
Abstract
Significance Statement
Nasopharyngeal angiofibroma rarely presents in post-adolescent and elderly men, either as the natural evolution of a pre-existing lesion or as a de novo skull-base tumor. As the lesion ages, its composition changes from vessel-predominant to stroma-predominant—the angiofibroma–fibroangioma spectrum. As a fibroangioma, it has restrained clinical features (asymptomatic or occasional epistaxis), minimal avidity for contrast agents, and limited spread potential evident on imaging. These atypical features lead to a diagnostic dilemma when an innocuous choanal/nasopharyngeal fibrovascular mass is encountered in hitherto asymptomatic adult men presenting with epistaxis.
Text Proper
A 47-year-old man [patient#1] presented with the history of two episodes of brisk epistaxis within a span of three weeks. They were abrupt in onset and relieved spontaneously. He denied any history of trauma or having symptoms of rhinosinusitis. He had no known comorbidities and was otherwise healthy. Regional examination of head–neck was unremarkable.
Subsequent naso-endoscopy revealed a mucosa-covered, firm, non-tender choanal mass that did not bleed on touch (Figure 1). It was attached to the anterior wall of sphenoid sinus infero-lateral to its ostium and was closely apposed to the posterior aspect of inferior turbinate. It had a mottled appearance on imaging, without any evidence of bone destruction, expansion, or remodeling (Figure 2). Since the lesion was essentially non-enhancing, angiographic studies were not performed. Endoscopic view of the choanal mass in the two patients (A–E, patient#1, left side; F, patient#2, right side). The masses were mucosa-covered, firm, and did not bleed on touch (A, B). The relationship of the mass with the spheno-ethmoidal recess (*) and the anterior face of the sphenoid (in patient#1) is shown in C–E. (S = septum, m = mass, IT = inferior turbinate, MT = middle turbinate, ST = superior turbinate, * = spheno-ethmoidal recess). Imaging characteristics of the lesions in the two patients (A–E, patient#1, left side; F–K, patient#2, right side). Magnetic resonance imaging (MRI) in patient#1 showed a hypo-intense mass lesion at the choana in T2-weighted protocol (A, B; coronal). In the T1-weighted series with gadolinium (C–E), the mass was seen not to take up the contrast appreciably and had a mottled appearance. Contrast-enhanced computed tomogram images (F, coronal; G, axial) showed the mass in patient#2 also as non-enhancing. Like patient#1, the lesion in this patient too was hypo-intense and had a mottled appearance on T2-weighted MRI (H, coronal; I, parasagittal; J, axial; K, coronal). As evident from the imaging, the masses in both patients were in a close association with the anterior face of the sphenoid sinus and the respective lateral nasal wall, without any evidence of lateral extension or bone remodeling/destruction. The paranasal sinuses were clear.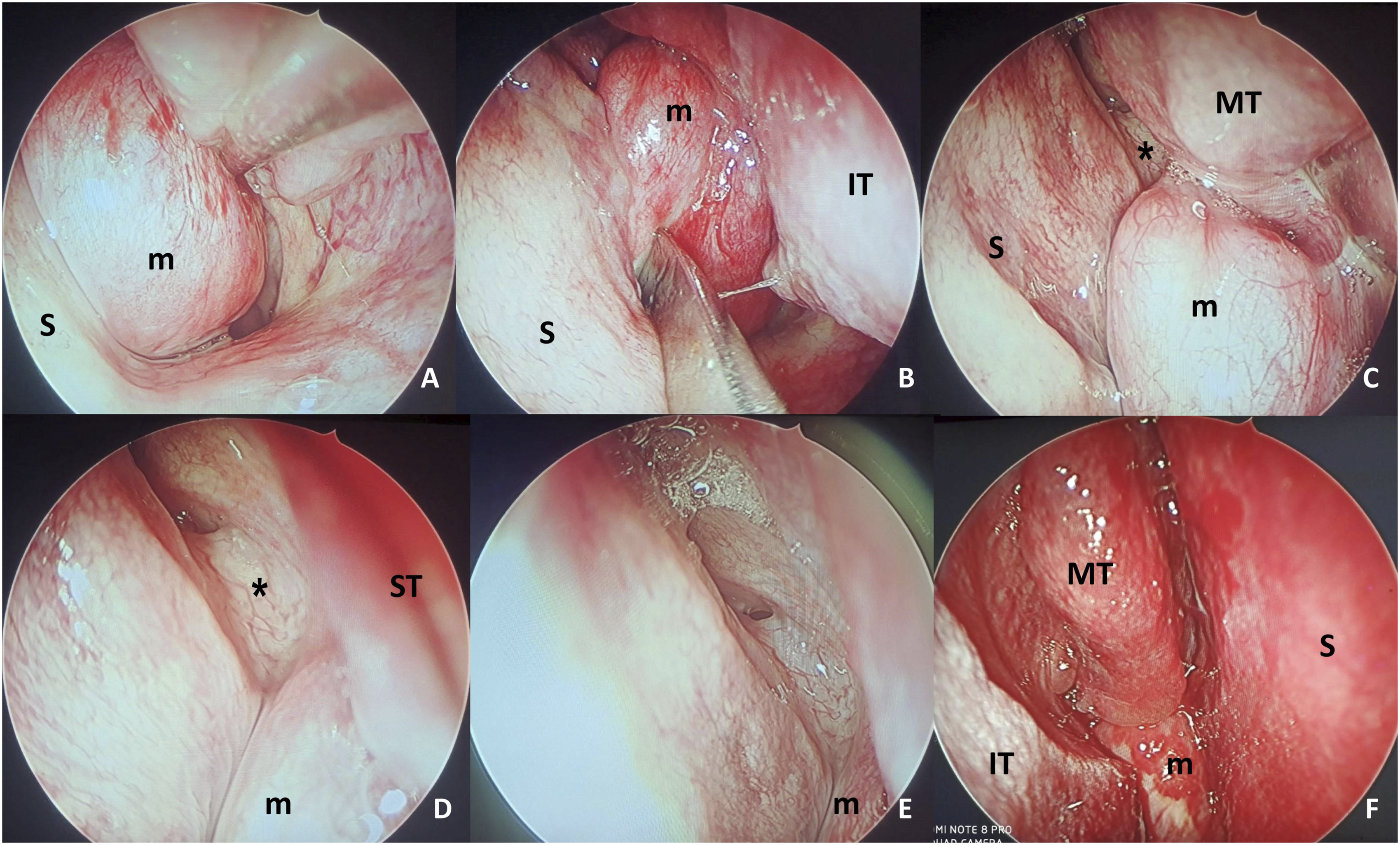
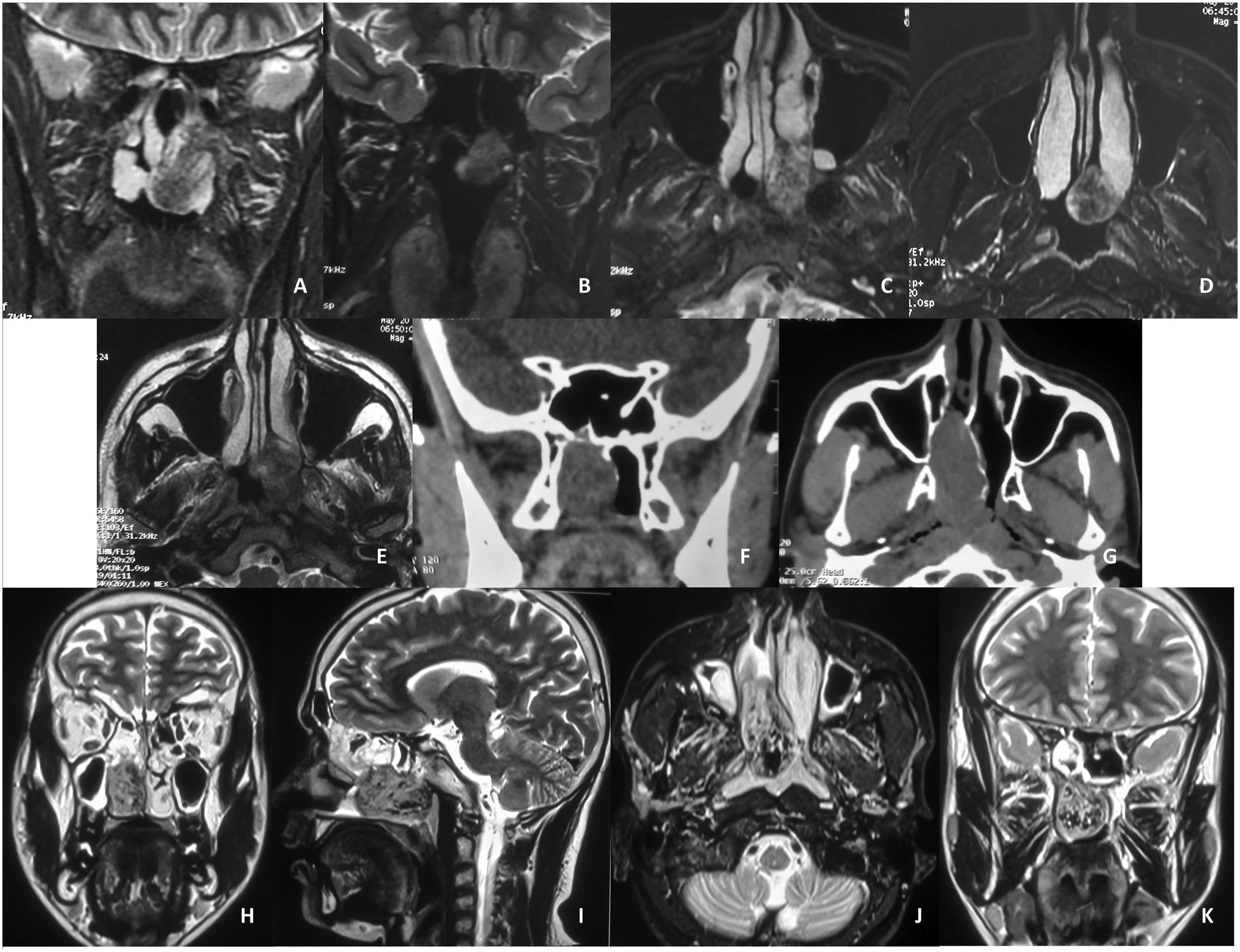
Similar clinical profile and imaging characteristics were encountered in another man, aged 41 years [patient#2], who presented six months later. As evident on imaging, the non-enhancing mass occupied the posterior half of the right nasal cavity (Figure 2). This time, a magnetic resonance angiogram was performed which revealed no tumor blush or prominent vasculature/feeder vessels.
Several differentials were considered, including neoplasms (e.g., minor salivary gland tumors and inverted papilloma), vascular fibrosed nasal polyp, and fibrovascular mass, thereby not ruling out nasopharyngeal angiofibroma (NA). Considering the limited extent of the mass in both the patients, and because their vessel density could not be apprehended, endoscopic excision under general anesthesia was decided without prior incision/punch biopsy.
Following greater palatine canal block and trans-maxillary endoscopic sphenopalatine artery ligation, the mass was separated from its attachment to the anterior face of sphenoid sinus using bipolar cautery in both the patients. In patient#1, the lesion along with the posterior part of inferior turbinate to which it was found attached was resected en masse. In patient#2, the mass was excised from its attachment in the lateral nasal wall posterior to the area of the sphenopalatine foramen. There was no significant intra-operative bleeding.
They are presently under follow-up for more than a year without complications or recurrence.
Histopathology revealed sub-epithelial compressed blood vessels of varying shapes and luminal widths, whose walls were lined by bland endothelial cells without muscular coat (Figure.3). However, the spindle and stellate-shaped stromal fibroblasts having bland vesicular nuclei and eosinophilic cytoplasm were predominant and dense. The abundance of stromal fibroblasts over sub-epithelial capillaries with overlying respiratory epithelium was diagnostic of stroma-predominant NA (the so-called “fibroangioma”). Histopathology from the excised specimen of both masses showed a definite predominance of the stromal components (A, patient#1; B, patient#2). The spindle and stellate-shaped stromal fibroblasts were densely packed in eosinophilic background. The blood vessels that were compressed into varying shapes and luminal widths, with their walls being lined by bland endothelial cells sans muscular coat, were relatively scanty. Only in some areas that were few and scarcely noted, the vessels appeared prominent and dilated (C, D). The abundance of stromal fibroblasts over capillaries suggested stroma-predominant angiofibroma (the so-called “fibroangioma”) (hematoxylin-eosin; x100).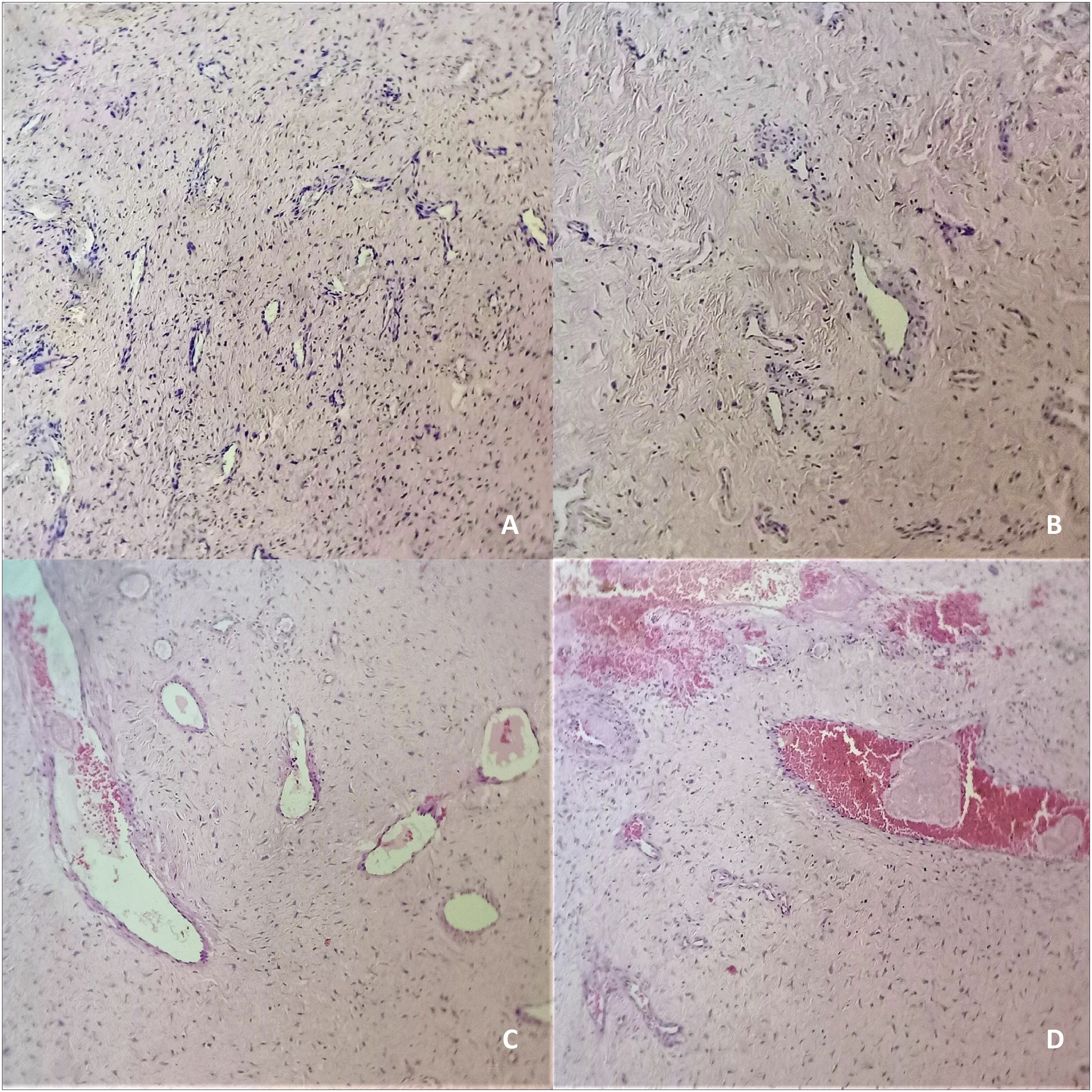
NA is an established clinical entity exclusive to pre-pubertal and adolescent boys. This unique predisposition relates to the hypothesis of the tumor’s responsiveness to pituitary–androgen–estrogen axis secondary to the hormone receptor expressions without a demonstrable endocrinological imbalance.1,2 The presentations in the two patients described, however, were unique on multiple aspects. That they were in their fifth decade at the initial presentation without episodes of epistaxis prior to that was one of them. The presentation of de novo NA in patients beyond their second decade is unusual with very few published reports.1,3 Also, the imaging in none of the patients provided any definitive cue suggestive of NA. There was no or minimal contrast uptake, no evidence of bone erosion or remodeling, absence of the characteristic spread pattern, and the resultant tell-tale radiologic signs (like the Holman-Miller). The only hint noticed on imaging and pre-operative naso-endoscopy, and later confirmed at surgery, favoring NA was the attachment of the mass to the anterior face of sphenoid and the adjacent lateral nasal wall from where it might have derived its vascular supply (posterior septal branch of the sphenopalatine artery). Therefore, from clinico-radiologic perspectives, angiofibroma/fibroangioma was a serious consideration for diagnosis but was never the only differential discussed.
One of the most remarkable features of interest here was the predominance of fibrous stroma over a relatively scanty, compressed vessel population seen on histopathology. This suggests that the lesions were aged.4,5 The patients possibly had been harboring the NA since decades, which was in the process of regression, and somehow became symptomatic only recently. But the absence of contiguous spread and resultant bone remodeling expected from an advancing angiofibroma might counter this assumption, thereby supporting their de novo origin here. However, not all symptomatic NAs, even in late adolescence, are necessarily large having contiguous extensions (typically the early stage lesions). The authors here have taken the liberty of referring this older, fibrous stroma-rich tissue as “fibroangioma” instead of angiofibroma. This nomenclature is backed by the histologically documented spectrum of changes an angiofibroma tissue encounters with time, from vessel-rich to stroma-predominant.4,5 One should be cautious in interpreting the terminology, as many literature studies have often used the term fibroangioma interchangeably with angiofibroma without acknowledging, from histologic perspectives, the continuum the tumor experiences in its composition as it gets older.6-8
The authors’ clinical experience with the two patients demonstrates the natural evolution of an angiofibroma to fibroangioma. Being stroma-predominant, a fibroangioma behaves differently resulting in diagnostic dilemma, with lesser propensity of bleeding, and poor or no contrast uptake. By virtue of its natural regression, it might have limited contiguous spread. On the contrary, it may arise de novo in adulthood. Although it is difficult to prove the origin of a fibroangioma (natural regression or de novo), an isolated choanal mass with poor enhancement in hitherto asymptomatic post-adolescent men having healthy paranasal sinuses should arouse suspicion for an angiofibroma/fibroangioma continuum.
Footnotes
Authors’ Note
The paper was presented at the 50th Annual Conference of the Association of the Otolaryngologists of India, West Bengal Chapter, on January 6–8, 2023, held at Kolkata, India.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The clinical data pertaining to the patient are available with the authors and can be reproduced on request.
Ethical statement
Written informed consent has been obtained from the patient for the publication of this clinic paper. The clinical and surgical principles adopted for the management of the patient complied with the ethical standards of the relevant national and institutional guidelines on human experimentation, as laid down in the Declaration of Helsinki, 1975, as revised in 2013, at Fortaleza, Brazil.