
Abstract
Atypical Ramsay-Hunt syndrome is caused by varicella zoster viruses (VZV), without herpes, herpes is not around the ear, or posterior cranial nerve palsy is the first clinical manifestation. In this case, a 60-year-old male patient with VZV invades the branches of the vagus nerve alone. The initial symptoms were in the pharynx and larynx, which presented as mucosal ulcers and voice disorders. The ear symptoms were only otalgia and auricular herpes, without deafness, tinnitus, or peripheral facial palsy. Herpes and ulcers healed with medication, but voice disorders caused by vocal cord paralysis did not return. Voice correction treatment has been implemented to help restore the movement and closure of the vocal cords, with ultimately good results. After voice correction treatment, the patient recovered without residual nerve palsy complications. Voice correction treatment has been shown to be potentially effective and promising in shortening the recovery period and improving the recovery rate for vocal cord paralysis caused by viral infection.
Keywords
Introduction
The atypical Ramsay-Hunt syndrome caused by varicella zoster viruses (VZV) infecting the vagus nerve alone is relatively unusual. 1 Unlike the typical Ramsay-Hunt syndrome, pharynx and larynx symptoms become the primary symptoms of the patient’s complaint. The first symptom is usually a sore throat or a feeling of obstructed swallowing, and vocal cord paralysis occurs when the recurrent laryngeal nerve is invaded. Viral infection-caused vocal cord paralysis is characterized by long duration, low recovery rate, and the potential for permanent hoarseness and susceptibility to aspiration pneumonia.2,3 However, the patient reported below with an isolated VZV invasion of the vagus nerve recovered within one month of voice correction treatment, and no recurrence throughout the more than 1.5-year follow-up period.
Case report
A 60-year-old man sought treatment for sore throat, difficulty swallowing for eight days, and hoarseness accompanied by choking on water for five days. At the local hospital, medication was administered but symptoms did not alleviate. On admission, multiple ulcers in the right lingual-palatal arch; congestion, edema, and mucosal ulcers in the right aryepiglottic fold and epiglottis; fixation of the right aryepiglottic fold and right vocal cord; and fluid in the right pyriform fossa (Figure 1). Laryngoscopy before treatment: 2021-06-19 Fiberoptic laryngoscopy reveals multiple ulcers in the right lingual-palatal arch; congestion, edema, and multiple mucosal ulcers in the right aryepiglottic fold and epiglottis; fixation of the right aryepiglottic fold and the right vocal cord, and inadequate closure of the vocal cords; and fluid in the right pyriform fossa. (1A: open phase of the vocal cords; 1B: closed phase of the vocal cords).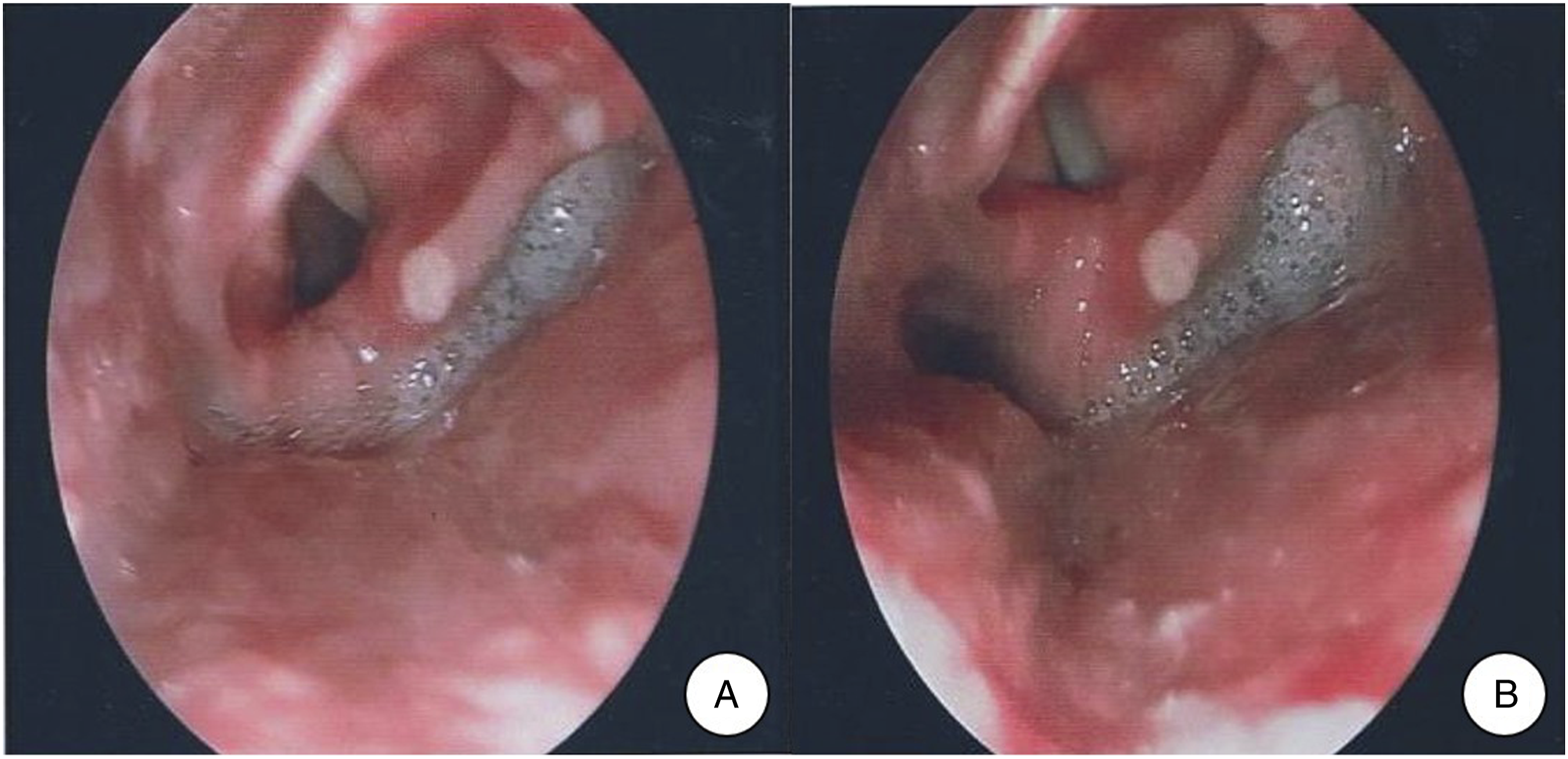
Before admission, CT scans of the head, neck, and chest and thyroid ultrasound were performed, and no substantial lesions were identified. Therefore, tumors were ruled out first and idiopathic paralysis of the vocal cord combined with pharyngeal mucosal ulcers was considered the most likely diagnosis. However, specific infections, such as fungal infections or tuberculosis, and rheumatic immune diseases such as Behcet’s disease could not be completely excluded. On admission day, therapeutic measures, including intravenous methylprednisolone and clindamycin, nebulized inhalation with budesonide suspension, and rehydration support therapy, were administered. Blood routine, C-reactive protein, calcitoninogen, erythrocyte sedimentation rate, mycobacterium tuberculosis, bacterial culture, fungal smear, biochemistry, hepatitis C virus antibody, anti-HIV antibody, syphilis spirochete antibody, autoantibodies, humoral immune function, immunoglobulin G4, and antineutrophil antibodies and subtypes were also performed, but no significant abnormal results were found. However, the patient presented pain in the right ear and auricular herpes on the second day of hospitalization, so we hypothesized Ramsay-Hunt syndrome and prescribed intravenous acyclovir, intramuscular mecobalamin, and wet compression of the ear with compound cypress oil solution, along with continued antibiotics, hormones, nebulization, and rehydration support.
The sore throat, otalgia, and swallowing obstruction resolved, while the auricular herpes subsided and gradually crusted after five days of medication. But there were no noticeable improvements in hoarseness and choking cough. There was no edema or ulcers in the pharyngeal mucosa on fiberoptic laryngoscopy. However, the right vocal cord remained immobile and the right pyriform fossa was covered with secretions (Figures 2A-B). Voice Handicap Index (VHI) score 97, the grade, roughness, breathiness, asthenia, strain (GRBAS) scale score was G3R3B3A2S1, fundamental frequency (F0): 72.3 Hz, jitter: 8.43%, Maximum Phonation Time (MPT): 7.9 s, Dysphonia Severity Index (DSI): −6.33. Subsequently, with the patient’s consent, he received voice correction treatment to promote movement and closure of the vocal cords, including coordination between breathing and articulation, interrupted breathing, coughing and humming, articulatory strength training, etc., and continued to take methylcobalamine to nourish the nerves, and Ginkgo biloba leaf to improve blood circulation. Throughout treatment, hoarseness and choking cough gradually decreased and his voice returned to normal with no choking cough a month later. VHI score 11. GRBAS score G0R0B1A1S0. F0: 160.7 Hz, jitter: 0.27%, MPT: 16.1 s, DSI: 1.97. Fiberoptic laryngoscopy revealed smooth pharyngeal mucosa, no edema or ulcers, normal movement of the bilateral vocal cords, and adequate closure of the vocal cords (Figures 2C-D). During the 1.5-year follow-up, there was no recurrence of throat and voice discomfort. Laryngoscope after treatment: 2A-B: 2021-06-26 Fiberoptic laryngoscopy shows smooth pharyngeal mucosa with no obvious edema or ulcers, fixation of the right aryepiglottic fold and the right vocal cord, and incomplete closure of vocal cords. The pyriform fossa is covered with secretions. (2A: open phase of the vocal cords; 2B: closed phase of the vocal cords). 2C-D: 2021-07-31 Fiberoptic laryngoscopy shows smooth pharyngeal mucosa with no edema or ulcers, normal movement of the bilateral vocal cords, and adequate closure of the vocal cords. (2C: open phase of the vocal cords; 2D: closed phase of the vocal cords).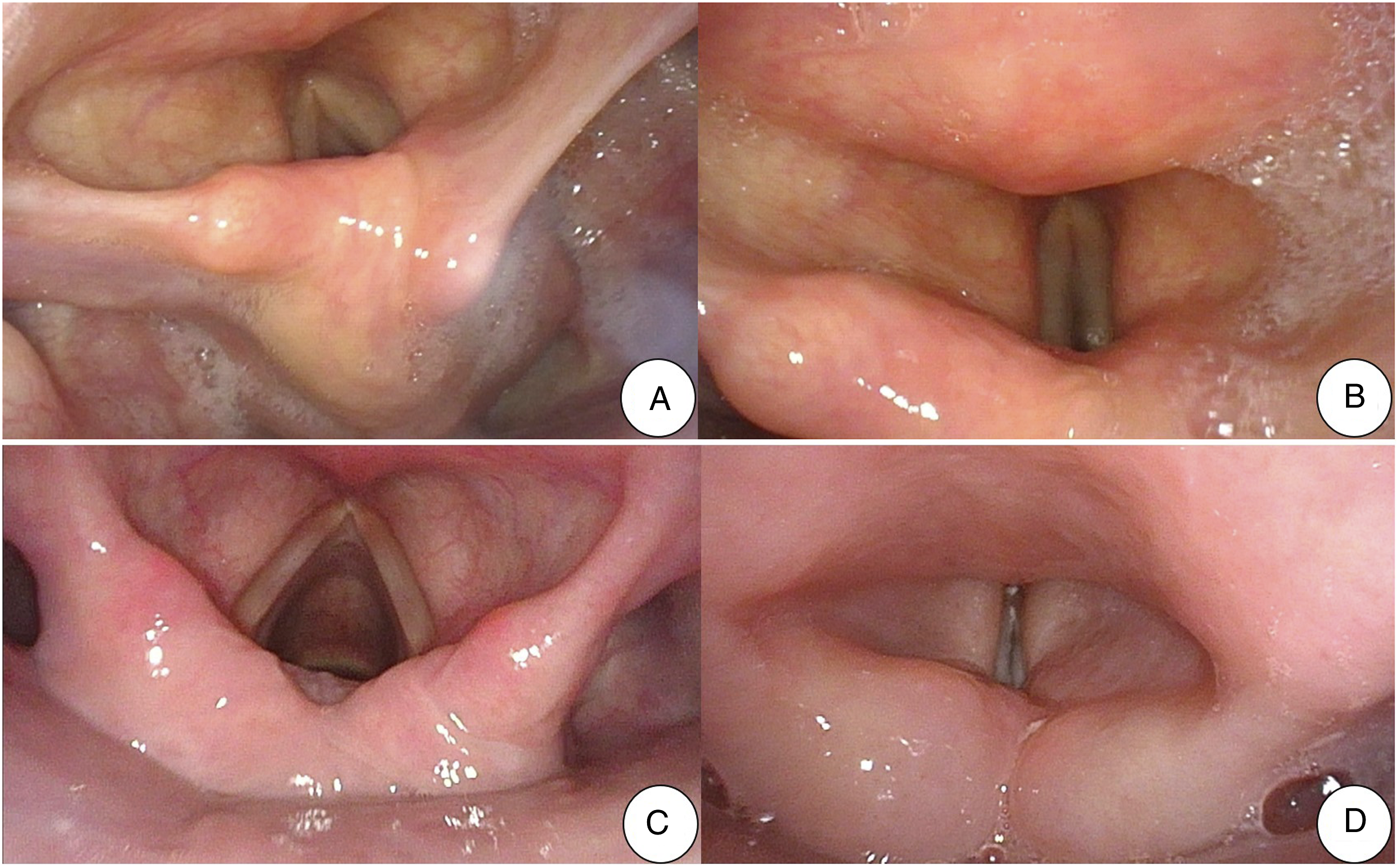
Discussion
Ramsay-Hunt syndrome, first reported by Ramsay Hunt in 1907, 4 has the “three main signs” of otalgia, peri-auricular herpes, and peripheral facial palsy, with peri-auricular herpes being the main diagnostic basis, so the disease is also known as ear herpes zoster. 5 However, there are a few patients who present without herpes or whose herpes is not peri-auricular, or who have posterior cranial nerve palsy as their first clinical manifestation, which is called atypical Ramsay-Hunt syndrome. 6 Ramsay-Hunt syndrome is caused by the reactivation of VZV, which are neurophilic and become latent in the geniculate ganglion following infection; it reactivates when provoked by exertion or cold and invades the nerve. Among them, the probability of invasion of the facial nerve is the highest, up to 93.8%, and the probability of invasion of the vagus nerve is the lowest, only 2.4%. 1
Treatment for Ramsay-Hunt syndrome aims to alleviate discomfort during the acute phase, shorten the duration of the lesions, prevent their spread, and avoid or mitigate consequences. 7 Virus-caused vocal cord paralysis is characterized by a prolonged course and low recovery rate, typically taking 2–3 months of treatment to begin to show signs of recovery, 2 and 40% of patients cannot fully recover. 3 In this case, the medication only cured some of the symptoms, including pharyngeal ulcers and ear herpes, but did not affect hoarseness and choking cough. In addition to the presentation on the laryngoscope, significant abnormalities were found in the voice assessment indicators. High scores on GRBAS and VHI before voice correction treatment subjectively indicate poor voice quality, which interferes with daily life.8,9 Shortening MPT, increased jitter, reduced F0, and abnormal DSI objectively reflect poor closure of the vocal cords and severity of voice disorders.10 –13
We tried to use a four-step training method for voice correction treatment and developed an individualized program based on the condition of the patient, which includes relaxation training, breathing training, vocalization training, and resonance training. 14 The principle of treatment is to increase the strength of the vocal cords on the one hand and work on the balance of the laryngeal muscles on the other. Relaxation training focuses on muscle relaxation through laryngeal massage and relaxation exercises for the laryngeal muscles. Breathing training includes abdominal breathing, blowpipe, and “dog panting” to train the patient to breathe in the most appropriate way to support vocalization. Vocalization training includes /hou/ sound training, yawning and sighing, semi-swallowing “boom” sounds, bubble sounds, interrupted breathing training, matching breathing with articulation, coughing and grunting training, and articulatory strength training. These exercises promote the closure of the vocal cords by increasing the tension of the vocal cords, assisting the movements of the cricoarytenoid joints, and increasing the vibration of the mucous membrane at the edge of the vocal cords. In resonance training, tone extension training lengthens the vocal cords and increases the tension of the vocal cords. Vapor flute training not only helps the patient learn to control the cricothyroid gap, which produces smooth changes in volume during the vibration of the vocal cords and reduces the thickness of the vocal cords, but also promotes flexibility in vertical laryngeal changes. 15 Voice correction treatment not only promotes the movement of the cricoarytenoid joints, improves the closure of the vocal cords, increases the movement of the vocal cords and enhances articulation, but also elevates the larynx, elevates the arytenoid muscles, promotes internal retraction and vibration of the arytenoid muscles, thus promoting the symmetric movement of the bilateral cricoarytenoid joints, which helps to increase the mobility of the joints and improve vocalization.
Patients learn the techniques from the professional voice therapist and then practice them at home. During the exercises, hoarseness gradually decreased, and the voice returned to normal after a month of voice correction treatment. On laryngoscopy, normal movements and adequate closure of the bilateral vocal cords were observed. The appreciable reduction in GRBAS and VHI scores, the prolongation of MPT, the decrease in jetter, and the general return of F0 and DSI to the normal range suggest a significant improvement in voice quality. The above results suggest that voice correction treatment is potentially effective and promising in shortening the recovery period and improving the recovery rate for vocal cord paralysis caused by viral infection.
Footnotes
Acknowledgments
Not applicable.
Contributions of the authors
Lei Dong and Xiumei Chen were the treating doctors in this case and administered medication and voice correction treatment; Lei Dong conceived the study, performed data analyses, and wrote the manuscript; Xicheng Song and Xiumei Chen contributed significantly to the interpretation of the data and performed the analysis with constructive discussions. Xicheng Song approved the final version. Xicheng Song agreed to be responsible for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors critically reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
All therapeutic options were approved by the Ethics Committee of Yuhuangding Hospital and all medical records were obtained with the consent of the patient.
Consent for publication
Before obtaining the original data and writing the article, informed consent was obtained from the patient.
Availability of data and materials
Not applicable.