
Abstract
Laser laryngectomy is a minimally invasive surgical technique that offers advantages such as precise and limited resections, magnification of the surgical field by microscopy, and improved patient outcomes. However, it is not without risks, and intraoperative complications have been reported, including cervical-cutaneous emphysema. This case report presents a rare complication of cervical-cutaneous emphysema after laser laryngectomy occurring in a 57-year-old patient with glottic carcinoma. The patient underwent laser cordectomy, and after an uneventful procedure, the patient experienced an intense coughing episode followed by swelling and progressive emphysema. The patient was kept under surveillance in the intensive care unit and received ampicillin sulbactam, protective orotracheal intubation, and voice rest. The patient had a good clinical evolution, and the emphysema resolved within 8–10 days. This case highlights the importance of prompt recognition and management of complications that can arise from laser laryngectomy. Although this technique offers several advantages, it is not risk-free, and intraoperative complications can occur. As such, careful consideration and patient selection are important to minimize the risks and achieve successful outcomes.
Introduction
Advancements in the treatment of laryngeal carcinoma have led to significant improvements in patient outcomes. Minimally invasive surgical techniques have been developed to reduce patient morbidity and improve laryngeal preservation. 1 One such technique is laser laryngectomy, which offers several advantages including precise and limited resections, adequate differentiation of healthy and compromised tissue, magnification of the surgical field by microscopy, functional improvement of patients, reduction of radical surgery, avoidance of tracheostomies or feeding tube placement,1 -3 and the possibility of repeating the procedure in case of recurrence or tumor recurrence. 4 In carefully selected cases, oncological results are similar to open surgery. However, laser laryngectomy is not without risks, and intraoperative complications have been reported, including major complications in 5–13% of cases and minor complications in 7–30% of cases. These complications may include postoperative bleeding, dyspnea, dysphagia, aspiration pneumonia, local infection, and severe bradycardia.1 -3,5 In this report, we present a rare complication of cervical-cutaneous emphysema after laser laryngectomy, occurring in less than 1% of cases.
Case Report
A 57-year-old patient presented with a two-year history of dysphonia, which was initially treated as an allergy, but the symptoms persisted. The patient had a history of myocardial revascularization with two stents and a 20-year history of smoking cessation. On physical examination, an infiltrating tumor lesion was observed on the right vocal cord. Nasofibrolaryngoscopy revealed a lesion extending to the anterior commissure and the upper third of the left cord (Figure 1). Nasofibrolaryngoscopy revealed a tumoral lesion on the right vocal cord that extended to the anterior commissure and upper third of the left cord.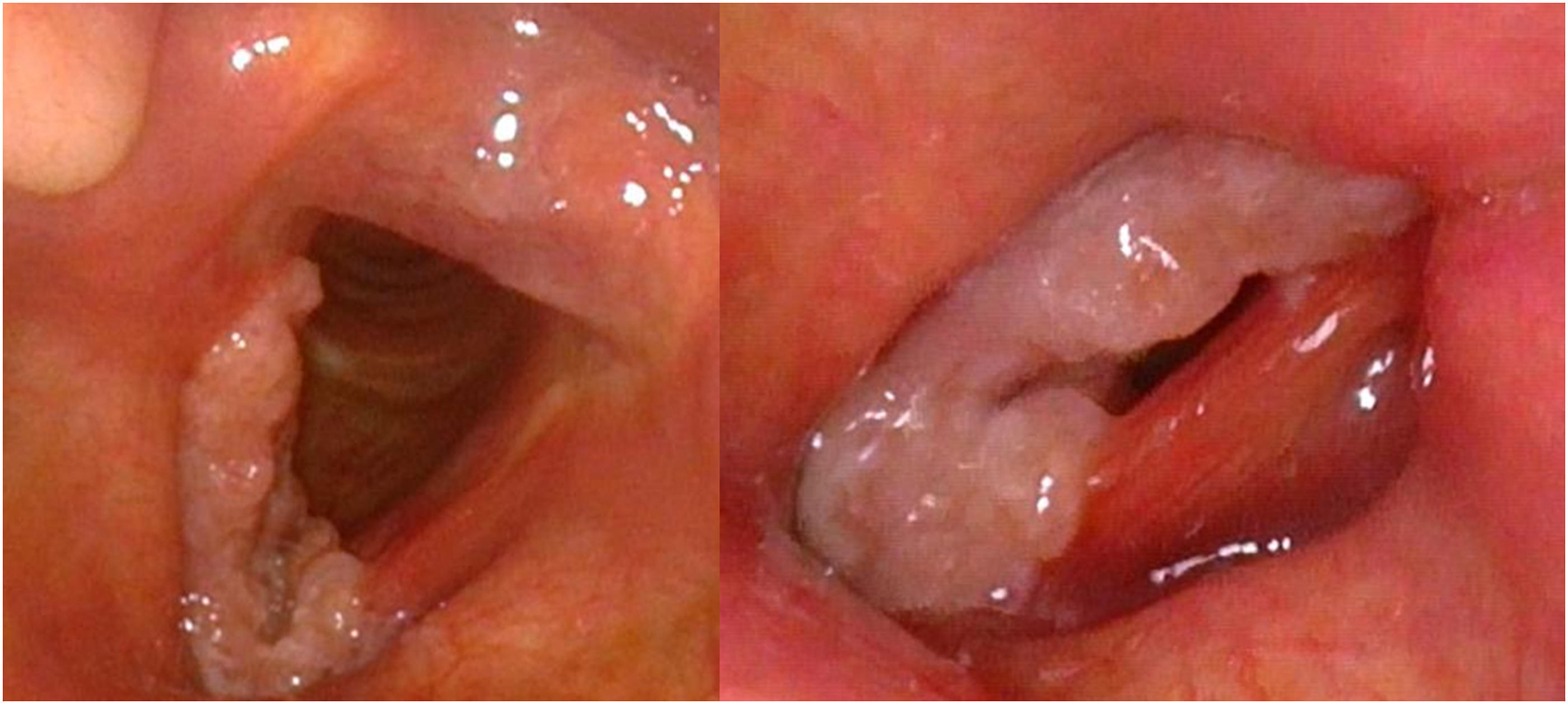
A biopsy confirmed the presence of moderately differentiated infiltrating squamous cell carcinoma. Further imaging studies, including neck CT scan and MRI, showed an infiltrating lesion in the right vocal cord with extension to the anterior commissure, but without any cartilage involvement. Additionally, a PET scan did not reveal any lymph node uptake or distant metastasis.
The patient was diagnosed with T1b N0 M0 glottic carcinoma and underwent a laser cordectomy, with resection of the carcinoma in the right vocal cord and extension towards the anterior commissure and the upper third of the left vocal cord. The procedure was uneventful, and the patient was extubated and transferred to the recovery room. However, the patient subsequently experienced an intense coughing episode, followed by swelling and progressive emphysema (cervical, facial, and chest). Due to the increasing emphysema, a laryngoscopy was performed, which did not reveal any bleeding or other pathological findings. The patient was then sedated and reintubated. A chest X-ray was performed, which showed bilateral supraclavicular subcutaneous emphysema associated with pneumomediastinum, but without pneumothorax.
After the patient experienced emphysema and pneumomediastinum post-surgery, the decision was made to keep the patient under surveillance in the intensive care unit. The patient was administered ampicillin sulbactam 3 gr IV every 6 hours for 7 days and had a protective orotracheal intubation for 24 hours. Following this, the patient was extubated and instructed to have absolute voice rest with the head of the bed raised. The patient had a good clinical evolution, was hemodynamically stable, and did not experience dyspnea. X-rays were performed for control and the patient had a clinical follow-up with progressive improvement of emphysema. Finally, the patient was discharged without complications (Figure 2). (a) Chest X-ray of the patient, which displays bilateral supraclavicular subcutaneous emphysema associated with pneumomediastinum but without pneumothorax. (b) Patient with protective intubation 24 hours after the surgical procedure, bilateral cervical, and facial emphysema. (c) Patient with complete resolution of emphysema 10 days after surgery.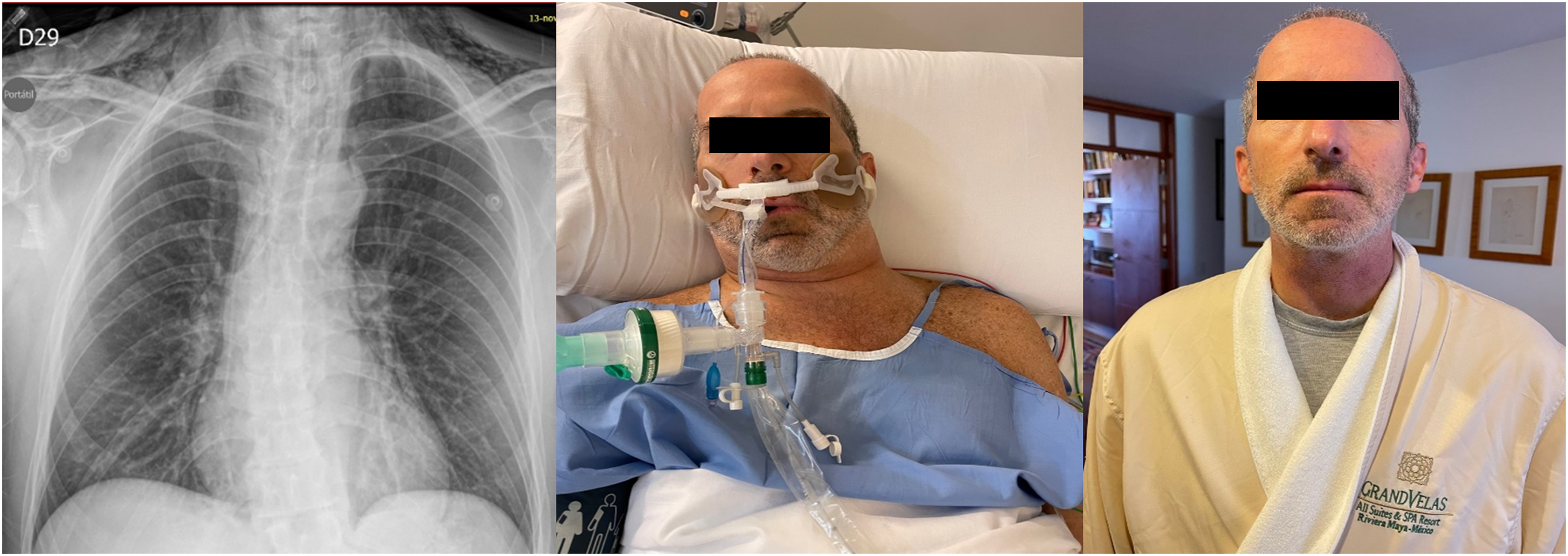
The pathology report confirmed infiltrating squamous cell carcinoma, moderately differentiated and keratinizing. The tumor was negative for p16 and positive for PD-L1. The patient received treatment with radiotherapy, which consisted of 30 sessions of IMRT at 6000 cGy. During follow-up, the patient showed complete resolution of the emphysema, and symptomatic management of the postoperative cough was provided
Discussion
The use of laser in laryngeal tumor surgery has revolutionized the management of these tumors, providing a less invasive option with improved functional outcomes and faster recovery time for patients.1 -6 However, complications such as subcutaneous emphysema can occur, 7 even in small tumor resections. In our case, the development of subcutaneous emphysema was likely due to the skeletonization of laryngeal cartilage and the cricothyroid membrane during the procedure, 6 combined with increased pressure from coughing. Protective intubation was used to manage the progressive emphysema and antitussives and voice rest were also employed. The patient recovered without complications, and the emphysema resolved within 8–10 days. This case highlights the importance of prompt recognition and management of complications that can arise from this procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This case report was carried out within the ethical principles for medical research in humans according to the Declaration of Helsinki–59th General Assembly, Seoul, Korea, October 2008. The national regulations of the Ministry of Health and Social Protection of Colombia Resolution 8430 of 1993 regarding Chapter I “Of the ethical aspects of research in human beings” were taken into account. This research is classified within the Research category without risk, and with the informed consent of the patient.