
Abstract
Objectives
While surgeries to correct the anatomical malformations that cause nasal airway obstruction (NAO) are generally successful, the outcomes of such procedures are often unsatisfactory. The aim of the present study was to assess the value of opening the middle meatus in patients with NAO.
Methods
Thirty-four patients with nasal obstruction due to nasal septal deviation were included in this study. After randomization, the middle meatus was either opened or not opened during septoplasty. The patients were evaluated through pre- and postoperative rhinomanometry and acoustic rhinometry. The Visual Analog Scale (VAS) scores of subjective symptoms along with responses to the 20-item Sinonasal Outcome Test (SNOT-20) were obtained before surgery and three months after surgery.
Results
The VAS scores and SNOT-20 responses improved significantly in both groups after surgery. The effective treatment rate based on the nasal congestion score (NCS) was 64.7% in the single group (septoplasty alone) and 100% in the combined group (septoplasty in conjunction with opening the middle meatus), and the difference was statistically significant (P = .018). In both groups, surgery significantly improved nasal flow, resistance, minimal cross-sectional area, cross-sectional area 6 cm (CA6) from the anterior nostril and nasal volume. Nasal volume and CA6 after surgery were statistically different between the 2 groups (P = .004 and .019, respectively).
Conclusions
Opening the middle meatus may further improve the subjective perception of patency on the basis of septoplasty.
Introduction
Nasal congestion is a subjective complaint defined as discomfort manifested as a feeling of insufficient airflow through the nose. Nasal septal deviation and turbinate hypertrophy are common anatomical causes of nasal airway obstruction (NAO). 1,2 Although surgeries to correct the anatomical malformations that cause NAO are generally successful, the outcomes of many of such procedures, especially the long-term results, are not satisfactory. 3 -6 Most surgeries are aimed at improving nasal resistance. However, the main mechanism of nasal airflow sensation is not airflow resistance but mucosal cooling by inspired air. 7 -11 This may explain the unsatisfactory postoperative outcomes to some extent.
The mucosal cooling mechanism provides an approach for clinicians to solve nasal congestion. Computational fluid dynamics (CFD) studies have shown that the perception of nasal patency is related to the distribution of nasal airflow and mucosal cooling in NAO. 12 -17 Some studies have also emphasized the positive effect of airflow in the middle of the nasal airway on the perception of nasal patency. 12 -14 Computational fluid dynamics studies have confirmed that sinus surgery increases airflow in the middle of the nasal cavity, 18 -21 and Xiong et al found that functional endoscopic surgery increased flux through the area connecting the middle meatus and surgically opened ethmoid sinuses by more than 13%. 18 Nasal and sinus surgery has also been used to improve subjective symptoms in patients with obstructive sleep apnea (OSA), and symmetric opening of the sinuses was found to reduce nasal resistance, increase nasal ventilation, and alleviate upper airway obstruction. 22,23
To our knowledge, few clinical studies have been conducted on the impact of opening the middle meatus on subjective nasal symptoms and objective indicators. We hypothesized that opening the middle meatus could improve the perception of nasal patency in NAO by modifying the intranasal airflow distribution. Through a randomized controlled study, we analyzed the effect of opening the middle meatus in patients with NAO. The main objective was to determine whether opening the middle meatus can (1) improve perception of nasal patency and (2) improve objective indicators of nasal ventilation.
Patients and Methods
Patients and Study Design
A prospective, controlled, randomized study was conducted monocentrically in the Department of Otorhinolaryngology, Head and Neck Surgery of the Beijing TongRen Hospital. The study was approved by the medical ethics committee and written informed consent was obtained from each patient before participation. Patients with nasal septal deviation who complained of nasal congestion met the following inclusion criteria between November 2018 and October 2020 were included in the study. The inclusion criteria were a visual analog scale (VAS) score for nasal congestion greater than 3 points and concomitant with bilateral asymptomatic cysts of ethmoid sinus and/or maxillary sinus with diameter less than 1.5 cm (e.g., Figure S1). The exclusion criteria were any kind of previous surgeries of the nose, turbinate, or sinuses; nasal polyps; and age less than 18 years or older than 65 years.
The first study group received a regular septoplasty with lateral displacement and fixation of the inferior turbinate, and followed up for unresected sinus cysts (“single” group). In addition to the above procedure, patients in the second group received bilateral partial ethmoidectomy and/or maxillary antrostomy to resect sinus cysts along with medial displacement and fixation of the middle turbinate, as previously described (“combined” group). 22
According to pre-experimental data, the effective treatment rates (determined as a decrease of more than 3 points in the nasal congestion VAS score after treatment) for the single and combined groups were 62.5% and 100%, respectively. Setting α = .05 and β = .15, the sample size was determined as 32 cases using PASS 15.0. Thirty-six patients meeting the inclusion criteria were recruited, but two cases were dropped due to inability to follow-up on time. Finally, a total of 34 subjects were randomized into single and combined groups. Randomization was carried out in sets of two consecutive patients (that is, in a ratio of 1:1) according to a computer generated randomization code.
Two examinations were completed for each patient. All participants provided preoperative VAS scores of subjective nasal symptoms and responses to the 20-item Sinonasal Outcome Test (SNOT-20). 24 Rhinomanometry and acoustic rhinometry were also performed before surgery. The second and final examination was performed three months after the operation. Each of the study participants reported the VAS scores for subjective nasal symptoms and completed SNOT-20 for the second time. Rhinomanometry and acoustic rhinometry were also repeated.
Surgical Procedures
The procedures were performed by the same senior rhinology specialist under general anesthesia, reducing the risk of inconsistency or bias for a particular procedure. Septoplasty with resection of three high-tension lines could preserve the maximal supporting framework of cartilage and the skeletal framework and avoid subsequent collapse by releasing three key stress lines. Lateral displacement and fixation of the inferior turbinate involved the following steps: A blunt dissector was used to push the anterior/inferior extremity of the inferior turbinate through the common nasal meatus, fracture the root of the inferior turbinate, and then displace it to the lateral nasal wall. Bilateral partial ethmoidectomy and maxillary antrostomy included removal of the uncinate process and ethmoidal bulla and opening of the anterior and/or posterior ethmoidal sinuses and/or maxillary sinus to resect sinus cysts. The medial displacement and fixation of the middle turbinate was performed by medially removing it from its root with a blunt dissector to widen the middle meatus. 22
Postoperative Medical Treatment
In both groups, nasal lavage with normal saline solution and intranasal steroids were used for three months after surgery. Antihistamine and/or leukotriene antagonists were used when the patient was diagnosed with allergic rhinitis and the related symptoms could not be controlled by intranasal steroids alone.
Clinical Assessment
Visual analog scale scores for subjective symptoms (nasal congestion, headache, hyposmia, postnasal discharge, runny nose, and general symptoms) were reported on a scale of 0–10 points. The primary endpoint was the effective treatment rate based on the nasal congestion score (NCS) three months after the operation in this study. Sinus-specific quality of life was assessed using SNOT-20. Rhinomanometry and acoustic rhinometry were performed using a rhinomanometer and acoustic rhinometer (GM instruments, The UK). The above four assessments were performed in all patients before and 3 months after the operation. The sinuses were examined by computed tomography (Philips Health Care, Best, The Netherlands) preoperatively. Eosinophils of nasal secretion and serum total IgE were evaluated using an Immuno-Cap Phadiatop (Pharmacia, Uppsala, Sweden) before surgery.
Statistical Analysis
Statistical analysis was performed using SPSS 19.0 (IBM Corp, Armonk, NY, USA), and graphs were created using GraphPad Prism 9.0 (GraphPad, La Jolla, CA, USA). Measurement data that corresponded to the normal distribution were reported as mean and standard deviation, and abnormally distributed data were reported as median and interquartile range (IQR). Count data were reported as frequency and percentage. Paired t tests or related nonparametric sample tests were used for intragroup variations. Independent sample t-tests or nonparametric tests were used for intergroup variations. Fisher’s exact test was used for frequencies and percentages. All statistical tests were two-sided and a level of .05 was considered statistically significant.
Results
Demographics
Demographic and General Clinical Data of the Patients in the two Groups.
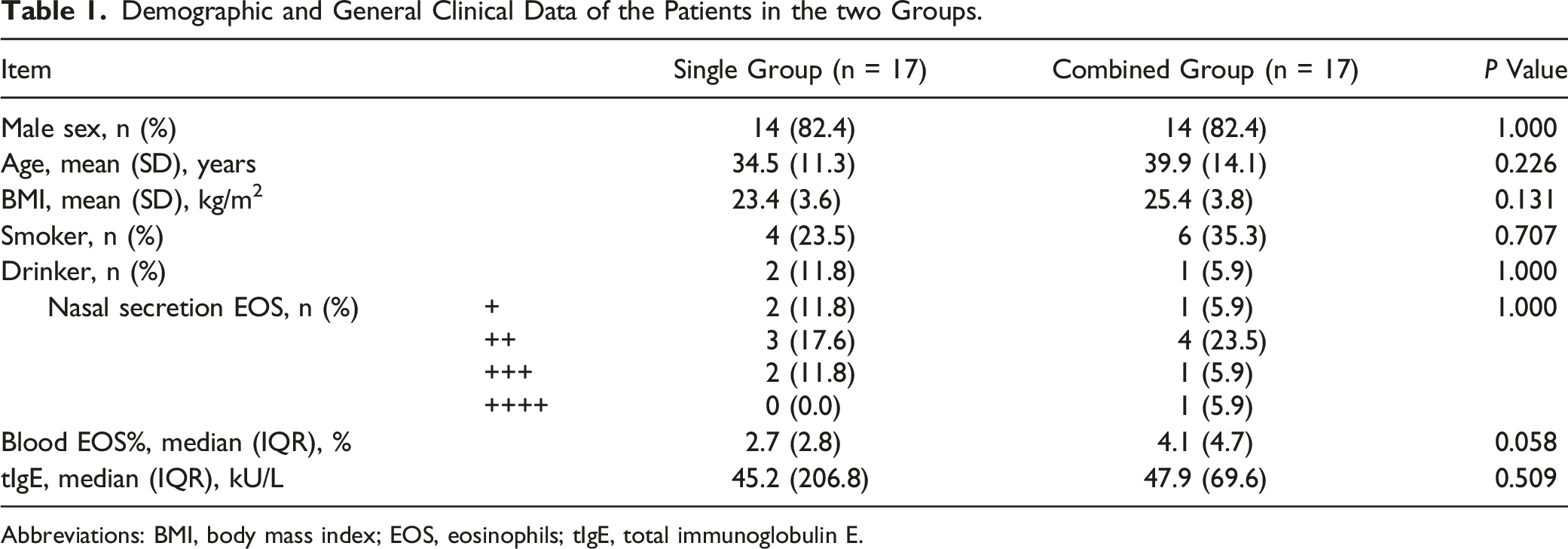
Abbreviations: BMI, body mass index; EOS, eosinophils; tIgE, total immunoglobulin E.
Visual Analog Scale Scores for Subjective Nasal Symptoms and SNOT-20 Scores
Comparison of Pre-and Postoperative VAS, SNOT-20 Scores, Rhinomanometry and Acoustic Rhinometry Values Within and Between Groups.
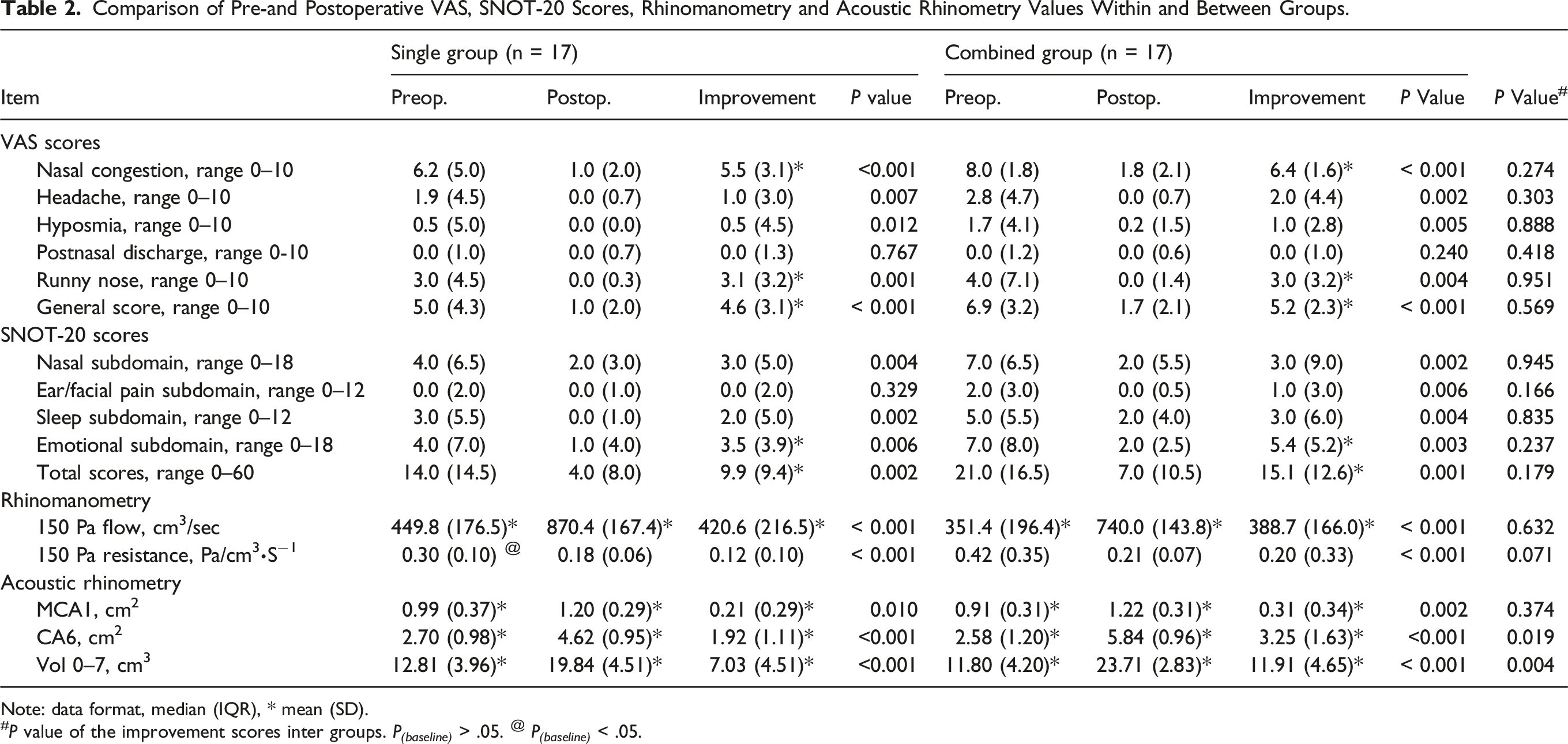
Note: data format, median (IQR), * mean (SD).
# P value of the improvement scores inter groups. P (baseline) > .05. @ P (baseline) < .05.
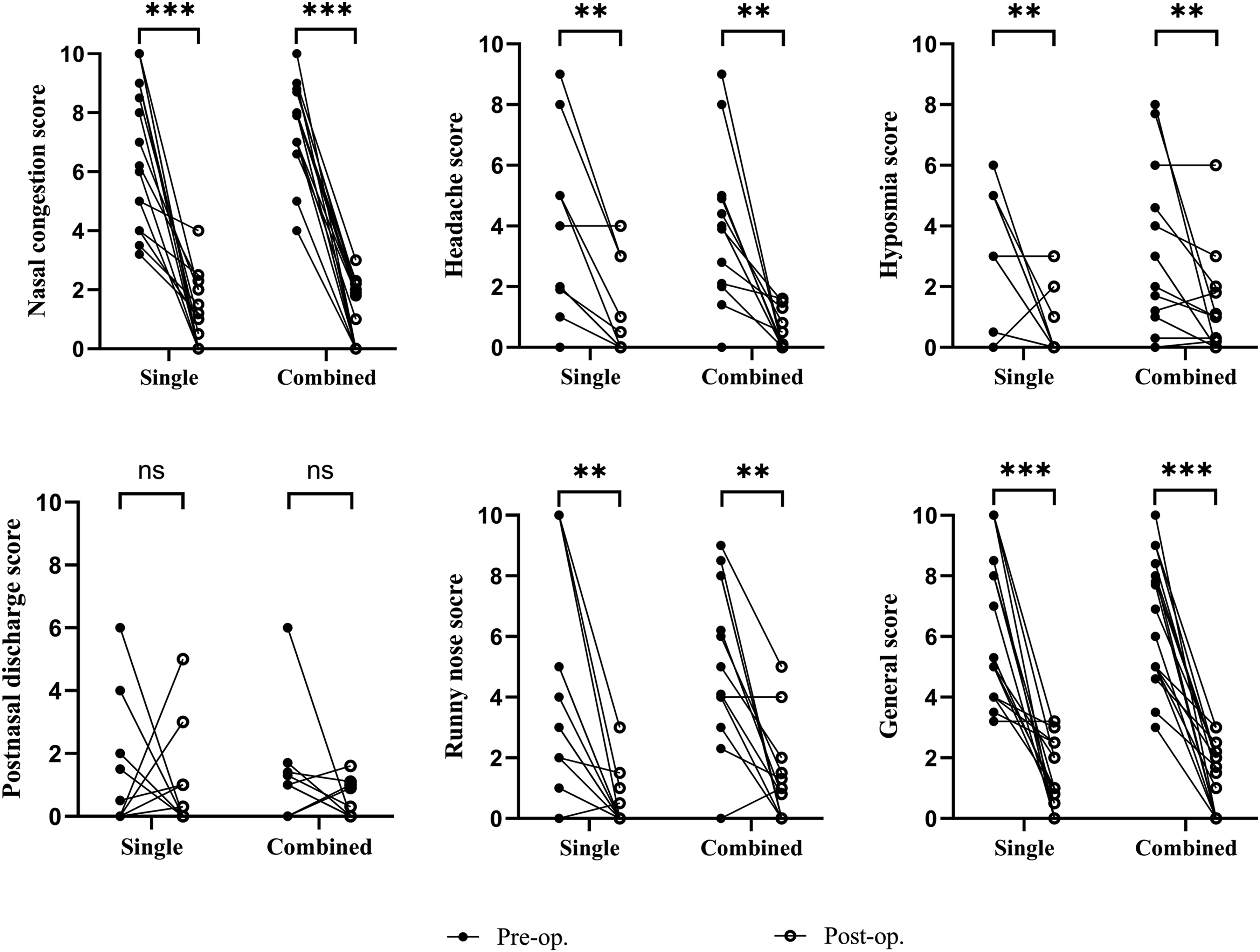
Comparison of the pre- and postoperative differences in various VAS scores of subjective symptoms in each group. ns, no significant, **P < .01, ***P < .001.
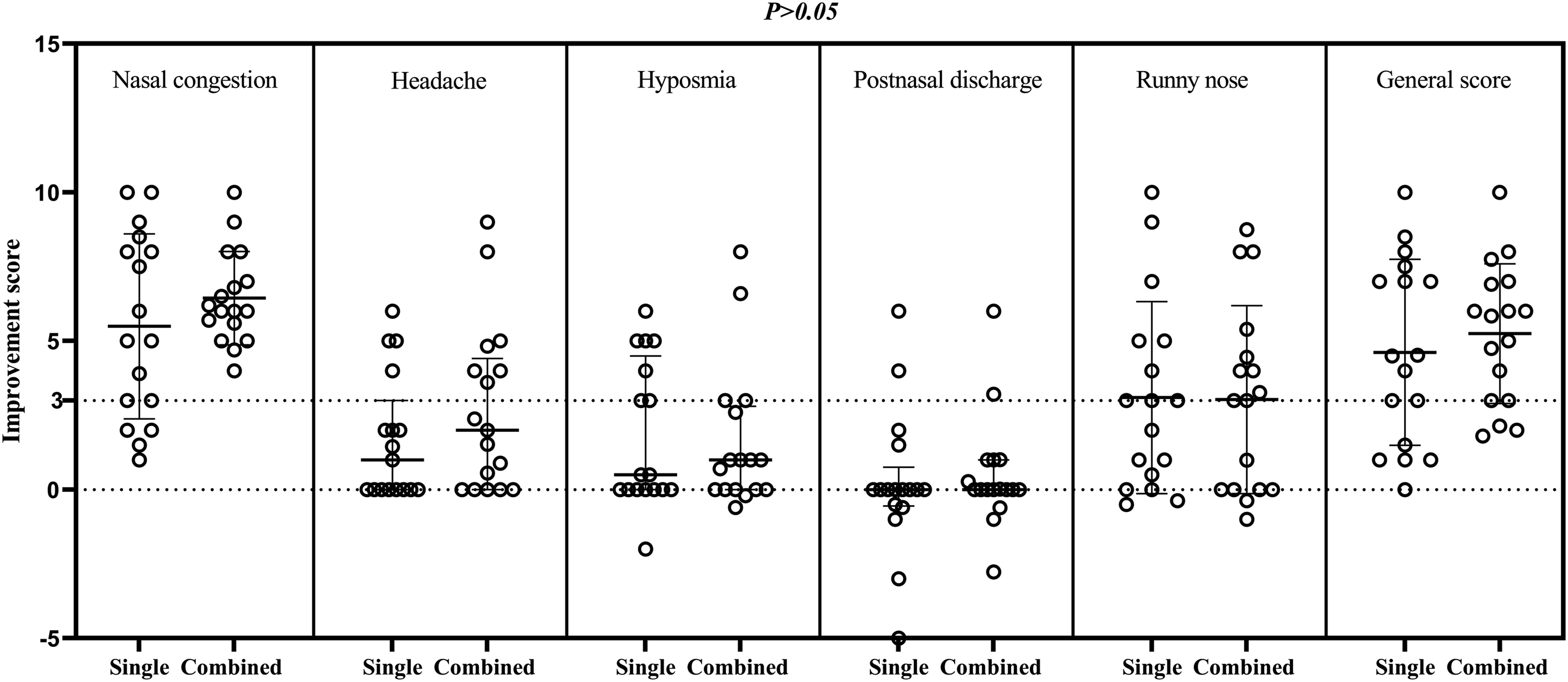
Comparison of the improvements between the pre- and postoperative VAS scores of various subjective symptoms between groups.
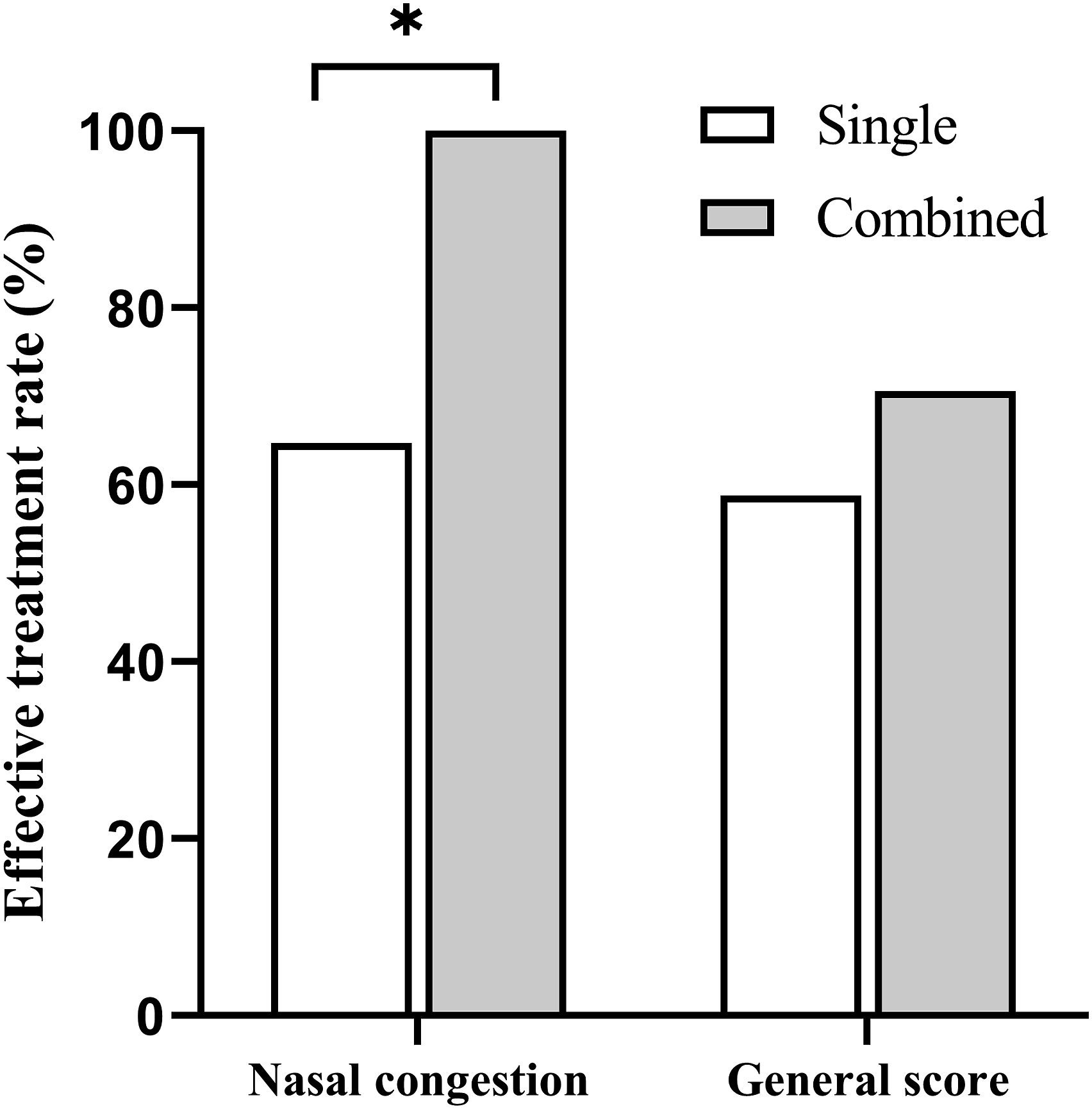
Comparison of the effective treatment rates between groups based on the VAS scores of various subjective symptoms, *P < .05.
There were no significant differences in the baseline subdomain and the total SNOT-20 scores between the groups. In the single group, the median total scores decreased from 14.0 points preoperatively to 4.0 points postoperatively, while it declined from 21.0 points to 7.0 points in the combined group. The difference before and after the operation was statistically significant (P < .01) for both groups. The mean improvement in the score after surgery was 9.9 in the single group and 15.1 in the combined group, and this difference was not significant (P = .179; Table 2 and Figure 4). The same result was obtained for most subdomain scores. All pre- and postoperative differences in subdomain scores were statistically significant (P < .01) except for ear/facial pain in the single group (P = .329). Meanwhile, no statistically significant differences were found in the improvement scores between the two groups (Table 2). Comparison of the pre-and postoperative differences in SNOT-20 scores within each group and improvement between the two groups, **P < .01.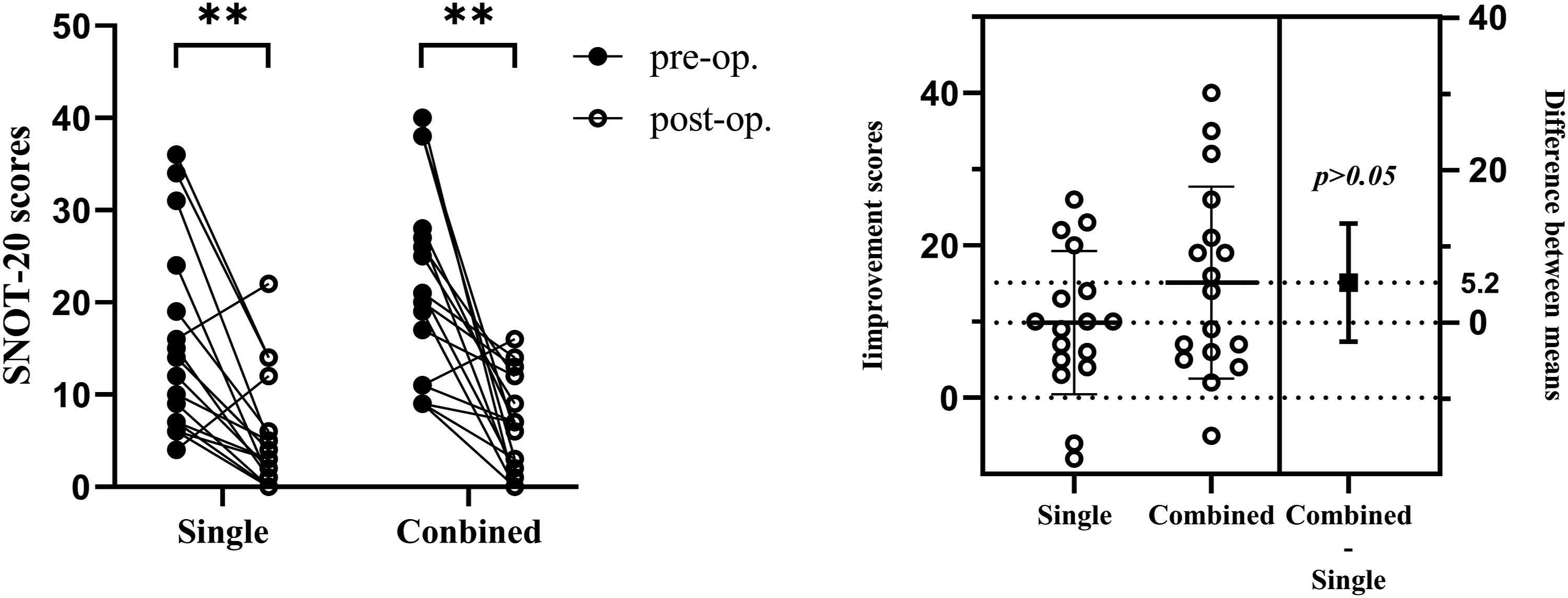
Rhinomanometry and Acoustic Rhinometry
The mean inspiratory flow of 150 Pa was 449.8 cm3/s preoperatively versus 870.4 cm3/s postoperatively in the single group, and 351.4 cm3/s preoperatively versus 740.0 cm3/s postoperatively in the combined group. There were no significant differences in baseline inspiratory flow between the groups. The same result was detected for nasal resistance, although the baseline nasal resistance was significantly different between the groups. The median 150-Pa nasal resistance was .30 Pa/cm3·S−1 preoperatively versus .18 Pa/cm3·S1 postoperatively in the single group, and .42 Pa/cm3·S−1 preoperatively versus and .21 Pa/cm3·S−1 postoperatively in the combined group. The pre- and postoperative results above were significantly different in both groups (P < .001), while the improvement values did not differ significantly between the two groups (Table 2 and Figure 5). Comparison of the pre- and postoperative differences in the rhinomanometry and acoustic rhinometry values within each group and improvement between the two groups, **P < .01, ***P < .001.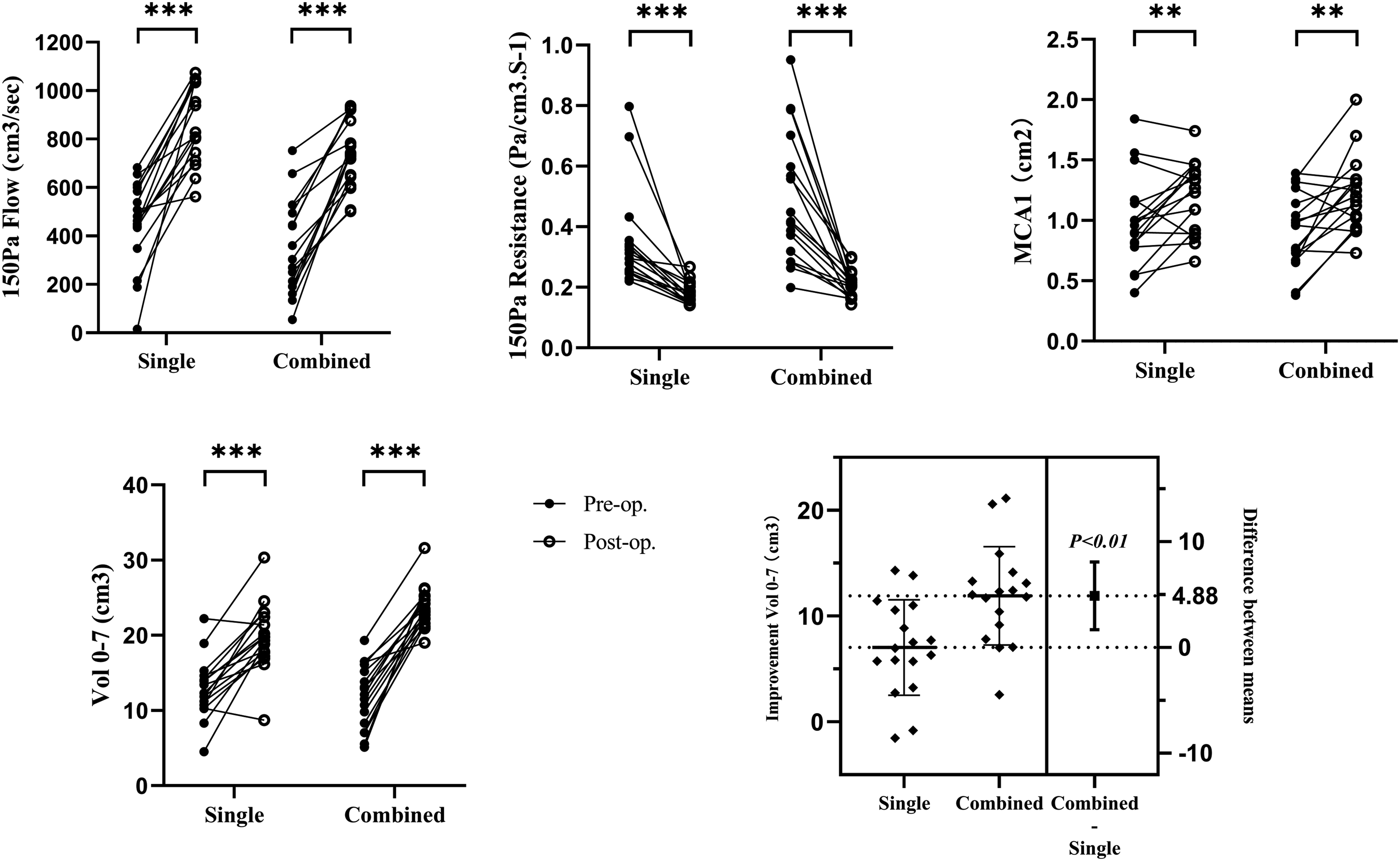
In the single group, the mean minimum cross-sectional area 1 (MCA1) was .99 cm2 preoperatively versus 1.20 cm2 postoperatively, and the mean nasal volume (Vol 0–7) increased from 12.81 cm3 preoperatively to 19.84 cm3 postoperatively. In the combined group, MCA1 was 0.91 cm2 preoperatively versus 1.22 cm2 postoperatively, and Vol 0-7 increased from 11.80 cm3 preoperatively to 23.71 cm3 postoperatively. The baseline values of MCA1 and Vol 0-7 were not significantly different between the groups. The pre- and postoperative results were significantly different in both groups (P < .05). The improvement in MCA1 did not differ significantly between the two groups, while the improvement in Vol 0–7 was significantly different between the two groups (P = .004; Table 2 and Figure 5).
The mean cross-sectional area 6 cm (CA6) from the anterior nostril was 2.70 cm2 preoperatively versus 4.62 cm2 postoperatively in the single group and 2.58 cm2 preoperatively versus 5.84 cm2 postoperatively in the combined group. There were no significant differences in baseline CA6 between the groups. The pre- and postoperative results were significantly different in both groups (P < .001), and the improvement in CA6 was significantly different between the two groups (P = .019; Table 2).
Some additional data are included in the supplementary material (Table S2 and Figure S2).
Discussion
Nasal Airway Obstruction is a common affliction, 1 and septoplasty and turbinoplasty are the most common methods to improve subjective nasal breathing. 2,25,26 Although the effectiveness of these procedures remains controversial in the literature, 27,28 our results support their positive impact on functional nasal breathing. The growing evidence suggests that the primary physiological mechanism of nasal airflow sensation is not airflow resistance but activation of trigeminal cool thermoreceptors, specifically TRPM8, by nasal mucosal cooling. 7,9,11,16 Subjective nasal patency is correlated with the distribution of intranasal airflow related to mucosal cooling. 13,14 Septoplasty is believed to reduce nasal resistance and alter the nasal airflow distribution to improve perception of nasal patency. 15,29
In this study, septoplasty significantly improved postoperative VAS scores for all nasal symptoms except posterior rhinorrhea in the single and combined groups. These improved symptoms included nasal congestion, headache, anosmia, and runny nose. Thus, both procedures are effective in alleviating nasal symptoms. Although VAS scores after surgery did not differ significantly between the two groups, the effective treatment rate based on NCS (defined as a decrease of more than 3 points in the NCS after surgery) was significantly higher in the combined group than in the single group. This suggests that opening the middle meatus may improve the perception of nasal patency. 20-item Sinonasal Outcome Test scores to assess quality of life revealed similar results. Thus, both procedures improved the SNOT-20 scores of patients with equivalent effects.
The results indicate that opening the middle meatus can improve the perception of nasal patency, possibly due to increased airflow and the promotion of mucosal cooling in the middle of the nasal cavity. This is consistent with previous CFD studies on nasal airflow. For example, Zhao et al emphasized the importance of airflow in the middle nasal meatus and found that increased airflow through the middle meatus compared to the inferior meatus was correlated with better patency ratings in healthy adults. 14 Casey et al reported that compared to healthy patients, NAO patients had significantly reduced middle airflow, and subjective nasal patency had no correlation with inferior and superior airflows, but a high correlation with middle airflow. 13 Anterior septal deviations tend to negatively affect airflow by reducing middle airflow and reducing mucosal cooling in some patients with NAO. The aerodynamic characteristics of nasal airflow might be revised after septoplasty in patients with NAO. 16 Ozlugedik et al found that airflow through the middle meatus increased profoundly after removal of the lateral half of the concha bullosa, confirming that functional endoscopic sinus surgery to widen the middle meatus influences the pathological process by increasing the aeration of the middle meatus. 15 The remodeling of the airway after sinus surgery significantly changes the airflow distribution, 19 -21 and airflow through the area connecting the middle meatus and the surgically opened ethmoid sinuses increased by more than 13% after sinus surgery. 18 In previous studies, our team had also found that nasal and sinus surgery can alter airflow patterns, increase airflow volume in both the middle meatus and common meatus, and improve subjective symptoms, including nasal obstruction. 23 The present study further verified that opening the middle meatus can improve the perception of patency by altering the airflow distribution in the nasal cavity. Moreover, some studies have suggested that subjective symptoms of OSA patients improve after sinus surgery. 22,23
In this study, objective indicators of nasal airflow and resistance (based on rhinomanometry) along with MCA, CA6 and nasal volume (based on acoustic rhinometry) improved significantly after surgery in both the single and combined groups. As expected, CA6 located in the middle meatus of the coronal plane and nasal volume increased more after surgery in the combined group than in the single group. The CA6 of middle meatus area increased by about 1.33 cm2 and the nasal volume of middle meatus area increased by about 4.88 cm3 after surgery in the combined group. Numerical simulation showed that nasal resistance in the area within 3 cm from the nostril accounts for 52.6% to 78.3% of total nasal airway resistance, 30 and their results agree with an earlier study based on a “head-out” body plethysmograph technique, which found that two-thirds of total nasal resistance can be attributed to the nasal valve region. 31 The narrowest part of the nasal cavity is usually within a distance of 3 cm from the nares, and two minima have been described in this region. 32 After removal of obstructing factors in the nasal valve area by septoplasty, nasal resistance was alleviated in most cases. 15,33,34 Since opening the middle meatus does not involve the nasal valve area, there were no significant differences in improvements in airflow, nasal resistance, and MCA between the two groups in our study. However, it is difficult for patients with internal valve stenosis, which is frequent in Caucasians, with deviated and crooked nose, to improve nasal airflow through surgery of nasal cavity alone, such as septoplasty or inferior turbinate surgery. In such cases, surgery on the dorsum, a surgical technique reported by Bracaglia et al is necessary to improve nasal airflow. 35
The increase in CA6 and nasal volume and the resulting change in intranasal airflow distribution after opening the middle meatus may improve the perception of patency in patients with NAO. Furthermore, the increase in nasal volume after sinus surgery may also improve quality of life in patients with OSA, 22,23 consistent with other studies on the effects of sinus surgery in patients with OSA. 36,37 Due to possible side effects and complications of sinus surgery, 38 -40 opening the middle meatus may be more suitable for patients with NAO with OSA. For patients with NAO only, the decision to open the middle meatus should be made individually according to clinical characteristics. More research is required to confirm whether opening the middle meatus can improve sleep indicators in OSA patients and understand the effects of continuous positive airway pressure treatment.
Our study has the following limitations. First, the follow-up period was relatively short and longer term follow-up is needed to confirm the outcomes. Second, there is currently no uniform standard for the minimal clinically important difference (MCID) of the NCS score; Clinical research is needed to further determine the MCID value. Finally, it is necessary to expand the sample size to improve the power of the study.
Conclusions
The sensation of nasal breathing is affected by multiple factors; it is related to but not solely dependent on the dimensions, resistance, and nasal airflow of the nasal airways. In general, increased nasal airflow tends to correspond to a sensation of better nasal breathing. However, nasal breathing sensation also depends on factors such as intranasal airflow distribution and mucosal cooling. Opening the middle meatus may further improve the subjective perception of patency on the basis of septoplasty.
Supplemental Material
Supplemental Material - Value of Opening the Middle Meatus in Patients With Nasal Airway Obstruction
Supplemental Material for Value of Opening the Middle Meatus in Patients With Nasal Airway Obstruction by Hongzheng Wei, Lianqi Wan, Yuan Zhang, Yanru Li, Wen Xu, Yunchuan Li, and Demin Han in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We acknowledge the reviewers for their helpful comments on this article.
Author Contribution
Hongzheng Wei: contributed to study design, acquisition of data, analysis and interpretation of data, and drafting of the manuscript; Lianqi Wan: contributed to acquisition of the data and picture processing; Yuan Zhang: contributed to acquisition of the data and interpretation of data; Yanru Li: contributed to interpretation of data and revision of the manuscript; Wen Xu: contributed to study design and revision of the manuscript; Yunchuan Li: contributed to study design and interpretation of data; Demin Han: contributed to study design and interpretation of the data and revision of the manuscript.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the medical ethics committee of Beijing Tongren Hospital.
Informed Consent
Written informed consent was obtained from each patient before participation.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.