells (consisting mainly of epithelioid histiocytes, mixed with several lymphocytes, and scattered macrophages). In the inactive phase, there is no inflammatory cell infiltration, only calcium deposits and dense collagen fibers. In this case, the histopathological section of the tumoral calcinosis mainly showed a large number of calcified nodules and interstitial fibrous tissue hyperplasia, so it should be in the inactive stage. The differential diagnosis of laryngeal masses with calcification includes laryngeal cancer, laryngeal amyloidosis, and infectious diseases of the larynx.9,10
The treatments for tumoral calcinosis include etiological treatment and symptomatic treatment. The choice of treatment is based on the etiology. Treatment of the primary cause of secondary tumoral calcinosis is critical. Because the pathogenesis of primary tumor-like calcium deposits is not clear, control of serum calcium and phosphorus levels, pain reduction, and surgical resection are generally used to control the progression of the disease and reduce complications until etiologic treatment is achieved. Since the effectiveness of surgical treatment is not entirely favorable and there is a risk of postoperative recurrence and non-healing wounds, surgical treatment is mainly aimed at patients with chronic infections due to tumor-like calcium deposits and those whose quality of life is affected. 6 In this case, the patient had tumor-like calcium deposits in the larynx with an atypical clinical presentation, no specific medical history or family history, and no abnormalities in laboratory tests. Because the CT findings and histopathological findings were consistent with tumoral calcinosis, it was a primary normophosphorus tumoral calcinosis of unknown etiology. Since the patient's calcium deposition occurred in the larynx, resulting in persistent hoarseness affecting the patient's daily life, other relevant laboratory indications did not show significant abnormalities, and the possibility of a malignant tumor could not be excluded, the patient was treated with surgery alone.
Conclusion
Tumoral calcinosis isolated to the larynx is rare. It should be distinguished from other laryngeal diseases to avoid misdiagnosis and misdiagnosis, and it should be taken seriously in clinical work.
Footnotes
Author’s Note
Informed consent was obtained from the patient, and the study was approved by the Ethics Committee of the Sixth Medical Center, PLA General Hospital
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee of the Sixth Medical Center, PLA General Hospital, Beijing Province, China
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Data Availability
All authors had full access to all of the information in this article. The data that support the findings of this study are available from the Corresponding author, upon reasonable request.