
Abstract
Objectives
Skin quality plays a major role in aesthetics, particularly in determining the success of rhinoplasty. Efficient preoperative estimation of nasal skin thickness can improve postoperative results and patient satisfaction. This study aimed to report on the relationship between nasal skin thickness and body mass index (BMI) as a possible tool to measure skin thickness preoperatively among rhinoplasty patients.
Methods
This prospective cross-sectional study targeted patients who visited a rhinoplasty clinic at King Abdul-Aziz University Hospital, Riyadh, Saudi Arabia, between January 2021 and November 2021, and agreed to participate in the study. Data on age, sex, height, weight, and Fitzpatrick skin types were collected. The participant visited the radiology department and underwent ultrasound nasal skin thickness measurement for the five different nasal points.
Results
The study included 43 participants (16 males and 27 females). The average skin thickness of the supratip area and the tip was significantly higher in males than in females (P < 0.05). The average BMI of the participants was 25.8 ± 5.26 Kg/m2. Participants with a normal BMI or less represented 50% of the study sample, whereas overweight and obese represented one-quarter (27.9%) and one-fifth (21%), respectively.
Conclusion
BMI was not associated with nasal skin thickness. Differences in nasal skin thickness were found between the sexes.
Introduction
The skin is the most obvious organ in the human body, with essential protective and regulatory functions. 1 In addition to its function, skin quality plays a major role in aesthetics, specifically in determining rhinoplasty success. Nasal skin quality consists of dermal thickness and number of pilosebaceous units. 2 It varies in thickness along the length of the nose. The rhinion area is the thinnest and thickens caudally in the supratip region. The skin covering the cephalic portion of the nose have little subcutaneous fat and sebaceous glands. Conversely, more subcutaneous tissue and sebaceous glands were found at the nasal tip. 3 In rhinoplasty, patients with thin nasal skin can be challenging because even the slightest irregularities of the reconstructed osseocartilaginous framework can be visible postoperatively. However, thick skin is rich in sebaceous glands and tends not to show a concrete change in their tip after surgery. Surgeons commonly assess skin quality by visual inspection; as a result, subjective measurement variability without validated tools can produce inaccurate preoperative planning.
Efficient preoperative estimation of nasal skin thickness can improve postoperative results and patient satisfaction. Reportedly, sex, age, ethnicity, and nutritional status affect facial soft tissue thickness.4,5 Simultaneously, body mass index (BMI) has been found to play a major role in influencing its thickness.6,7 Various methods have been suggested for measuring nasal and facial soft tissue thickness. For instance, visual examination, palpation, and radiological studies such as ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI).8-11 Nevertheless, there is no standard measure to evaluate nasal thickness. Preoperative ultrasound has been used by Kosins et al. to measure nasal STE thickness in patients undergoing rhinoplasty. 8 CT scans have been used in various populations, such as Korean, Caucasian, Saudi, and diverse races.9-11 Additionally, Ozkul et al. introduced a practical noninvasive method for calculating nasal skin thickness using a Castroviejo Caliper instrument to measure both the nasal dorsum and alar thickness. 2
This study aimed to report the relationship between nasal skin thickness and BMI) as a possible tool to measure skin thickness preoperatively among rhinoplasty patients.
Patients and Methods
The study was a prospective cross-sectional study that targeted patients who visited a rhinoplasty clinic seeking rhinoplasty at King Abdul-Aziz University Hospital (KAUH) Riyadh, Saudi Arabia, between January 2021 and November 2021. KAUH is a teaching and referral hospital for all otolaryngology subspecialties, including facial plastic surgery in Riyadh, and provides health services to Saudi citizens and residents. This research was approved by the Institutional Review Board of the research committee of at college of medicine at king Saud University program with IRB registration number: E-21-6530. Informed consent was obtained from the patients involved in this study. Patients with previous rhinoplasty surgery, other sinonasal surgeries, or congenital nasal deformities were excluded from the study. Age, sex, and Fitzpatrick skin type were collected from the patient history and physical examination. Height was measured using a metric stadiometer and weight was measured using standardized medical measurements. BMI was calculated using the following formula: BMI = body mass divided by the square of body height and is expressed in units of kg/m2. A data collection sheet was used to measure different variables. The participants underwent ultrasound nasal skin thickness measurement by a specialized radiologist for five different nasal points using a GE LOGIQ E9 US machine, superficial probe, frequency 9–15 Mhz (Figure 1). The 5 points are: nasion, nasal dorsum, rhinion, supratip area, and tip defining point. The nasion point defined as the most anterior point of the frontonasal suture that joins the nasal part of the frontal bone and the nasal bones. Dorsum is the midline anterior bony prominence of the nose. Rhinion is a point at the lower end of the median suture joining the nasal bones. Supra tip point is the nasal region where the inferior region of the nasal dorsum meets the tip of the nose. Tip defining point is located at the apex of the tip lobule and formed by the junction of the medial and lateral crura of each lower lateral cartilage. The measurement of the nasal tip was done by calculating the depth from the superficial skin to the dome of the lower lateral cartilage for each side then dividing by two. The data were transferred to an Excel spreadsheet with all the required variables. Data were input from the Excel spreadsheet and analyzed using R v.3.6.3. Counts and percentages were used to summarize categorical variables, and mean ± standard deviation (SD) was used for continuous variables. Linear regression analysis was used to assess the factors associated with nasal skin thickness. The models were adjusted for age and sex. Hypothesis testing was performed at the 5% significance level. Correlation between nasal skin thickness and BMI.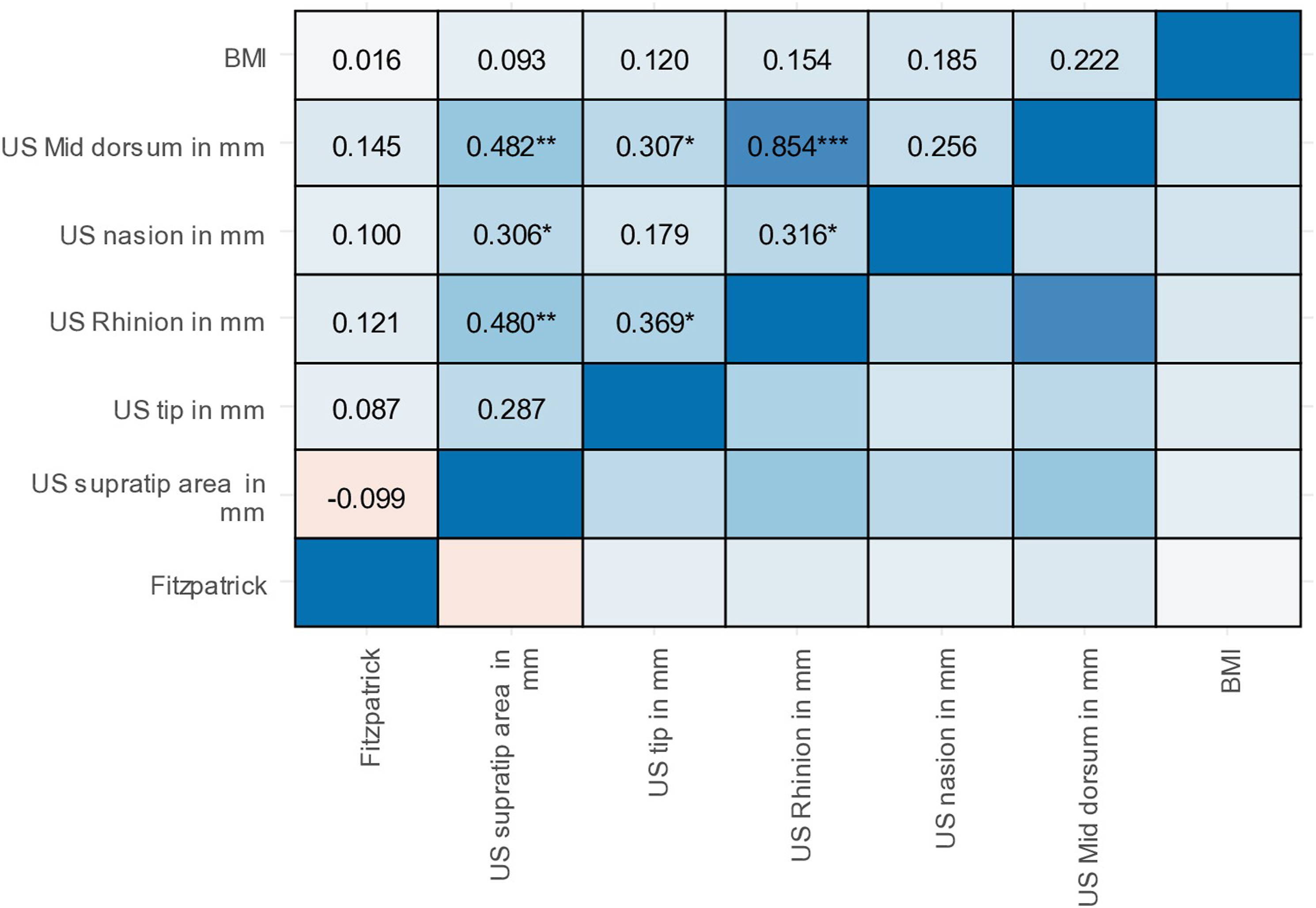
Results
Descriptive Statistics for the Study Sample.
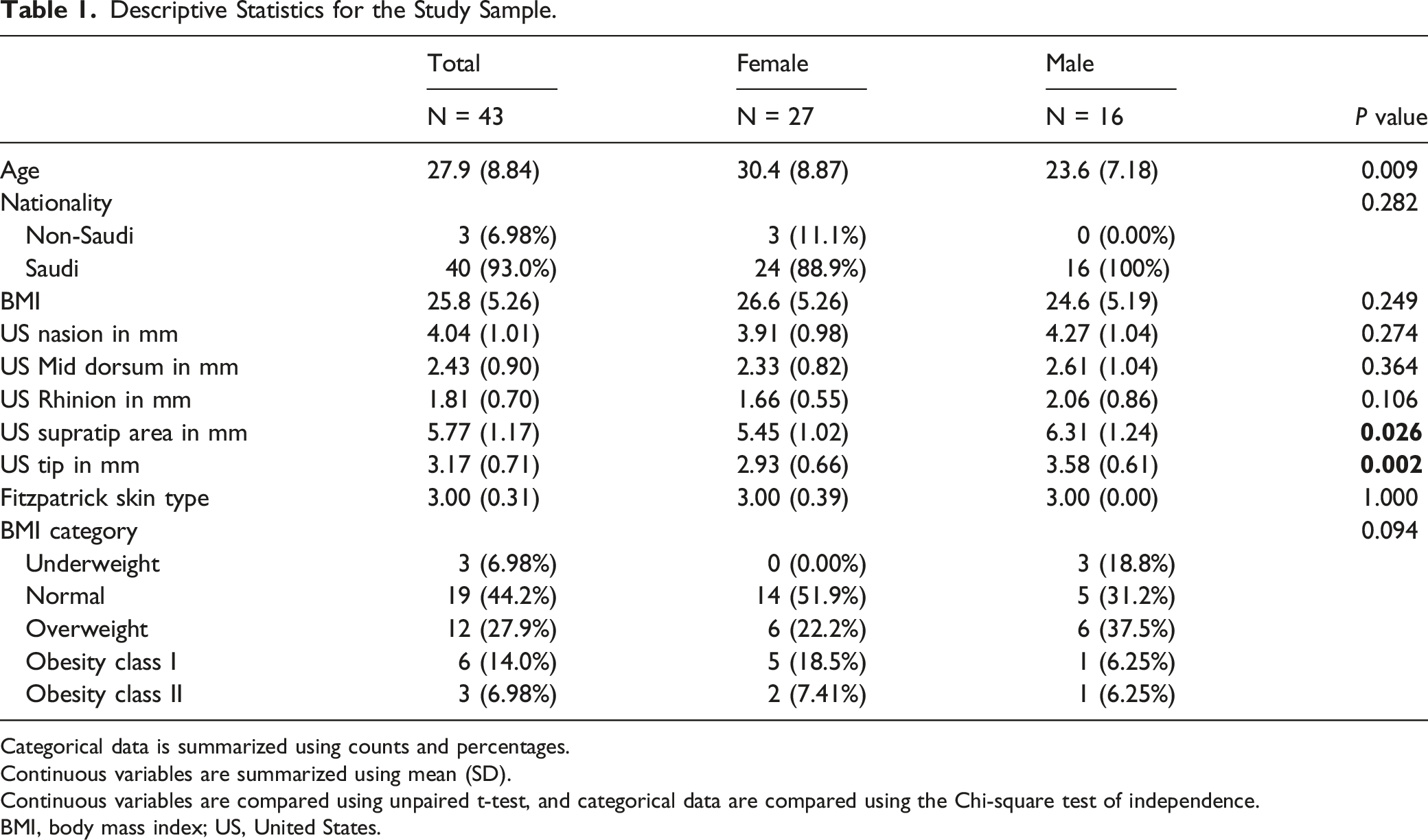
Categorical data is summarized using counts and percentages.
Continuous variables are summarized using mean (SD).
Continuous variables are compared using unpaired t-test, and categorical data are compared using the Chi-square test of independence.
BMI, body mass index; US, United States.
Association Between Body Mass Index and Nasal Mucosal Thickening.
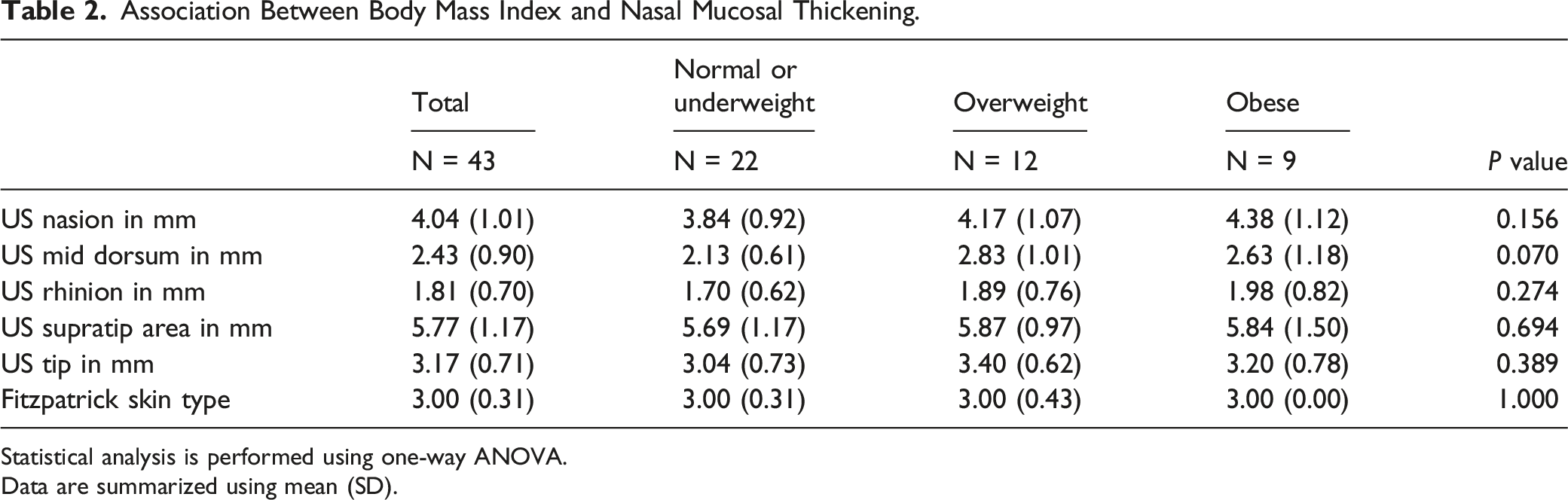
Statistical analysis is performed using one-way ANOVA.
Data are summarized using mean (SD).
Linear Regression Analysis for Middorsum and Rhinoin Areas.
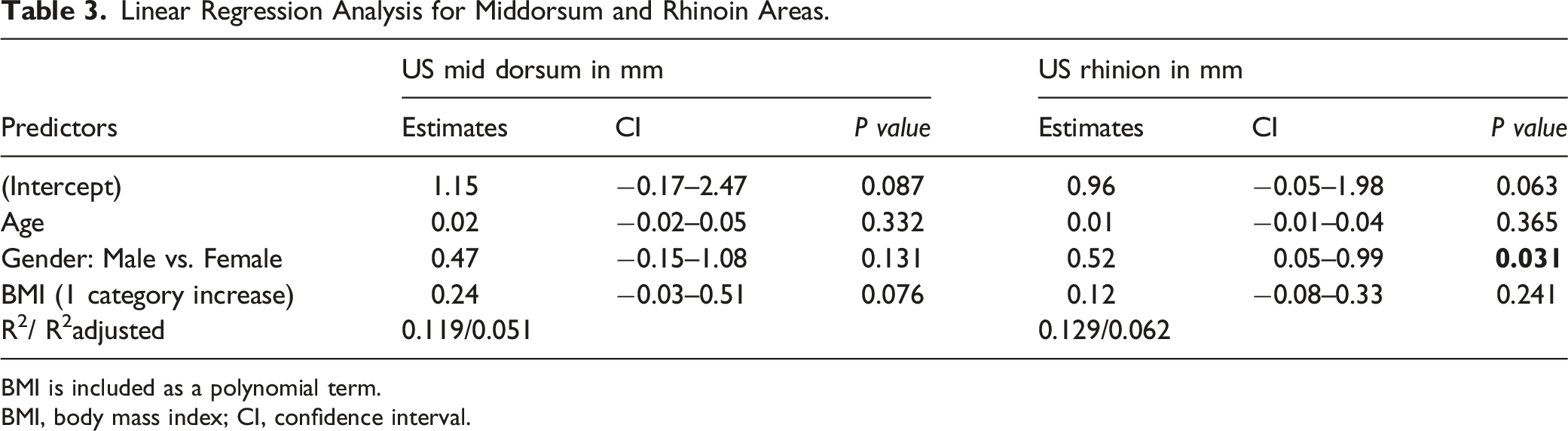
BMI is included as a polynomial term.
BMI, body mass index; CI, confidence interval.
Linear Regression Analysis for Nasion, Supratip, and Tip Areas.
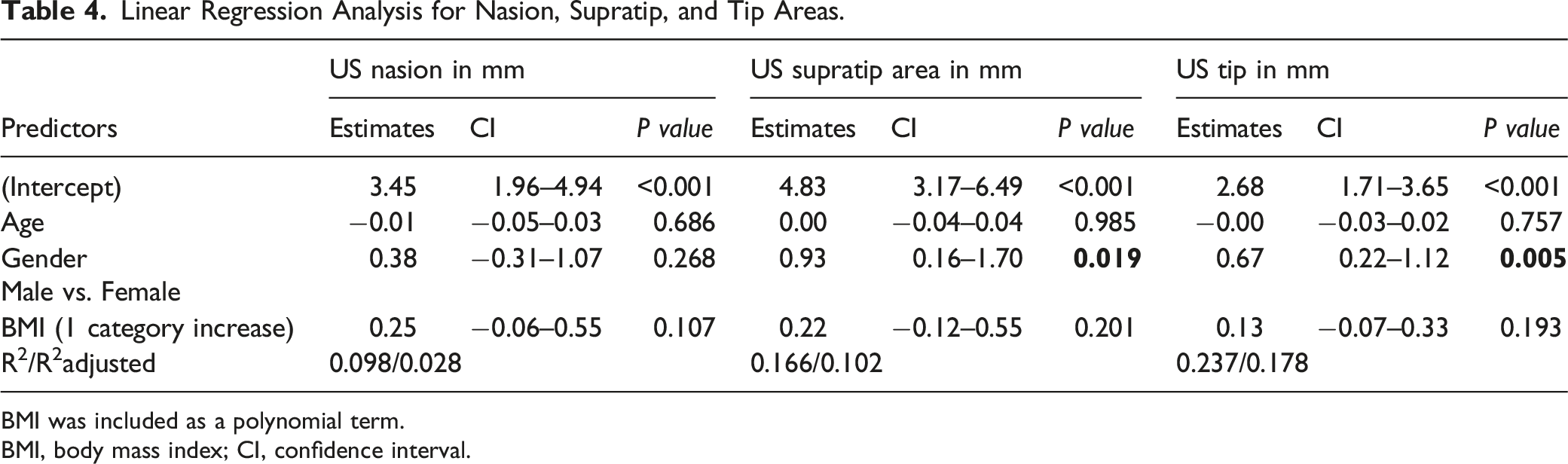
BMI was included as a polynomial term.
BMI, body mass index; CI, confidence interval.
Discussion
Our study aimed to determine the relationship between nasal skin thickness by measuring skin thickness preoperatively among rhinoplasty patients using ultrasound technique measurements and BMI. Nasal skin thickness was reported to be an important factor for rhinoplasty, interfering with intraoperative difficulty, the final result of rhinoplasty surgery, and overall satisfaction.2,4 Patients involved in the study were categorized according to their BMI into normal, overweight, and obese groups. Skin thickness measurements were performed using the US scan technique to determine the association between obesity and skin thickness. There is no standardized method for nasal skin thickness measurements. Different modalities have been used in the literature, and most rhinoplasty surgeons utilize visual inspection to assess skin thickness; 12 however, many authors have utilized CT scans in many populations.9-11 Okzul et al. 2 used the Castroviejo Caliper instrument, and showed that only sex was significantly associated with the thickness of the rhinion, supratip, and tip areas, which is consistent with the findings of Simpson and Kim et al.4,5 In addition, Jacob et al. found that the nasal soft tissue envelope was thicker in individuals with a higher BMI. 12 Similarly, facial soft tissue was thicker in the Chinese population in those with a higher BMI. 13 In addition to these findings, Alharethy et al. showed that BMI did not influence the nasal shape. 14 In our study, BMI was found to have an insignificant association with nasal skin thickness areas, including the nasion, mid dorsum, rhinion, supratip, and tip areas.
Obesity often increases subcutaneous fat. A study by Boza et al. compared the skin manifestations in obese patients with a control group of normal-weight patients. The study showed that a large number of dermatological diseases are associated with a greater extent in obese populations such as striae, pseudoacanthosis nigricans, and bacterial infections. 15 Numerous studies have detailed the effects of obesity on craniofacial measurements.6,7,16,17 Similarly, Moghadam et al. revealed a significant association between soft tissue thickness, MRI measurements, and BMI. 18
Nonetheless, few studies have been conducted to understand the relationship between BMI and nasal skin thickness and whether it can be used as a predictor of skin quality.
Alharethy et al. illustrated the CT measurements of the skin thickness at the nasion and the rhinion region of 100 patients. The study found no correlation between nasal thickness and BMI in all nasal regions. 19 However, Dey et al. described the correlation between BMI, other facial features, and nasal STE thickness in a sample size of 190 patients. They found that thick skin is more prevalent in patients with rich sebaceous skin, telangiectasias, higher Fitzpatrick skin type, male sex, and higher BMI. In contrast, thin skin is associated with increased visibility of nasal tip cartilages, freckles, lower Fitzpatrick skin type, female sex, and lower BMI. 12 Ming et al have used US technique to measure dermal and epidermal facial thickness and have found that gender had a significant impact on the thicknesses of facial dermis and epidermis of normal adults while BMI had no correlation with epidermal and dermal thicknesses which is consistent with findings of our study. 20
Small sample size is considered one of the limitations of this study and because of this to better represent the population more studies with larger sample size are needed in the future.
In conclusion, BMI was not associated with nasal skin thickness. Differences in nasal skin thickness were found between the sexes.
Footnotes
Acknowledgments
Author confirmations
Hassan Assiri: Literature review, Data collection, manuscript writing.
Waleed Abdelkader: Literature review, Imaging interpretation, manuscript writing.
Rayan Alfallaj: Literature review, result analysis, manuscript writing, submission.
Yasser Alarimah: Literature review, Data collection, manuscript writing.
Hadeel AlMajed: Literature review, Data collection, manuscript writing.
Ahmed Alarfaj: Research Idea, Literature review, manuscript writing, review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
All research data can be accessed through an excel files for review.
Ethical Approval
This research was approved by the Institutional Review Board of the research committee of at college of medicine at king Saud University program with IRB registration number: E-21-6530.
Correction (August 2023):
Hassan Assiri and Yasser Alarimah affiliation has been updated in the article.